Mastering Vascularized Bone Grafts: Iliac Crest, Medial Femoral Condyle, and Composite Rib Transfers
Key Takeaway
Vascularized bone grafting remains a cornerstone in complex orthopaedic reconstruction. This guide details the surgical harvesting and fixation of free iliac crest bone grafts, medial femoral condyle flaps, and composite rib grafts. Key considerations include preserving the nutrient blood supply, navigating complex recipient site fixation, and critical preoperative planning such as identifying the artery of Adamkiewicz during rib harvest to prevent catastrophic spinal cord ischemia.
Comprehensive Introduction and Patho-Epidemiology
The reconstruction of massive skeletal defects—whether secondary to high-energy trauma, radical tumor resection, congenital pseudarthrosis, or recalcitrant nonunion—often exceeds the biological capacity of conventional non-vascularized autografts. In these challenging clinical scenarios, the free vascularized bone graft (VBG) remains the undisputed gold standard in orthopedic microsurgery. By transferring living, biologically active bone with its intrinsic blood supply preserved via microvascular anastomosis, the graft entirely bypasses the protracted, inefficient, and often incomplete process of creeping substitution. This physiological advantage results in accelerated union, profound resistance to deep infection, and the unique ability to undergo primary bone healing even in highly compromised, irradiated, or avascular recipient beds.
The patho-epidemiology of massive bone defects necessitates a nuanced understanding of host biology and mechanical demands. High-energy ballistic injuries or open fractures (Gustilo-Anderson Type IIIB and IIIC) frequently result in composite tissue loss, stripping the periosteum and destroying the local endosteal blood supply. Similarly, the wide en bloc resection of primary bone sarcomas (e.g., osteosarcoma, Ewing sarcoma) or aggressive benign lesions (e.g., giant cell tumors) leaves substantial intercalary or metaphyseal voids. In the absence of a vascularized reconstruction, the placement of massive structural allografts or non-vascularized autografts in these hostile environments carries an unacceptably high rate of infection, fatigue fracture, and nonunion, often culminating in amputation. Vascularized bone grafting directly addresses this patho-epidemiology by importing an independent, robust vascular network that rapidly integrates with the host, delivering osteoprogenitor cells, osteoinductive growth factors, and a durable osteoconductive scaffold simultaneously.
While the free vascularized fibula is universally recognized as the workhorse for long-bone diaphyseal reconstruction due to its linear geometry and length, other donor sites offer unparalleled anatomical, geometric, and biomechanical advantages for specific reconstructive niches. The free iliac crest bone graft provides a massive, naturally contoured corticocancellous volume that is biologically ideal for complex metaphyseal defects, pelvic ring reconstructions, and mandibular restorations. The medial femoral condyle (MFC) corticocancellous flap has revolutionized the treatment of small, recalcitrant nonunions—most notably in the proximal pole of the scaphoid—by delivering highly osteogenic cancellous bone perfectly suited for small, three-dimensional intercalary gaps. Furthermore, composite rib grafts offer unique contouring capabilities and the option for chimeric osteocutaneous or osteochondral transfers, proving invaluable in specialized spinal, facial, and pediatric reconstructions.
Mastering these advanced microvascular donor sites requires an exhaustive understanding of their distinct surgical anatomy, precise harvesting techniques, rigid fixation strategies, and the critical preoperative considerations necessary to mitigate donor site morbidity. As orthopedic microsurgery continues to evolve with the integration of computer-assisted design and manufacturing (CAD/CAM) and 3D stereolithographic templating, the precision and efficacy of transferring the iliac crest, MFC, and rib have reached unprecedented heights. This definitive chapter systematically details the comprehensive management of these specialized vascularized bone grafts, providing the reconstructive surgeon with the requisite knowledge to execute these complex procedures successfully.
Detailed Surgical Anatomy and Biomechanics
The Deep Circumflex Iliac Artery and Iliac Crest
The vascularized iliac crest graft is highly valued for its natural curvature, substantial structural integrity, and dense, rich cancellous bone, which promotes rapid osteointegration at the recipient site. The anatomical basis of this flap is the Deep Circumflex Iliac Artery (DCIA) and its accompanying venae comitantes (DCIV). The DCIA arises from the lateral aspect of the external iliac artery, typically just superior to the inguinal ligament. It courses laterally and superiorly toward the anterior superior iliac spine (ASIS), running within the transversalis fascia. The pedicle length typically ranges from 5 to 7 cm, with an arterial diameter of 1.5 to 3.0 mm, making it highly suitable for microvascular anastomosis.
