Vascularized Bone Grafting: Medial Femoral Condyle and Iliac Crest Flaps
Key Takeaway
Free vascularized bone grafts, including the medial femoral condyle (MFC) and iliac crest flaps, are essential techniques for treating recalcitrant nonunions and achieving complex arthrodesis. This comprehensive guide details the vascular anatomy, indications, and step-by-step surgical harvesting techniques for both the MFC and circumflex iliac systems, providing orthopaedic surgeons with the critical knowledge required for successful microvascular bone reconstruction.
Comprehensive Introduction and Patho-Epidemiology
Progressive valgus deformity of the ankle and hindfoot frequently presents as a devastating and highly complex complication following high-energy trauma, chronic syndesmotic instability, or paralytic conditions. When the lateral column of the ankle fails, the fibula inevitably migrates proximally or laterally under the repetitive axial and shear loads of ambulation. This pathological migration leads to lateral talar shift, profound incongruity of the ankle mortise, and rapid, relentless joint degeneration. The resultant biomechanical environment is fundamentally hostile to standard reconstructive efforts. In cases where standard arthrodesis techniques are rendered insufficient due to poor local biology, massive segmental bone loss, or recalcitrant nonunion, achieving a robust distal tibiofibular fusion becomes paramount to halting deformity progression and salvaging the limb.
The patho-epidemiology of these massive osseous defects and nonunions is deeply intertwined with the vascular compromise of the host bed. High-energy mechanisms, such as open pilon fractures or severe crush injuries, frequently strip the periosteum and obliterate the delicate extraosseous blood supply. Subsequent surgical interventions, infection, and chronic inflammation further deplete the local osteogenic potential, creating a dense, avascular, and fibrotic recipient bed. When traditional non-vascularized autografts (such as standard iliac crest bone graft) are placed into this hostile environment, they undergo creeping substitution—a prolonged process of osteoclastic resorption followed by osteoblastic deposition. In an avascular bed, this process stalls, leading to graft resorption, structural collapse, and ultimately, catastrophic failure of the arthrodesis.
To bridge these critical defects and provide immediate, vitalized osteogenic tissue, orthopaedic reconstructive surgeons and microsurgeons increasingly rely on free vascularized bone grafts. Unlike non-vascularized grafts, vascularized bone transfers bypass the precarious process of creeping substitution. Because the graft's intrinsic blood supply is surgically re-established via microvascular anastomosis, the transferred bone heals to the recipient bed through primary fracture healing mechanisms. The osteocytes within the graft survive the transfer, maintaining immediate structural integrity and profound osteogenic capacity.
The two most versatile, reliable, and extensively studied donor sites for these complex lower and upper extremity reconstructions are the Medial Femoral Condyle (MFC) and the Iliac Crest. The selection between these two donor sites is dictated by the specific mechanical and biological requirements of the recipient bed. The MFC provides a thin, highly pliable, and intensely osteogenic corticoperiosteal layer ideal for recalcitrant nonunions with minimal structural deficits. Conversely, the vascularized iliac crest provides massive, structurally robust bicortical bone capable of bridging significant segmental defects and withstanding the immense mechanical demands of weight-bearing joints. Mastery of both donor sites is an absolute prerequisite for the advanced reconstructive microsurgeon.
