Masterclass in Replantation Surgery: Preoperative Preparation and Sequential Repair Techniques
Key Takeaway
Successful replantation of amputated digits and limbs demands meticulous ex vivo preparation, precise microsurgical dissection, and a strict, biomechanically sound order of repair. This guide details the critical steps from initial stump debridement and bone shortening to neurovascular anastomosis. Emphasizing tension-free repairs and strategic sequencing, these evidence-based protocols are designed to maximize tissue viability, restore functional anatomy, and optimize postoperative recovery for complex amputation injuries.
Comprehensive Introduction and Patho-Epidemiology
The successful replantation of amputated digits, hands, and upper extremities represents one of the most demanding and sophisticated challenges in operative orthopedics, traumatology, and reconstructive microsurgery. Achieving not merely tissue survival, but meaningful, durable functional recovery, requires a profound understanding of vascular anatomy, biomechanics, and meticulous surgical sequencing. Since the first successful human limb replantation by Malt and McKhann in 1962, and the first successful microvascular digital replantation by Komatsu and Tamai in 1968, the field has evolved from a focus on mere viability to a rigorous pursuit of maximal functional restoration. The preparation phase—encompassing patient optimization, ex vivo dissection of the amputated part, and proximal stump management—dictates the trajectory of the entire procedure and ultimately determines the functional fate of the replanted appendage.
Epidemiologically, traumatic upper extremity amputations occur most frequently in young, working-age males, typically secondary to industrial accidents, agricultural machinery injuries, or high-energy power tool trauma. The mechanism of injury is the single most critical determinant of both the technical feasibility of replantation and the ultimate prognosis. Sharp, guillotine-type amputations (e.g., from a paper cutter, machete, or table saw) inflict a minimal zone of injury, preserving the microvascular architecture proximal and distal to the amputation plane, thereby yielding the highest success rates. Conversely, crush and avulsion injuries (e.g., from punch presses, rotating gears, or agricultural PTO shafts) impart a massive, diffuse zone of trauma. These mechanisms cause extensive endothelial damage, intimal disruption, and multilevel skip lesions that severely complicate microvascular reconstruction and drastically increase the risk of postoperative thrombosis.
The pathophysiology of the amputated part is dominated by the ischemia-reperfusion (I/R) injury cascade. During the ischemic phase, the depletion of cellular adenosine triphosphate (ATP) leads to the failure of the sodium-potassium ATPase pump, resulting in intracellular sodium accumulation, cellular swelling, and microvascular luminal narrowing. Simultaneously, anaerobic metabolism generates toxic accumulations of lactic acid and hypoxanthine. Upon the restoration of arterial inflow (reperfusion), the sudden influx of oxygen interacts with hypoxanthine and xanthine oxidase to generate massive quantities of reactive oxygen species (ROS), including superoxide anions and hydroxyl radicals.
These free radicals initiate lipid peroxidation of cell membranes, leading to profound endothelial injury, increased microvascular permeability, and the expression of adhesion molecules (e.g., ICAM-1, P-selectin). This cascade promotes leukocyte sequestration, platelet aggregation, and the formation of microthrombi, culminating in the "no-reflow phenomenon"—a catastrophic state where, despite a technically patent macrovascular anastomosis, the microcirculatory bed remains occluded, leading to inevitable graft necrosis. Understanding this biochemical cascade is fundamental to the rationale behind hypothermic preservation, ex vivo perfusion, and the administration of systemic rheologic agents during the perioperative period.
