Bone and Joint Management in Replantation Surgery
Key Takeaway
Effective bone and joint management is the foundation of successful limb and digit replantation. This guide details critical techniques, including precise bone shortening to enable tension-free neurovascular anastomoses, and rigid skeletal fixation using Kirschner wires, intraosseous loops, or plates. By mastering these evidence-based protocols, orthopedic surgeons can optimize functional recovery, minimize nonunion rates, and ensure the viability of replanted extremities across varying levels of amputation.
Comprehensive Introduction and Patho-Epidemiology
The management of bones and joints during replantation surgery dictates the functional outcome and survival of the amputated part. Establishing a rigid, stable skeletal framework is the mandatory first step following meticulous débridement. Without absolute skeletal stability, subsequent microvascular anastomoses and neurorrhaphies are subjected to catastrophic shear forces, leading to thrombosis, ischemia, and ultimate replant failure. The overarching goals of skeletal management in replantation include rapid and rigid fixation to protect delicate microvascular repairs, anatomic alignment to restore axial and rotational alignment optimizing tendon excursion and joint kinematics, strategic bone shortening to allow tension-free repair of soft tissues, nerves, and vessels, and the absolute preservation of biology by minimizing periosteal stripping to ensure bone healing.
Traumatic amputations of the upper and lower extremities represent devastating injuries with profound functional, psychological, and socioeconomic consequences. Epidemiologically, these injuries predominantly affect young, working-age males, often resulting from industrial accidents involving power tools, heavy machinery, or agricultural equipment. The mechanism of injury plays a paramount role in determining the viability of the amputated part and the complexity of the skeletal reconstruction. Guillotine-type amputations, characterized by sharp, clean transections, present the most favorable prognosis, as the zone of injury is highly localized, allowing for minimal bone resection and straightforward osteosynthesis. Conversely, crush and avulsion injuries impart extensive, diffuse trauma to the osseous architecture and the surrounding soft-tissue envelope. These mechanisms create a wide zone of injury characterized by severe intimal damage to vessels, extensive periosteal stripping, and comminution of the bony framework.
The pathophysiology of the amputated extremity is governed by the ischemic cascade. Skeletal muscle can tolerate warm ischemia for approximately six hours before irreversible myonecrosis occurs, whereas digits, lacking muscle bellies, can tolerate up to twelve hours of warm ischemia and up to twenty-four hours of cold ischemia. The imperative for rapid skeletal stabilization cannot be overstated; prolonged ischemia time directly correlates with the "no-reflow" phenomenon, where microvascular thrombosis persists despite technically flawless anastomoses. Therefore, the orthopedic surgeon must execute skeletal fixation with extreme efficiency, balancing the biomechanical need for absolute stability with the biological clock of tissue viability.
Furthermore, the initial management of the skeletal framework sets the stage for the entire reconstructive effort. The skeletal construct must be sufficiently robust to withstand the immediate postoperative mobilization protocols necessary to prevent tendon adhesions and joint contractures. A failure at the bone-hardware interface not only jeopardizes the vascular repairs but also condemns the patient to a stiff, non-functional appendage, which is often functionally inferior to a well-constructed amputation stump. Consequently, the orthopedic surgeon's approach to bone and joint management in replantation must be meticulous, pre-planned, and executed with an uncompromising adherence to biomechanical and biological principles.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the upper extremity skeleton is an absolute prerequisite for successful replantation. The phalanges and metacarpals possess a unique diaphyseal geometry, characterized by a palmar concavity and a dorsal convexity. This anatomical bow is critical for the mechanical advantage of the flexor and extensor mechanisms. When performing bone shortening and subsequent osteosynthesis, the surgeon must meticulously recreate this palmar bow; failure to do so results in a loss of the mechanical advantage of the flexor tendons, leading to a profound decrease in grip strength and an increased risk of tendon bowstringing.
The vascular anatomy of the tubular bones of the hand dictates the biological approach to fixation. The diaphysis is supplied by a dual system: the nutrient artery system (endosteal) and the periosteal plexus. In the context of a traumatic amputation, the endosteal blood supply is invariably severed. Consequently, the survival and subsequent union of the replanted bone segment rely entirely on the precarious periosteal blood supply and the ingrowth of neovasculature from the surrounding soft-tissue envelope. The surgical warning remains absolute: the periosteum must be stripped minimally. Excessive periosteal elevation devascularizes the bone ends, significantly increasing the risk of nonunion, infection, and hardware failure.