Crucially, the DCIA provides an ascending branch that supplies the internal oblique muscle, but its primary reconstructive value lies in the nutrient vessels that penetrate the inner table of the ilium. These terminal branches arborize extensively within the iliacus muscle before entering the bone. When harvesting the free iliac crest bone graft, it is an absolute biomechanical and anatomical mandate to retain the covering of the iliacus muscle on the inner table of the iliac crest. Stripping this muscle will sever the nutrient blood supply to the bone, effectively converting a meticulously dissected vascularized graft into a non-vascularized block, inevitably leading to catastrophic graft failure. The biomechanics of the iliac crest allow it to withstand significant compressive loads, making it ideal for bridging metaphyseal defects where a fibula would fail to provide adequate cross-sectional area.
The Descending Genicular Artery and Medial Femoral Condyle
The Medial Femoral Condyle (MFC) flap is a periosteal or corticocancellous flap based primarily on the Descending Genicular Artery (DGA) or, in approximately 11% of cases, the Superomedial Genicular Artery (SMGA). The DGA arises from the superficial femoral artery just proximal to the adductor hiatus in the distal thigh. It divides into three main branches: the saphenous branch, the muscular branch to the vastus medialis, and the critical osteoarticular branch. The osteoarticular branch courses distally and posteriorly over the medial femoral condyle, providing a robust, consistent vascular arborization to the periosteum and the underlying cancellous bone. The pedicle length is typically 7 to 12 cm, with an arterial diameter of 1.5 to 2.5 mm.
The primary biomechanical advantage of the MFC flap is its composition. Unlike the dense cortical bone of the fibula, the MFC provides highly vascularized, structurally sound cancellous bone with a thin cortical shell. This unique architecture allows the graft to be precisely contoured to fit complex, three-dimensional defects, such as the proximal pole of the scaphoid or limited segmental defects of the clavicle and forearm. The rich cancellous network acts as a highly osteogenic sponge, rapidly incorporating into the host bone and driving primary bone healing in avascular environments. Furthermore, because the harvest relies on the non-weight-bearing aspect of the medial condyle, the structural integrity of the distal femur is maintained, provided the harvest dimensions are respected.
Intercostal Vasculature and Composite Rib Grafts
Vascularized rib grafts offer a unique combination of pliable bone and, if necessary, overlying soft tissue, muscle, or cartilage. Two distinct anatomical types of vascularized rib grafts are utilized clinically, differentiated by their vascular supply. The posterior rib graft is harvested with its nutrient vessels intact, providing both medullary and periosteal circulation. It relies on the proximal intercostal artery, which arises directly from the descending thoracic aorta. The posterolateral (segmental) rib graft is supplied solely by periosteal vessels derived from the intercostal muscle cuff harvested in continuity with the rib. Despite these anatomical differences in medullary versus periosteal blood supply, clinical and experimental data demonstrate that the viability and osteogenic potential of these two types of grafts are equivalent, provided the microvascular anastomosis is patent.
The biomechanics of the rib graft are characterized by its inherent flexibility and curvature. The rib is highly malleable, particularly when multiple closing-wedge osteotomies are performed along its inner cortex, allowing it to be shaped to match the contour of the mandible or the structural requirements of a kyphotic spine. However, the rib is mechanically weaker in compression compared to the fibula or iliac crest. Therefore, when used in load-bearing applications, it must be supplemented with rigid internal fixation to prevent fatigue fracture during the integration phase.
Exhaustive Indications and Contraindications
The selection of a specific vascularized bone graft is dictated by the precise anatomical, biomechanical, and biological requirements of the recipient site, weighed against the patient's physiological capacity to tolerate the donor site morbidity. The indications for the iliac crest, MFC, and rib grafts are highly specialized and distinct from those of the vascularized fibula.