Detailed Surgical Anatomy and Biomechanics
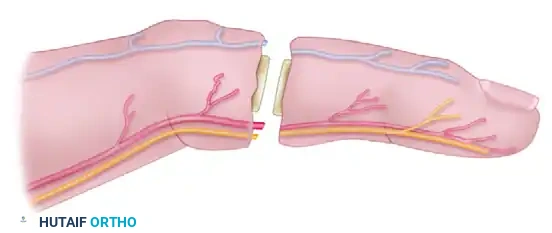
A masterful command of upper extremity vascular and neural anatomy is an absolute prerequisite for any surgeon undertaking replantation. The arterial supply to the hand is derived from the complex anastomotic networks of the superficial and deep palmar arches, which are fed by the radial and ulnar arteries. The superficial palmar arch, predominantly supplied by the ulnar artery, gives rise to the common digital arteries. At the level of the metacarpal heads (web spaces), these common digital arteries bifurcate into the proper digital arteries, which travel along the volar-radial and volar-ulnar aspects of the digits, volar to the digital nerves.
The proper digital arteries are consistently located just volar to the mid-axial line of the digit. At the level of the proximal interphalangeal (PIP) joint, the external diameter of a proper digital artery typically ranges from 0.8 to 1.2 mm, demanding the use of operating microscopes and ultrafine (9-0 to 11-0) monofilament sutures. The arterial anatomy of the thumb is uniquely complex, supplied by the princeps pollicis artery, which arises from the deep palmar arch and bifurcates at the metacarpophalangeal (MCP) joint into the radial and ulnar proper digital arteries. In distal thumb amputations, the arborization of these vessels requires meticulous dissection to identify terminal branches suitable for microvascular anastomosis.
Venous drainage of the digits and hand is overwhelmingly dorsal, a critical biomechanical and anatomical fact that dictates surgical sequencing. The volar venous system is negligible in its contribution to outflow. The dorsal venous network originates from the nail bed and paronychial regions, coalescing into larger, thin-walled dorsal veins that travel in the loose areolar tissue superficial to the extensor paratenon. These veins are incredibly fragile, highly susceptible to desiccation and crush injury, and lack the robust muscularis layer found in arteries. Identifying and mobilizing these veins without inducing adventitial stripping or intimal damage is one of the most technically demanding aspects of the ex vivo preparation.
Neurologically, the proper digital nerves run dorsal to the proper digital arteries in the proximal palm but cross to become volar to the arteries within the digits. They are accompanied by tiny venae comitantes. The biomechanics of the flexor and extensor tendon systems also play a pivotal role in replantation planning. Amputations through "Zone II" (no man's land) involve both the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) within a tight fibro-osseous sheath. Repairing both tendons in the setting of a replantation can lead to massive scarring and a stiff, non-functional digit; therefore, many surgeons opt to repair only the FDP or perform a delayed flexor tendon reconstruction depending on the extent of the soft tissue crush and contamination.
Exhaustive Indications and Contraindications
The decision to proceed with replantation requires a complex calculus balancing the technical feasibility of the microvascular repair, the anticipated functional outcome, the patient's physiological reserve, and the socioeconomic impact of the injury. The overarching philosophy of replantation surgery is that a successfully replanted part must offer superior function and aesthetics compared to a well-constructed amputation stump or a prosthetic device.
Absolute indications for replantation are well-established and encompass scenarios where the loss of the amputated part would result in devastating functional impairment. The thumb is the cornerstone of hand function, contributing to approximately 40% to 50% of overall hand capability through pinch and grasp mechanics; therefore, thumb amputations at almost any level are an absolute indication for replantation attempts. Similarly, multiple digit amputations require replantation to restore basic prehensile function. In the pediatric population, the remarkable capacity for nerve regeneration and cerebral plasticity makes replantation an absolute indication for almost all amputated parts, as functional outcomes significantly surpass those seen in adults.
Conversely, absolute contraindications are dictated by the "life over limb" principle. Replantation must never compromise the patient's survival. Hemodynamic instability, severe concomitant life-threatening injuries (e.g., traumatic brain injury, major thoracic or abdominal trauma), and profound systemic comorbidities (e.g., severe end-stage renal disease, advanced peripheral vascular disease) preclude prolonged microvascular procedures. Furthermore, amputated parts that have sustained massive, multilevel crush injuries, severe segmental avulsions, or prolonged warm ischemia times (generally >12 hours for digits, >6 hours for major muscle-containing parts) are considered non-viable due to irreversible myonecrosis and the high risk of fatal reperfusion syndrome.