Bone shortening is a cornerstone principle in replantation surgery, serving multiple critical biomechanical and biological functions. Primarily, it permits tension-free vascular anastomoses and nerve repairs, which is the single most important factor in preventing microvascular thrombosis. Tension across a microvascular repair induces intimal hyperplasia, vasospasm, and turbulent flow, invariably leading to failure. Secondly, initial bone shortening reduces the size of the soft tissue defect, allowing for primary closure without the immediate need for complex, time-consuming local or free flaps. Finally, it allows for aggressive, maximal soft tissue débridement, effectively converting a jagged, contaminated crush injury into a clean, "guillotine-type" injury.
If interpositional vein grafts are utilized, the absolute need for bone shortening is minimized. However, relying on vein grafts introduces the risk of two anastomotic sites per vessel rather than one, inherently decreasing the overall patency rate. Furthermore, harvesting the vein and performing additional anastomoses significantly prolongs ischemia time. Vein grafting is generally reserved for scenarios where amputation has occurred near an undamaged joint, and shortening would destroy the articular surface.
The Thumb Exception
While shortening is highly beneficial in the fingers, shortening of an amputated thumb must be kept to an absolute minimum. The thumb contributes to approximately 40% to 50% of overall hand function, and its length is critical for effective opposition and pinch kinematics. The biomechanics of the thumb carpometacarpal (CMC) joint allow for a wide arc of motion, but this functional envelope is highly dependent on the lever arm provided by the metacarpal and phalanges. Excessive shortening compromises the ability of the thumb pulp to meet the index and long fingers, severely disabling fine motor tasks and power pinch.
When shortening the thumb proximal phalanx, the surgeon should use an oscillating saw under continuous saline irrigation to remove bone in meticulous 2- to 3-mm increments until satisfactory, tension-free shortening is achieved. In the lesser digits, shortening of 1 cm usually allows for tension-free vessel anastomosis without excessively impairing hand function. However, shortening a digit much more than 1 to 1.5 cm frequently impairs the biomechanical advantage of the intrinsic muscles, altering the length-tension curve of the lumbricals and interossei, and severely limits the functional arc of motion.
Exhaustive Indications and Contraindications
The decision to proceed with replantation versus revision amputation requires a complex calculus involving patient factors, injury characteristics, and institutional capabilities. Skeletal management is a major variable in this equation. Replantation is generally indicated for amputations of the thumb at any level, multiple digits, amputations in pediatric patients, and amputations at or proximal to the wrist joint (macro-replantations). In these scenarios, the functional deficit incurred by amputation is so severe that the exhaustive resources and prolonged rehabilitation associated with replantation are overwhelmingly justified. For single-digit amputations distal to the flexor digitorum superficialis (FDS) insertion (Zone I), replantation is often indicated for aesthetic and functional restoration of the fingertip, utilizing specialized skeletal fixation techniques such as longitudinal pinning.
Contraindications to replantation are heavily influenced by the condition of the skeletal and soft-tissue elements. Absolute contraindications include severe crush or avulsion injuries with multi-level segmental skeletal destruction, where the zone of injury precludes the establishment of a stable, shortened skeletal framework without resulting in a functionally useless appendage. Prolonged warm ischemia time (greater than 6 hours for proximal amputations containing muscle mass) is a strict contraindication due to the risk of reperfusion injury, myoglobinuria, and systemic toxicity (crush syndrome). Life-threatening concomitant injuries take absolute precedence; the patient's physiological stability must never be compromised for limb salvage.
Relative contraindications require nuanced surgical judgment. Single-digit amputations in Zone II (proximal to the FDS insertion) in adults remain controversial; the resulting stiffness from combined skeletal, tendon, and nerve injury often yields a digit that impedes overall hand function. Extreme contamination, severe psychiatric illness, and profound medical comorbidities (e.g., severe peripheral vascular disease, uncontrolled diabetes mellitus) significantly elevate the risk of failure and must be carefully weighed. Furthermore, if the skeletal reconstruction requires such extensive shortening that the resulting digit will lack the intrinsic biomechanical advantage to function, revision amputation may be the superior choice.