The vascularized iliac crest is the premier choice for massive metaphyseal defects where a fibula would result in an unacceptable mismatch in cross-sectional area. It is heavily utilized in hemipelvic reconstructions following internal hemipelvectomy for chondrosarcoma, as well as in composite mandibular reconstructions requiring significant bone height for subsequent osseointegrated dental implants. The MFC flap is the definitive solution for small, recalcitrant nonunions complicated by avascular necrosis (AVN). Its most celebrated application is in the treatment of scaphoid nonunions with proximal pole AVN, where it has demonstrated union rates exceeding 90% in cases that have failed multiple prior non-vascularized grafting attempts. The vascularized rib is selectively indicated for multi-level anterior spinal fusions in heavily irradiated beds, complex facial reconstructions requiring osteochondral composite tissue (utilizing the costochondral junction), and pediatric mandibular reconstructions.
Contraindications to microvascular bone grafting encompass severe systemic illness, uncorrectable coagulopathies, and profound peripheral vascular disease that precludes a safe microvascular anastomosis. Active smoking is a profound relative, and often absolute, contraindication due to the severe vasoconstrictive effects of nicotine, which exponentially increase the risk of pedicle thrombosis. Specific donor site contraindications include prior surgery or trauma that has compromised the vascular pedicle, such as a previous inguinal hernia repair with mesh compromising the DCIA, or prior knee trauma altering the DGA anatomy.
Graft-Specific Clinical Algorithms
| Feature / Parameter | Free Iliac Crest Graft | Medial Femoral Condyle (MFC) | Composite Rib Graft |
|---|---|---|---|
| Primary Indications | Pelvic ring reconstruction, Mandibular body/ramus, Metaphyseal long-bone defects | Scaphoid nonunion with AVN, Clavicle nonunion, Small intercalary upper extremity defects | Irradiated spinal fusion, Osteochondral facial reconstruction, Pediatric mandible |
| Bone Composition | Massive Corticocancellous | Predominantly Cancellous with thin cortex | Cortical shell with medullary canal, highly pliable |
| Vascular Pedicle | Deep Circumflex Iliac Artery (DCIA) | Descending Genicular Artery (DGA) | Intercostal Artery |
| Pedicle Length | 5 – 7 cm | 7 – 12 cm | 4 – 6 cm |
| Absolute Contraindications | Prior DCIA disruption, Severe abdominal wall laxity | Prior distal medial thigh trauma, Pre-existing severe knee osteoarthritis | Prior ipsilateral thoracotomy, Pedicle origin of Artery of Adamkiewicz |
| Major Donor Morbidity | Incisional Hernia, Lateral femoral cutaneous nerve palsy | Knee stiffness, Iatrogenic medial condyle fracture | Pneumothorax, Anterior spinal artery syndrome (Paraplegia) |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Angiographic Mapping
The success of a free vascularized bone transfer hinges entirely on meticulous preoperative planning and the precise mapping of both donor and recipient vasculature. Standard orthogonal radiographs and high-resolution computed tomography (CT) scans are mandatory to accurately define the three-dimensional geometry of the osseous defect. In contemporary orthopedic oncology and complex trauma reconstruction, these CT data sets are routinely imported into CAD/CAM software to generate stereolithographic 3D models. These models allow the surgical team to pre-contour fixation plates, determine the exact osteotomy angles required at the donor site, and minimize the ischemic time during the actual transfer.
Vascular imaging is equally critical. CT angiography (CTA) or Magnetic Resonance Angiography (MRA) of the donor and recipient sites must be performed to confirm the presence, caliber, and anatomical variations of the pedicles. For the MFC flap, CTA confirms the dominance of the DGA versus the SMGA. For the iliac crest, the origin and course of the DCIA are mapped to rule out atherosclerotic occlusion.
When planning a vascularized rib graft, the neurological stakes are unprecedentedly high. The blood supply to the lower thoracic and upper lumbar spinal cord is highly dependent on a dominant radicular artery. Selective spinal arteriography is absolutely mandatory prior to rib harvest to assess the location of the arteria radiculomedullaris magna (Artery of Adamkiewicz). This critical vessel usually arises from the dorsal branch of the lower intercostal or upper lumbar arteries, predominantly on the left side (in approximately 75% of patients) between T8 and L1. It is paramount to establish the exact anatomical location of this artery to ensure it does not originate from the chosen intercostal artery. Ligation of the intercostal artery that gives rise to the artery of Adamkiewicz will result in profound anterior spinal artery syndrome, leading to irreversible paraplegia.