Indications and Contraindications Matrix
| Category | Absolute Parameters | Relative Parameters |
|---|---|---|
| Indications | • Thumb amputations at any level • Multiple digit amputations • Any amputation in children • Amputations through the wrist or forearm (sharp) |
• Single digit amputation distal to FDS insertion (Zone I) • Ring avulsion injuries (Urbaniak Class II) • Clean, sharp amputations in young, healthy adults |
| Contraindications | • Concomitant life-threatening injuries • Severe, multilevel crush/segmental injuries • Prolonged warm ischemia (>12h digits, >6h proximal) • Severe psychiatric illness or self-inflicted amputation |
• Single digit amputation in Zone II (adults) • Extreme age with significant medical comorbidities • Avulsion injuries with extensive intimal damage • Heavy tobacco use or non-compliance |
Relative indications and contraindications require highly individualized surgical judgment. The classic debate surrounds the single-digit amputation in Zone II in an adult. Historically considered a relative contraindication due to the high likelihood of a stiff, painful digit that bypasses functional use, modern microsurgical techniques and aggressive hand therapy have led many centers to offer replantation for specific patients, particularly musicians, surgeons, or those with strong aesthetic demands. However, the patient must be extensively counseled that a stiff, cold-intolerant replanted digit may ultimately require a secondary amputation if it interferes with global hand function.
Pre-Operative Planning, Templating, and Patient Positioning
The physiological optimization of the patient and the meticulous management of the surgical environment are paramount. Replantation is often a marathon procedure, frequently lasting between 6 to 18 hours depending on the number of digits involved. This necessitates rigorous, proactive attention to patient comfort, core temperature maintenance, deep vein thrombosis (DVT) prophylaxis, and continuous hemodynamic stability.
The handling of the amputated part prior to arrival in the operating room is a critical determinant of success. The amputated part must be gently cleansed of gross debris with sterile saline, wrapped in saline-moistened gauze, and placed inside a sealed, watertight plastic bag. This bag is then immersed in an ice-water slurry. This method achieves an optimal hypothermic state of approximately 4°C, which drastically reduces cellular metabolism and extends the allowable ischemia time. Crucially, the amputated part must never be placed directly on ice or submerged in dry ice, as this will induce irreversible cellular frostbite and tissue necrosis, rendering replantation impossible.
Anesthetic Considerations and Sympathetic Blockade
The choice of anesthesia profoundly impacts both intraoperative hemodynamics and postoperative graft survival. For most adults and older children undergoing digital or hand replantation, a continuous regional anesthetic technique, such as an axillary or supraclavicular brachial plexus block utilizing a long-acting local anesthetic (e.g., bupivacaine or ropivacaine), is the gold standard. Beyond providing excellent intraoperative and postoperative analgesia, regional blocks induce a profound sympathetic blockade. This pharmacological sympathectomy results in sustained peripheral vasodilation, maximizing arterial inflow, mitigating microvascular vasospasm at the anastomotic sites, and expanding the microcirculatory bed.
General anesthesia is frequently preferable, and often mandatory, for proximal amputations (forearm and arm level) where major muscle mass is involved, in younger or highly anxious children, or during extraordinarily prolonged surgeries involving multiple digits or bilateral amputations where tourniquet tolerance and decubitus complications become significant concerns. In cases requiring general anesthesia, core temperature management becomes even more critical, as volatile anesthetics can impair central thermoregulation.