Detailed Surgical Anatomy and Biomechanics
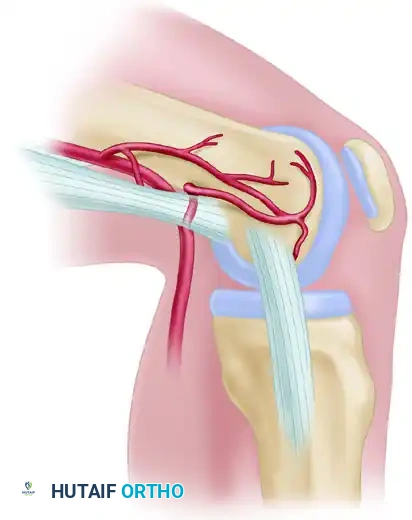
A profound, three-dimensional understanding of the vascular anatomy is non-negotiable for the successful harvest and transfer of vascularized bone flaps. The Medial Femoral Condyle (MFC) flap is uniquely versatile because it can be based off the descending genicular artery (DGA), the superior medial genicular artery (SMGA), or a combination of both, providing redundant and highly reliable perfusion to the corticoperiosteal segment. The descending genicular artery branches off the superficial femoral artery approximately 13 cm above the knee joint line, just proximal to the adductor hiatus. Upon its origin, it consistently divides into two or three distinct branches: the osteoarticular branch, the muscular branch (supplying the vastus medialis), and the saphenous branch (supplying the overlying skin, allowing for a chimeric osteocutaneous flap).
Anatomical cadaveric studies and high-resolution angiographic mapping demonstrate that the descending genicular artery is present in approximately 90% of specimens. The critical osteoarticular branch arises about 11 cm above the knee, lying just deep or lateral to the adductor magnus tendon along the posterior aspect of the medial intermuscular septum. It then arborizes into a rich periosteal plexus over the medial condyle. The superior medial genicular artery is consistently present, arising from the popliteal artery 5 cm above the knee. It courses anteriorly to anastomose with the osteoarticular branch of the descending genicular artery, forming a robust periosteal plexus. In approximately 11% of specimens, the SMGA is the dominant arterial supply to the medial condyle, necessitating a slight alteration in the harvest trajectory.

Biomechanically, the MFC flap provides a thin, pliable layer of corticoperiosteal bone. Unlike the fibula or iliac crest, it is not inherently structural and cannot bridge massive segmental defects (greater than 3-4 cm) under high mechanical load without supplemental rigid internal fixation. However, its immense osteogenic potential makes it the gold standard for treating avascular necrosis (e.g., Preiser disease, Kienböck disease) and recalcitrant nonunions where biological stimulation is prioritized over structural bridging. The periosteal layer of the MFC contains a high concentration of osteoprogenitor cells, which, when coupled with immediate vascularization, rapidly jump-starts the healing cascade in previously inert nonunion sites.
In contrast, the vascularized iliac crest bone flap is the donor site of choice when a reconstruction requires both robust biological activity and significant structural integrity. The iliac crest can be harvested based on either the Superficial Circumflex Iliac Artery (SCIA) or the Deep Circumflex Iliac Artery (DCIA). The DCIA provides a much more robust endosteal and periosteal blood supply, allowing for the harvest of large, structural bicortical grafts. The DCIA arises from the lateral aspect of the external iliac artery, just superior to the inguinal ligament, and courses laterally in a fibrous tunnel formed by the transversus abdominis and iliacus fasciae. This robust pedicle supports the harvest of up to 10-12 cm of curved bicortical bone. The natural curvature of the ilium dictates its biomechanical applications; while excellent for reconstructing the angle of the mandible or the structural arch of the pelvis, employing it for linear long bone defects may require closing wedge osteotomies, provided the periosteal blood supply on the concave side is meticulously preserved.
Exhaustive Indications and Contraindications
The decision to utilize a free vascularized bone graft, and the subsequent selection between the Medial Femoral Condyle and the Iliac Crest, requires a highly nuanced assessment of the recipient site's mechanical and biological deficits. The primary indication for an MFC flap is a recalcitrant nonunion characterized by poor local vascularity but minimal structural bone loss. In the upper extremity, this includes scaphoid nonunions with avascular necrosis of the proximal pole, Kienböck's disease, and clavicular nonunions. In the lower extremity, the MFC is highly effective for localized arthrodesis, including complex distal tibiofibular fusions where local vascularity is compromised by previous surgeries or trauma, yet the gap to be bridged is relatively small (less than 3 cm).