Surgical Positioning and Two-Team Setup
Vascularized bone grafting is a highly orchestrated procedure that demands a synchronized, two-team approach to minimize operative time and graft ischemia. The recipient team is responsible for radical debridement, recipient vessel preparation, and initial hardware placement, while the donor team simultaneously harvests the flap.
Patient positioning must accommodate simultaneous access to both surgical fields. For an iliac crest harvest, the patient is placed supine with a sandbag or gel bump under the ipsilateral hip to elevate the hemi-pelvis. The entire hemi-pelvis, lower abdomen, and ipsilateral lower extremity are prepped and draped to allow for intraoperative manipulation. For the MFC flap, the patient is positioned supine with a bump under the ipsilateral hip, allowing the knee to rest in a slightly flexed, "frog-leg" position to expose the medial thigh. A sterile tourniquet is applied high on the thigh. For the rib graft, the patient is typically placed in the lateral decubitus position, which may preclude a simultaneous two-team approach depending on the location of the recipient site, thereby necessitating a sequential surgical strategy.
Step-by-Step Surgical Approach and Fixation Technique
Iliac Crest Harvest and Pelvic Closure
The harvest of the vascularized iliac crest begins with an incision made parallel to and approximately 2 cm superior to the inguinal ligament, extending from the femoral pulse laterally toward the ASIS, and continuing posteriorly along the iliac crest. The external oblique aponeurosis is carefully incised, and the internal oblique and transversus abdominis muscles are divided to expose the transversalis fascia. The DCIA and DCIV are identified near their origin at the external iliac vessels and traced laterally. The dissection must be meticulous to avoid injury to the lateral femoral cutaneous nerve, which frequently crosses the pedicle near the ASIS.
As the dissection proceeds toward the ilium, a 2 to 3 cm cuff of the internal oblique, transversus abdominis, and iliacus muscles must be maintained attached to the inner table of the crest. This muscle cuff protects the ascending branch and the delicate nutrient vessels penetrating the bone. Using an oscillating saw and sharp osteotomes, the required length and depth of the iliac crest are harvested. The cuts are made strictly from the outer table inward, ensuring the inner table and its muscular pedicle remain completely undisturbed. Once the bone is fully mobilized and the recipient site is prepared, the DCIA and DCIV are ligated at their origin, and the composite graft is transferred. Closure of the donor site is notoriously challenging due to the resection of the abdominal wall musculature insertions. The donor site must be closed in multiple robust layers, often utilizing heavy non-absorbable sutures or mesh reinforcement. To facilitate primary closure and reduce tension, the hip is flexed, and the patient is maintained in a "beach chair" position postoperatively.
Medial Femoral Condyle Elevation
The surgical approach to the MFC begins with a longitudinal incision over the medial aspect of the distal thigh, centered over the vastus medialis. The fascia is incised, and the vastus medialis is elevated anteriorly, exposing the medial intermuscular septum. The DGA is identified as it emerges from the superficial femoral artery and courses over the medial femoral condyle. The pedicle is carefully dissected distally, preserving the osteoarticular branches while ligating the muscular and saphenous branches to maximize pedicle length and mobility.
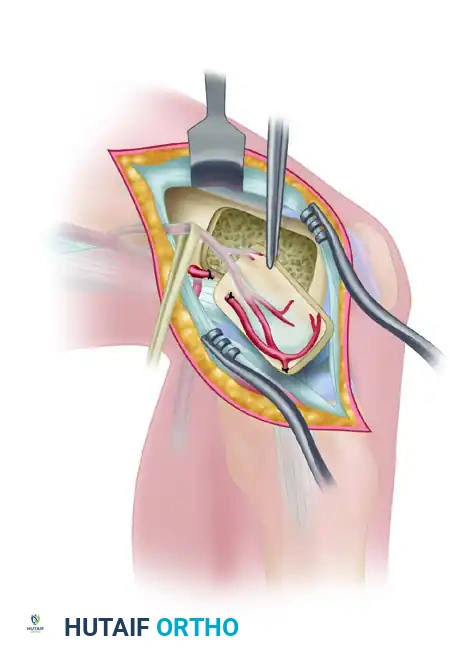
Once the pedicle is isolated, a corticocancellous block is outlined on the medial condyle with a surgical marker, typically measuring up to 3 cm by 2 cm, depending on the defect size. Using a thin oscillating saw and sharp, curved osteotomes, the bone block is harvested. It is imperative that the periosteal blood supply remains meticulously attached to the underlying cortex during the osteotomy. The graft is then gently elevated, ensuring the deep cancellous bone remains intact and the pedicle is not subjected to traction or torsion.