Patient Positioning and Environmental Control
Hypothermia is a potent, systemic trigger for peripheral vasoconstriction, which can be catastrophic for microvascular anastomoses. The operating room ambient temperature should be elevated, and the operating table must be heavily padded with gel matrices to prevent pressure-induced neuropathies or decubitus ulcers during the prolonged case. Forced-air warming blankets (e.g., Bair Hugger) must be applied to all non-operative body surface areas, and intravenous fluids should be administered through an in-line fluid warmer to maintain strict normothermia (core temperature >37°C) throughout the surgical duration.
A pneumatic tourniquet is essential to provide a bloodless field during the initial dissection of the proximal stump and to control subsequent significant bleeding during bone preparation. The tourniquet should be heavily padded with cast padding and applied high on the arm. Once the patient is anesthetized and comfortable, the proximal stump is thoroughly cleansed with a surgical antiseptic solution (typically povidone-iodine or chlorhexidine, though chlorhexidine must be strictly avoided near exposed peripheral nerves due to its severe neurotoxicity). The stump is then meticulously irrigated with copious volumes of warmed normal saline to remove gross contaminants and dilute bacterial loads before formal surgical debridement under magnification begins.
Step-by-Step Surgical Approach and Fixation Technique
While the patient is being prepped and anesthetized, a second surgical team—led by a hand surgeon with advanced microsurgical training—simultaneously prepares the amputated part on a sterile back table. This ex vivo dissection is a critical, time-saving maneuver that minimizes warm ischemia time once the part is brought to the surgical field. The approach to the structures of the amputated part must allow for extensive, atraumatic exposure.
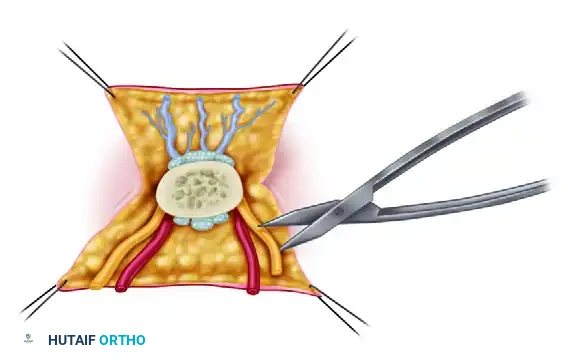
Ex Vivo Dissection and Structural Tagging
Mid-axial incisions on the radial and ulnar aspects of the digit are the standard approach. These incisions allow for the reflection of full-thickness dorsal and palmar flaps, providing panoramic, 360-degree access to the neurovascular bundles, flexor tendon sheath, and extensor mechanism.
Using magnifying loupes (minimum 4.5x) or an operating microscope, the surgeon employs meticulous, no-touch technique to identify the arteries, veins, and nerves. Small structures are highly susceptible to retraction and loss within the edematous soft tissue planes. They must be carefully preserved and tagged with 8-0 or 9-0 nylon epineurial or adventitial sutures. This ensures they can be rapidly located for nerve repair and vascular anastomoses later in the procedure. Tendons are dissected, their ends freshened, and secured with 4-0 nylon core sutures.
During vascular assessment, crush and avulsion injuries present a much wider zone of trauma. Evidence of distal injury may manifest as ecchymoses along the neurovascular bundles, adventitial abrasions, or skip lacerations.
In these complex scenarios, the vascular tree must be interrogated and cleared. The surgeon gently cannulates the digital artery using a small Silastic catheter and perfuses the vascular tree with a heparinized Ringer's lactate or normal saline solution (typically 100 units of heparin per mL). If there is no return of the perfusate from the dorsal veins, or if the fluid extravasates from distally injured vessels, the microvascular bed is likely destroyed, and replantation may be contraindicated.
The Standardized Order of Repair
After all structures in both the amputated part and the proximal stump have been thoroughly cleansed, aggressively debrided of all necrotic tissue, and clearly identified, the formal repair begins. The universally accepted, biomechanically optimized order of repair is designed to provide skeletal stability first, followed by sequential soft tissue and neurovascular reconstruction.