Conversely, the vascularized Iliac Crest flap based on the DCIA is indicated for massive segmental bone defects where immediate structural stability is required alongside biological enhancement. This includes the reconstruction of massive distal tibiofibular defects following tumor resection, severe osteomyelitis debridement, or high-energy ballistic trauma. The iliac crest is also the premier choice for complex maxillofacial reconstructions and the management of large segmental defects of the femur or tibia (up to 10-12 cm) where the fibula may not provide sufficient cross-sectional diameter to withstand immediate axial loading. The SCIA-based iliac crest flap is specifically indicated when a large, reliable overlying skin paddle is the primary requirement, and the structural demands on the bone graft are secondary.
Contraindications to free vascularized bone grafting are absolute and relative, primarily revolving around the patient's physiological capacity to withstand prolonged microsurgical procedures and the patency of the vascular tree. Absolute contraindications include severe peripheral vascular disease that compromises either the donor pedicle or the recipient vessels, active systemic sepsis, and the inability of the patient to tolerate a 6- to 12-hour surgical intervention. Relative contraindications include heavy tobacco use, severe uncontrolled diabetes mellitus, and previous radiation therapy to the donor or recipient sites. Tobacco use, in particular, dramatically increases the risk of microvascular thrombosis and flap failure; thus, strict smoking cessation is mandated for at least 6 weeks preoperatively and postoperatively.
| Feature / Variable | Medial Femoral Condyle (MFC) Flap | Vascularized Iliac Crest (DCIA) Flap |
|---|---|---|
| Primary Indication | Recalcitrant nonunions, AVN, small gaps (<3 cm) | Massive segmental defects (up to 10-12 cm), structural loss |
| Biological Profile | Highly osteogenic, corticoperiosteal | Robust endosteal/periosteal, bicortical |
| Structural Capacity | Low (requires rigid supplemental fixation) | High (capable of immediate load sharing) |
| Vascular Pedicle | Descending Genicular Artery (DGA) / SMGA | Deep Circumflex Iliac Artery (DCIA) |
| Chimeric Potential | Yes (Saphenous branch for skin paddle) | Yes (Internal oblique muscle, overlying skin) |
| Absolute Contraindications | Prior severe knee trauma, compromised SFA | Previous abdominal wall hernia, compromised external iliac |
| Donor Site Morbidity | Low (transient saphenous neuralgia, rare fracture) | Moderate to High (hernia risk, significant pain, gait alteration) |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for free vascularized bone grafting is an exhaustive process that begins with high-resolution imaging of both the donor and recipient sites. For the recipient site, orthogonal radiographs and fine-cut computed tomography (CT) scans are mandatory to accurately define the geometry of the bony defect, assess the quality of the remaining host bone, and template the required dimensions of the bone graft. In cases of chronic osteomyelitis or infected nonunion, magnetic resonance imaging (MRI) may be utilized to delineate the extent of the fibrotic and infected tissue that must be radically debrided prior to reconstruction.
Vascular mapping is the cornerstone of preoperative preparation. The surgeon must absolutely perform preoperative vascular imaging—either CT angiography (CTA) or MR angiography (MRA)—prior to harvesting an MFC or Iliac Crest flap. For the MFC, while the DGA is present in 90% of patients, identifying a dominant SMGA preoperatively will fundamentally alter the surgical approach and dissection trajectory, preventing inadvertent devascularization of the graft. For the recipient site, angiography confirms the patency, caliber, and flow characteristics of the target vessels (e.g., the anterior or posterior tibial vessels for a distal tibiofibular fusion). In traumatized limbs, the "zone of injury" often extends far beyond the visible soft tissue defect, necessitating the planned use of vein grafts or the selection of recipient vessels well proximal to the zone of trauma.
Patient positioning and operating room logistics are critical to minimizing operative time and ischemia. Microvascular reconstruction is highly demanding and should ideally utilize a two-team approach. One surgical team works simultaneously to prepare the recipient site—radically debriding the distal tibiofibular nonunion, isolating the recipient artery and concomitant veins, and preparing the fixation construct. The second team concurrently harvests the flap. For an MFC harvest, the patient is positioned supine with a bump under the ipsilateral hip, allowing the leg to rest in a "frog-leg" position (flexed, abducted, and externally rotated). A sterile tourniquet is applied high on the thigh.