FIGURE 63-47: Flap elevated from the medial femoral condyle, demonstrating the vascular pedicle and the harvested corticocancellous block prior to microvascular transfer.
Rib Resection and Pleural Management
Because of the anatomical variability and the catastrophic risks associated with the lower thoracic vessels, donor site selection for the rib graft must be meticulous. The ninth rib (left or right) is universally recommended as the primary donor site, as it provides adequate length, a reliable intercostal pedicle, and generally avoids the most common origins of the artery of Adamkiewicz. The patient is placed in the lateral decubitus position. An incision is made directly over the chosen rib. The latissimus dorsi and serratus anterior muscles are divided to expose the rib cage.
The periosteum of the superior rib and the inferior rib is preserved, but the intercostal muscles attached to the harvested rib are kept intact to preserve the vascular pedicle. The rib is osteotomized anteriorly at the costochondral junction (unless a composite cartilage graft is required) and posteriorly near the angle of the rib. The intercostal artery and vein are then dissected proximally toward the aorta and azygous system to obtain adequate pedicle length. Extreme care must be taken to avoid breaching the underlying parietal pleura. If a pleural tear occurs, it must be meticulously repaired with absorbable sutures under positive pressure ventilation, and a chest tube is routinely placed to prevent tension pneumothorax.
Microvascular Anastomosis and Recipient Fixation
Placing and securing these specialized grafts in the recipient site presents unique biomechanical challenges. Because the iliac graft is relatively short and bulky, fixation techniques that consume bone length—such as insetting or doweling the graft into the medullary canal—may severely compromise the reconstruction. Furthermore, the natural curvature of the ilium and the varying thickness of its cortices make standard plate contouring unpredictable. Fixation is often best achieved using an external fixation device, which spans the defect and neutralizes forces without requiring direct hardware application to the graft. Alternatively, a combination of limited internal fixation with independent lag screws can be utilized at the host-graft junctions, meticulously avoiding compression of the vascular pedicle.
For the MFC graft in scaphoid reconstructions, fixation is typically achieved with headless compression screws or fine Kirschner wires. The microvascular anastomosis is performed under an operating microscope, utilizing 8-0 or 9-0 nylon sutures. The recipient vessels (e.g., the radial artery and cephalic vein for the scaphoid, or the posterior tibial vessels for lower extremity defects) are prepared, and an end-to-end or end-to-side anastomosis is performed. Ischemia time must be minimized, ideally kept under two hours, to prevent irreversible ischemia-reperfusion injury to the osteocytes and microvasculature.
Complications, Incidence Rates, and Salvage Management
Microvascular Failure and Flap Salvage
The most devastating complication following vascularized bone grafting is microvascular thrombosis, which typically occurs within the first 72 hours postoperatively. The incidence of arterial thrombosis or venous congestion ranges from 3% to 7% in high-volume microsurgical centers. Arterial occlusion presents as a sudden loss of Doppler signal, pallor of the chimeric skin paddle (if present), and an absence of capillary refill. Venous congestion, which is more common, presents as a swollen, violaceous skin paddle with a rapid, dark return on capillary refill testing.
Immediate re-exploration is the only viable salvage strategy. The anastomosis must be inspected under the microscope. If a thrombus is identified, a thrombectomy is performed, the vessel edges are resected to healthy intima, and the anastomosis is revised, often requiring an interpositional vein graft (e.g., saphenous vein) to bridge the resulting gap without tension. Local administration of thrombolytics (e.g., tissue plasminogen activator or urokinase) and systemic heparinization may be employed to clear the microcirculation. If the flap cannot be salvaged, it must be explanted, and the defect managed with an antibiotic spacer until a secondary reconstructive procedure can be planned.