1. Bone Shortening and Osteosynthesis:
Bone shortening is the foundational, non-negotiable step of replantation. It is an absolute prerequisite for achieving tension-free vascular and neural anastomoses. Attempting to stretch a microvascular repair across a gap will inevitably result in vasospasm, intimal tearing, and thrombosis. Shortening is usually performed on the side of the amputation that has the most bone to spare, typically resecting 0.5 to 1.0 cm of bone using an oscillating saw under continuous saline irrigation to prevent thermal necrosis. Rigid, low-profile internal fixation is required. We typically insert a longitudinal Kirschner wire (K-wire) combined with an obliquely crossing K-wire to provide rotational stability. Intraosseous wiring (90-90 wiring) is highly effective near metaphyseal regions. Plates and screws are generally avoided in digital replantation due to their bulk, which can compromise soft tissue closure and impinge on the delicate vascular repairs.
2. Extensor Tendon Repair:
Repairing the extensor tendons immediately after osteosynthesis provides a secondary layer of stability to the skeletal fixation. It is performed using non-absorbable sutures (e.g., 4-0 or 5-0 core sutures) utilizing a figure-of-eight, modified Kessler, or mattress technique. Repairing the dorsal structures first prevents the need to continuously flip the hand later, which could jeopardize delicate volar vascular repairs.
3. Flexor Tendon Repair:
Flexor tendon repair follows the extensor repair. A robust core suture (e.g., 4-strand or 6-strand repair) is placed in the FDP, followed by a meticulous epitendinous repair to ensure smooth gliding within the sheath. In cases of severe crush injury or massive contamination where establishing blood flow is the overriding priority, flexor tendon repair may be intentionally delayed and performed as a secondary reconstructive procedure (e.g., Hunter rod staging) weeks later.
4. Arterial Anastomosis:
Establishing arterial inflow is the most critical step for tissue survival. Before initiating reattachment, the proximal arterial stumps must be freed of any intraluminal clots. The tourniquet is temporarily deflated to assess pulsatile flow. The stumps are opened to allow free arterial bleeding, which flushes out microthrombi. If satisfactory, brisk, pulsatile flow cannot be achieved, the vessel is likely suffering from intimal damage or severe vasospasm. Additional proximal dissection and aggressive vessel resection back to healthy, uninjured intima under the microscope is mandatory. The anastomosis is performed using 9-0 or 10-0 nylon sutures on a spatulated needle, utilizing a triangulation or back-walling technique to ensure perfect intima-to-intima coaptation. If resection results in a gap, interpositional reversed vein grafts (typically harvested from the volar forearm or dorsal foot) must be utilized.
5. Nerve Repair:
Primary neurorrhaphy is performed using 8-0 or 9-0 nylon epineurial sutures. If ischemia time permits, it is often technically easier to repair the digital nerves just before repairing the digital arteries. The nerves lie deep to the arteries in the volar surgical field; repairing them first prevents the surgeon from having to manipulate, retract, or traumatize the newly anastomosed, highly fragile artery to access the nerve.
6. Venous Anastomosis:
Venous outflow must be established to prevent catastrophic venous congestion. A general rule is to repair two veins for every one artery anastomosed, if anatomically feasible. Many microsurgeons prefer the "Dorsal First" approach: repairing the veins immediately after the extensor tendon repair (Step 2). This allows all dorsal work to be completed in a bloodless field before the hand is supinated to address the volar structures, minimizing repositioning and protecting the venous anastomoses from mechanical disruption.
7. Soft Tissue Coverage and Wound Closure:
The final step is meticulous, tension-free wound closure. In major limb replantations, or digits with significant crush components, prophylactic fasciotomies (e.g., carpal tunnel release, forearm fasciotomies) are highly recommended to prevent compartment syndrome secondary to reperfusion edema. Skin must never be closed under tension over vascular repairs. If primary closure is not possible, split-thickness skin grafts, local rotational flaps, or dermal regeneration templates should be employed immediately to cover exposed vessels and nerves.