For the Iliac Crest harvest, the patient is placed supine with a significant bump under the ipsilateral hip to elevate the iliac crest and open the space between the costal margin and the anterior superior iliac spine (ASIS). The entire abdomen, groin, and lower extremity are prepped and draped into the sterile field. The anesthesia team must be meticulously briefed; a general anesthetic is administered with strict physiological parameters maintained. The core body temperature must be kept normothermic to prevent peripheral vasospasm, and the use of peripheral vasoconstrictors (e.g., phenylephrine, norepinephrine) is strictly avoided unless absolutely necessary for life-threatening hypotension, as these agents can precipitate catastrophic microvascular thrombosis.
Step-by-Step Surgical Approach and Fixation Technique
Medial Femoral Condyle Harvest
The surgical approach to the MFC begins with a longitudinal incision centered over the medial aspect of the distal femur, extending from the adductor tubercle proximally along the course of the vastus medialis. The deep fascia is incised, and the vastus medialis is carefully elevated and retracted anteriorly. This exposes the medial intermuscular septum and the adductor magnus tendon. The descending genicular artery (DGA) and its concomitant veins are identified as they emerge from the superficial femoral vessels at the adductor hiatus. The pedicle is meticulously traced distally, identifying the muscular, saphenous, and critical osteoarticular branches.
Once the osteoarticular branch is visualized arborizing over the medial condyle, the dimensions of the required corticoperiosteal graft are marked on the bone using a sterile ruler and electrocautery. Using a sharp osteotome or a fine oscillating saw under continuous cold saline irrigation to prevent thermal necrosis, the corticoperiosteal graft is harvested. The depth of the cut is typically 5 to 8 mm, ensuring the subchondral bone and articular cartilage are strictly preserved to prevent joint collapse. The pedicle is left attached and perfused until the recipient site is entirely ready. Once the recipient vessels are prepared, the DGA pedicle is ligated proximally, and the flap is transferred.
Iliac Crest Harvest (DCIA System)
The DCIA system harvest is a complex abdominal wall dissection. The incision parallels the inguinal ligament, starting lateral to the femoral artery and extending superiorly and laterally toward the ASIS and along the iliac crest. The superficial circumflex iliac vessels are identified and protected or ligated depending on the flap design. The external oblique, internal oblique, and transversus abdominis muscles are incised transversely. It is absolutely critical to leave a 2-3 cm cuff of these muscles attached to the inner lip of the iliac crest; this muscle cuff protects the delicate ascending branches of the DCIA that perfuse the bone.
Following muscle transection, blunt preperitoneal dissection is utilized to expose the preperitoneal fascia. The peritoneum is gently retracted medially to expose the posterior aspect of the inner table of the iliac crest and the iliacus muscle. The deep circumflex iliac artery and vein are identified at their origin from the external iliac vessels and traced laterally. The osteotomy is then performed beginning on the lateral surface of the iliac crest using an oscillating saw. During this preperitoneal dissection and isolation of the DCIA pedicle, extreme caution must be exercised to avoid injury to the spermatic cord (or round ligament in females), the external iliac vascular structures, and the genitofemoral branch of the femoral nerve. Retraction should be gentle, and bipolar electrocautery should be used sparingly near the pedicle.
Recipient Site Preparation and Fixation
At the recipient site (e.g., the distal tibiofibular joint), all non-viable, sclerotic bone is aggressively resected until punctate bleeding (the "paprika sign") is observed. The recipient vessels are dissected free of surrounding scar tissue, and adventitial stripping is performed under the operating microscope. The vascularized bone graft is inset into the defect. Because the MFC is non-structural, it is typically packed into the nonunion site and secured with low-profile mini-fragment screws or Kirschner wires, while the primary mechanical stability is provided by a robust bridging plate or an external fixator. The Iliac Crest graft, being structural, is often slotted into a mortise created in the host bone and rigidly fixed with absolute stability using lag screws and strong neutralization plates. Once skeletal fixation is achieved, the microvascular anastomoses (arterial and venous) are performed using 8-0 or 9-0 nylon sutures under high magnification. Ischemia time is meticulously recorded and minimized to prevent no-reflow phenomenon.