Donor Site Morbidity
Donor site morbidity represents a significant clinical challenge and must be explicitly discussed with the patient during the informed consent process. The iliac crest donor site carries a 5% to 9% risk of incisional hernia due to the disruption of the abdominal wall aponeurosis. Meticulous, multi-layered closure and strict postoperative hip flexion are critical to mitigating this risk. Additionally, injury to the lateral femoral cutaneous nerve can result in meralgia paresthetica, characterized by numbness and dysesthesia over the anterolateral thigh.
The MFC donor site is generally well-tolerated, but aggressive harvesting that violates the structural integrity of the medial condyle can lead to an iatrogenic distal femur fracture, requiring immediate open reduction and internal fixation. Postoperative knee stiffness and localized hematoma are also reported, necessitating early, protected range-of-motion exercises. Rib graft harvesting carries the inherent risks of thoracic surgery, including pneumothorax (up to 15% incidence), atelectasis, pleural effusion, and severe postoperative pain that can compromise respiratory excursion.
| Complication | Associated Graft | Incidence Rate | Prevention and Salvage Management |
|---|---|---|---|
| Incisional Hernia | Iliac Crest | 5% - 9% | Multi-layer closure, mesh reinforcement, postoperative hip flexion. Salvage: General surgery hernia repair. |
| Microvascular Thrombosis | All (Iliac, MFC, Rib) | 3% - 7% | Meticulous intimal approximation, avoid pedicle tension/kinking. Salvage: Immediate re-exploration, thrombectomy, vein grafting. |
| Pneumothorax | Composite Rib | 10% - 15% | Meticulous subperiosteal dissection, positive pressure valsalva check. Salvage: Primary pleural repair, immediate chest tube insertion. |
| Femoral Condyle Fracture | MFC | < 2% | Limit harvest size, avoid deep cortical notching, prophylactic fixation if weak. Salvage: ORIF with locking plates. |
| Spinal Cord Ischemia | Composite Rib | < 1% | Mandatory preoperative selective spinal angiography to map Artery of Adamkiewicz. Salvage: Irreversible; strictly preventative. |
Phased Post-Operative Rehabilitation Protocols
Acute Post-Operative Phase (Days 0-7)
The postoperative management of patients undergoing free vascularized bone grafting requires a highly coordinated, multidisciplinary approach focused on flap survival, hemodynamic optimization, and the initiation of optimal bone healing. During the acute phase, the patient is monitored in an intensive care or specialized microsurgical step-down unit. Hemodynamic stability is paramount; the surgical team must maintain adequate systemic blood pressure and hydration to ensure optimal perfusion pressure across the delicate microvascular anastomosis. The use of systemic vasopressors is generally avoided or used with extreme caution, as they can induce profound vasospasm in the newly anastomosed pedicle, precipitating thrombosis.
Flap monitoring is conducted aggressively, typically every hour for the first 48 hours, and then gradually spaced out. If a chimeric flap was harvested (e.g., an iliac crest graft with an overlying cutaneous paddle), the skin paddle serves as a highly reliable, continuous clinical monitor for the buried bone graft. In purely osseous grafts, an implantable venous Doppler probe is often utilized for the first 5 to 7 days to continuously monitor anastomotic patency. The recipient site must be rigidly immobilized. Because vascularized grafts bypass creeping substitution, they heal via primary bone healing, but the graft is initially mechanically weak and highly susceptible to shear forces at the osteotomy junctions.
Subacute and Long-Term Integration
Donor site care during the subacute phase is tailored to the specific graft harvested. For iliac crest harvests, hip flexion is maintained in a "beach chair" position for the first week to protect the abdominal closure. Early mobilization is encouraged to prevent deep vein thrombosis, but core-straining activities and heavy lifting are strictly prohibited for a minimum of 6 to 8 weeks. For rib harvests, aggressive pulmonary toilet, incentive spirometry, and adequate multimodal analgesia (often including regional blocks or epidurals) are critical to prevent atelectasis and hospital-acquired pneumonia.
Weight-bearing protocols are strictly regulated. For lower extremity and pelvic reconstructions utilizing the iliac crest, patients remain strictly non-weight-bearing until definitive radiographic union is confirmed at the host-graft junctions, which typically occurs between 3 and 6 months. This is followed by a protracted period of progressive, protected weight-bearing. This gradual loading is essential to stimulate the graft to hypertrophy in response to mechanical stress, in accordance with