Complications, Incidence Rates, and Salvage Management
Despite flawless surgical technique, the replanted part remains highly vulnerable in the immediate postoperative period. Complications can be broadly categorized into early (vascular) and late (functional/structural) failures. The most devastating early complication is vascular occlusion, which typically occurs within the first 48 to 72 hours.
Arterial thrombosis presents as a "white digit"—the replanted part becomes pale, cool to the touch, loses tissue turgor, and exhibits absent capillary refill. Venous congestion, conversely, presents as a "blue digit"—the part becomes swollen, cyanotic, engorged, and exhibits a rapid, dark capillary refill. Both scenarios require immediate, aggressive intervention. Time is tissue; a delay in recognizing and treating vascular compromise is the most common cause of preventable replant failure.
If vascular compromise is suspected, the initial salvage management involves removing all constrictive dressings, ensuring the patient is warm and adequately hydrated, and placing the limb in a dependent position (for arterial insufficiency) or elevating it (for venous congestion). Pharmacological interventions, such as adjusting heparin drips, administering chlorpromazine for vasospasm, or performing a stellate ganglion block, may be attempted. However, if clinical improvement is not immediate, the patient must be rushed back to the operating theater for anastomotic exploration and revision.
Complications and Salvage Management Matrix
| Complication | Estimated Incidence | Clinical Presentation | Salvage Management & Protocols |
|---|---|---|---|
| Arterial Thrombosis | 10% - 15% | Pale, cool digit, absent turgor, no capillary refill ("White Digit"). Usually occurs <24h post-op. | Immediate surgical re-exploration. Resection of thrombosed segment, thrombectomy, and interpositional vein grafting. |
| Venous Congestion | 15% - 25% | Cyanotic, swollen, purple/blue digit, brisk dark capillary refill ("Blue Digit"). Usually occurs 48-72h. | Suture removal, nail bed bleeding via heparin pledgets. Application of medicinal leeches (Hirudo medicinalis). |
| Infection | 5% - 10% | Erythema, purulent drainage, systemic fever, escalating pain. | Aggressive surgical debridement, hardware removal if loose, targeted IV antibiotics. Prophylaxis for Aeromonas if leeches used. |
| Nonunion / Malunion | 10% - 20% | Persistent pain at osteosynthesis site, radiographic evidence of failed bridging. | Late bone grafting, revision internal fixation, or arthrodesis once vascularity is completely stable (>3 months). |
| Cold Intolerance | >80% | Severe pain, blanching, and stiffness upon exposure to cold environments. | Conservative management (gloves, biofeedback). Often improves spontaneously over 2-3 years as sympathetic reinnervation occurs. |
When venous congestion cannot be surgically revised (e.g., due to a lack of suitable dorsal veins), medicinal leeches (Hirudo medicinalis) are an invaluable salvage tool. Leeches secrete hirudin, a potent direct thrombin inhibitor, and actively decongest the digit through feeding and subsequent prolonged bleeding from the bite site. When utilizing leech therapy, it is absolutely critical to administer prophylactic antibiotics (typically a fluoroquinolone like Ciprofloxacin, or Trimethoprim-Sulfamethoxazole) to prevent infection by Aeromonas hydrophila, a symbiotic bacterium residing in the leech's gut that can cause devastating, rapidly progressive tissue necrosis in the human host.
Phased Post-Operative Rehabilitation Protocols
The success of a replantation extends far beyond the operating room; it is heavily reliant on a rigorous, highly specialized postoperative monitoring and rehabilitation protocol. The patient is typically admitted to a specialized microsurgical intensive care unit or a dedicated step-down ward. The ambient room temperature must be maintained at a warm, constant level (typically >75°F or 24°C) to prevent environmental vasoconstriction. Strict prohibitions are placed on smoking, secondary smoke exposure, caffeine, and chocolate, as nicotine and methylxanthines are potent peripheral vasoconstrictors that can rapidly induce anastomotic thrombosis.