Complications, Incidence Rates, and Salvage Management
The execution of free vascularized bone grafting is fraught with potential intraoperative and postoperative complications. The most devastating complication is microvascular thrombosis, which typically occurs within the first 72 hours postoperatively. Arterial thrombosis presents with a pale, cool flap (if a skin paddle is present) and loss of Doppler signal, whereas venous congestion presents with a swollen, violaceous flap with brisk, dark capillary refill. The incidence of pedicle thrombosis ranges from 3% to 8% in high-volume microsurgical centers. Immediate recognition and emergent return to the operating room for pedicle exploration, thrombectomy, and revision anastomosis are mandatory. If the flap cannot be salvaged, it must be explanted to prevent severe systemic toxicity and deep infection.
Donor site morbidity is another significant concern and varies drastically between the MFC and Iliac Crest. Following an MFC harvest, complications are generally mild. Patients may experience transient saphenous nerve neuropraxia (incidence ~15-20%) if the sensory branches were manipulated during harvest. Postoperative hematoma is mitigated by the use of closed suction drains. Rarely (less than 1%), aggressive harvest of the medial condyle can lead to a stress fracture of the distal femur, necessitating prophylactic protected weight-bearing.
Conversely, the Iliac Crest donor site carries a much higher morbidity profile. The most feared complication is the development of a postoperative abdominal hernia, which occurs in 2% to 5% of patients. This is directly related to the failure to adequately repair the transversus abdominis and oblique musculature to the remaining iliac crest or pelvic fascia. Meticulous, multi-layered closure, often utilizing non-absorbable mesh in cases of severe fascial attenuation, is required. Furthermore, patients frequently experience significant, debilitating pain at the iliac crest donor site, which can alter gait mechanics for months postoperatively. Injury to the lateral femoral cutaneous nerve (meralgia paresthetica) is also a known complication during the lateral dissection.
| Complication | Incidence Rate | Clinical Presentation | Salvage / Management Strategy |
|---|---|---|---|
| Microvascular Thrombosis | 3% - 8% | Loss of Doppler signal, pale/blue skin paddle | Emergent OR return, thrombectomy, revision anastomosis. Explant if unsalvageable. |
| Abdominal Hernia (IC Harvest) | 2% - 5% | Bulging at donor site, bowel obstruction risk | Surgical repair with non-absorbable mesh, meticulous fascial closure. |
| Saphenous Neuroma (MFC Harvest) | 10% - 20% | Medial knee pain, paresthesias, Tinel's sign | Gabapentinoids, targeted nerve blocks, surgical excision and burying of stump. |
| Distal Femur Fracture (MFC) | < 1% | Acute knee pain with weight-bearing, radiographic fracture | Open reduction internal fixation (ORIF) with lateral/medial locked plating. |
| Graft Nonunion / Resorption | 5% - 10% | Persistent pain, lack of bridging trabeculae at 6 months | Assess vascularity. Revision rigid fixation, supplementary bone marrow aspirate concentrate (BMAC). |
Phased Post-Operative Rehabilitation Protocols
The success of a free vascularized bone graft depends as much on meticulous postoperative care and phased rehabilitation as it does on flawless intraoperative execution. The postoperative protocol is rigidly structured to protect the delicate microvascular anastomosis while promoting primary bone healing and preventing systemic complications. The immediate postoperative phase (0-72 hours) is the most critical window for microvascular thrombosis. The patient is typically managed in a specialized microsurgical step-down unit. The flap must be monitored every 1 to 2 hours by highly trained nursing staff.