Continuous or hourly monitoring of the replanted part is mandatory for the first 48 to 72 hours. Clinical assessment remains the gold standard, focusing on skin color, capillary refill time, tissue turgor, and temperature. Surface temperature probes are highly sensitive indicators of vascular status; a sudden drop of >2°C compared to an adjacent normal control digit, or an absolute temperature falling below 30°C, is highly indicative of acute vascular compromise and warrants immediate surgical evaluation. Adjunctive monitoring technologies, such as implantable Doppler probes, laser Doppler flowmetry, or quantitative fluoroscopy, can provide continuous data but should never replace astute clinical observation.
Anticoagulation protocols vary significantly by institution and surgeon preference, but almost all regimens aim to modulate thrombogenesis without inducing catastrophic surgical site bleeding. A common protocol includes intravenous low-molecular-weight dextran (Dextran 40) to improve microcirculatory rheology, subcutaneous or intravenous heparin, and oral aspirin (81 mg to 325 mg daily) for antiplatelet effect. Intravenous hydration is maintained to ensure slight hemodilution, keeping the hematocrit between 30% and 35%, which optimizes blood viscosity for microvascular flow.
Rehabilitation is initiated as soon as the vascular status is deemed stable, typically between postoperative days 3 and 7, under the direct supervision of a certified hand therapist. The goal of early therapy is to prevent dense tendon adhesions and joint contractures while meticulously protecting the fragile vascular and neural repairs. A modified Kleinert or Duran protocol is often employed, utilizing dynamic splinting to allow early, protected passive flexion and active extension within safe arcs of motion. Active range of motion is generally delayed until 3 to 4 weeks postoperatively, coinciding with the early phases of tendon healing. Strengthening and aggressive scar management protocols are introduced at 8 to 12 weeks. The patient must be counseled that maximal functional recovery, particularly regarding sensory reinnervation and cold intolerance resolution, may take up to 24 to 36 months.
Summary of Landmark Literature and Clinical Guidelines
The evolution of replantation surgery is deeply rooted in landmark clinical studies and foundational guidelines that continue to dictate modern practice. The seminal work by Malt and McKhann (1964) describing the first successful arm replantation, and Komatsu and Tamai (1968) detailing the first microvascular digital replantation, established the technical feasibility of these procedures.
Urbaniak's classification of ring avulsion injuries remains a critical prognostic tool. Urbaniak Class I (circulation adequate) and Class II (circulation inadequate, bone/tendon intact) generally respond well to microvascular reconstruction. However, Class III injuries (complete avulsion with bone/tendon loss) historically carried a dismal prognosis, though modern advancements in venous flow-through flaps and aggressive shortening have improved salvage rates.
Tamai's classification of digital amputations defines the vascular zones of the digit, which directly correlates with surgical success. Zone I amputations (distal to the lunula) require highly specialized super-microsurgical techniques to anastomose vessels smaller than 0.5 mm, often relying on conservative management or composite grafting in adults, though replantation is increasingly successful in specialized centers.
The functional outcomes of replantation are frequently evaluated using Chen's criteria, which assess the recovery of motor function, sensation, joint range of motion, and the ability to return to work. Landmark retrospective reviews have consistently demonstrated that while overall survival rates of replanted digits now exceed 80-90% in experienced centers, functional recovery is highly variable. The literature emphatically supports the use of interpositional vein grafts over primary anastomoses under tension, demonstrating significantly higher patency rates when tension-free repairs are prioritized. Furthermore, clinical guidelines from the American Society for Surgery of the Hand (ASSH) strongly advocate for the centralization of major replantation cases to high-volume, Level I trauma centers equipped with dedicated microsurgical teams, as institutional volume is an independent predictor of both graft survival and long-term functional success.