Monitoring modalities include clinical assessment of the skin paddle (color, capillary refill, temperature) and continuous or intermittent Doppler ultrasound. An implantable venous Doppler around the anastomotic site or a surface handheld Doppler should be used to confirm continuous arterial inflow and venous outflow. Any loss of Doppler signal, sudden change in flap turgor, or unexplained drop in hemoglobin mandates immediate evaluation by the operative surgeon. The reconstructed limb (e.g., the ankle following distal tibiofibular fusion) must be strictly immobilized in a well-padded, bivalved splint or a spanning external fixator. Shearing forces across the microvascular anastomosis or the osteotomy sites will lead to catastrophic failure.
During the intermediate phase (1 to 6 weeks), the focus shifts to protecting the osteosynthesis while initiating donor site rehabilitation. Patients are kept strictly non-weight-bearing on the affected extremity for a minimum of 6 to 8 weeks. Dependent positioning of the reconstructed limb is strictly avoided for the first 3 weeks to prevent severe venous congestion and swelling that can compromise the microcirculation. For the iliac crest donor site, early mobilization (within the constraints of the recipient site) helps prevent deep vein thrombosis and pulmonary complications, though patients must be counseled on avoiding maneuvers that increase intra-abdominal pressure.
The late rehabilitation phase (6 weeks to 6 months) is guided by serial radiographic follow-up. Radiographs are obtained at 2, 6, and 12 weeks. Because the graft is vascularized, it will not undergo the typical creeping substitution seen in non-vascularized grafts. Instead, primary bone healing should be observed at the host-graft interfaces, characterized by the bridging of trabecular lines without a preceding radiolucent resorptive phase. Hypertrophy of the graft in response to mechanical loading is a positive prognostic sign, typically visible by 3 to 6 months. Once radiographic union is confirmed, progressive weight-bearing is initiated, advancing from partial to full weight-bearing over a 4-to-6-week period under the guidance of a physical therapist.
Summary of Landmark Literature and Clinical Guidelines
The evolution of free vascularized bone grafting represents a triumph of modern microsurgery, built upon decades of meticulous anatomical research and clinical trial. The use of free vascularized periosteal and corticoperiosteal bone from the medial femoral condyle was first described by Sakai in 1991. Sakai's foundational work demonstrated that the rich periosteal blood supply of the distal femur could be reliably isolated and transferred to treat recalcitrant nonunions. Since its inception, the technique has revolutionized the management of small-to-medium bony defects. Fuchs et al. subsequently described its use extensively in the treatment of nonunions of the clavicle and scaphoid, demonstrating vastly superior union rates compared to traditional non-vascularized autografts, particularly in the setting of avascular necrosis.
The development of the vascularized iliac crest flap was pioneered in the late 1970s and early 1980s by Taylor, Townsend, and Corlett, who first described the reliable anatomy of the deep circumflex iliac artery (DCIA). Their landmark anatomical studies elucidated the profound endosteal and periosteal blood supply provided by the DCIA, establishing it as the premier pedicle for structural bone transfer. Subsequent clinical series by Daniel and Weiland et al. expanded the indications for the DCIA flap, demonstrating its efficacy in reconstructing massive mandibular defects, segmental tibial bone loss, and complex arthrodeses of the lower extremity.
Current clinical guidelines from major orthopaedic and microsurgical societies emphasize that while non-vascularized autografts remain the first line of treatment for small, well-vascularized defects, free vascularized bone grafts are the absolute standard of care for defects exceeding 5-6 cm, defects in irradiated tissue, and recalcitrant nonunions that have failed multiple prior interventions. The utilization of free vascularized bone grafts represents the pinnacle of orthopaedic reconstructive surgery. Whether employing the corticoperiosteal Medial Femoral Condyle flap for recalcitrant nonunions or the structural Deep Circumflex Iliac Artery flap for massive defects and complex distal tibiofibular fusions, a profound understanding of the vascular anatomy is non-negotiable. By adhering to strict microvascular principles, respecting the biomechanical limitations of the donor tissues, and executing meticulous postoperative monitoring, surgeons can achieve successful arthrodesis and limb salvage in the most challenging clinical scenarios.