| Parameter | Indications for Replantation | Contraindications (Absolute & Relative) |
|---|---|---|
| Patient Demographics | Pediatric patients (almost all levels), highly motivated adults | Severe psychiatric illness, non-compliant patients, severe medical comorbidities |
| Anatomical Level | Thumb (any level), multiple digits, wrist, forearm, arm | Single digit Zone II (relative), distal fingertip with severe crush |
| Mechanism of Injury | Guillotine, sharp lacerations, minimal crush | Severe avulsion, multi-level segmental bone loss, extreme contamination |
| Ischemia Time | Cold ischemia < 24h (digits), < 12h (proximal) | Warm ischemia > 6h (proximal with muscle), > 12h (digits) |
| Skeletal Status | Reconstructable bone stock, viable joints | Irreparable comminution, inability to achieve stable fixation |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning begins the moment the patient and the amputated part arrive at the trauma center. The amputated part must be immediately retrieved, wrapped in saline-moistened gauze, placed in a sealed plastic bag, and submerged in an ice-water slurry to establish optimal cold ischemia (approximately 4°C). Direct contact between the tissue and ice must be strictly avoided to prevent frostbite and irreversible cellular damage. Radiographic evaluation of both the amputation stump and the amputated part is mandatory. High-quality orthogonal radiographs allow the surgeon to assess the level of bone injury, the degree of comminution, and the presence of foreign bodies, and to formulate a definitive plan for osteosynthesis.
Templating is a critical step in determining the required extent of bone shortening. The surgeon must measure the anticipated defect and calculate the necessary resection to achieve healthy, bleeding bone margins while ensuring a tension-free soft-tissue envelope. In the digits, this typically involves planning for 1 to 1.5 cm of shortening. For macro-replantations of the forearm or arm, shortening of 2 to 5 cm may be required. The surgical team should prepare a sterile field for the amputated part separate from the patient, allowing a two-team approach. The "bench team" performs meticulous débridement of the amputated part, isolates and tags vessels and nerves under loupe or microscopic magnification, and prepares the distal bone ends for fixation.
Patient positioning is tailored to the level of amputation. For upper extremity replantations, the patient is positioned supine with the affected arm extended on a radiolucent hand table. A pneumatic tourniquet is applied to the proximal arm. Regional anesthesia (brachial plexus block) is highly preferred over general anesthesia whenever feasible. Regional anesthesia not only avoids the systemic risks of prolonged general anesthesia but also provides a profound sympathectomy, maximizing peripheral vasodilation and optimizing microvascular flow post-anastomosis. A Foley catheter is placed, and the patient is prepped and draped to allow access to the iliac crest or distal radius in the event that structural bone grafting is unexpectedly required.
The sequence of replantation must be established pre-operatively. The standard sequence typically follows: 1) Identification and tagging of structures, 2) Skeletal fixation, 3) Extensor tendon repair, 4) Venous anastomoses, 5) Arterial anastomoses, 6) Neurorrhaphy, and 7) Flexor tendon repair. However, in cases of prolonged ischemia, the sequence may be altered to perform arterial shunting or immediate arterial anastomosis prior to definitive skeletal fixation, though this places the vascular repairs at high risk during subsequent bone manipulation.
Step-by-Step Surgical Approach and Fixation Technique
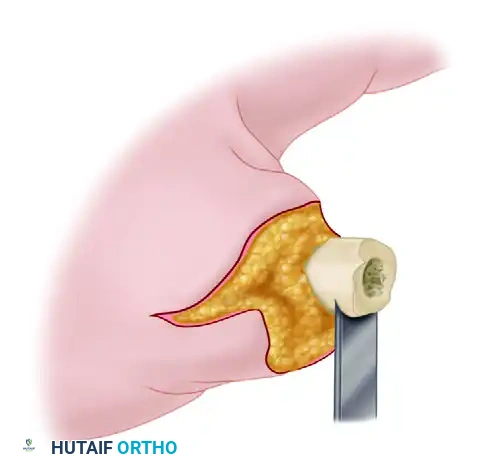
The surgical approach to skeletal fixation in replantation demands a synthesis of speed, rigidity, and biological respect. Once the bone ends are exposed, the periosteum is carefully elevated only 1 to 2 millimeters from the fracture edge. Using an oscillating saw under continuous, copious saline irrigation to prevent thermal necrosis, the bone ends are resected to healthy, bleeding cortex. The cuts must be perfectly perpendicular to the longitudinal axis of the bone in both the coronal and sagittal planes to prevent angular deformity, unless a specific compensatory angle is required.
Bone fixation in digits and metacarpals must balance the need for rigidity with the constraints of time and soft-tissue envelope volume. While mini-plates and screws offer rigid internal fixation and allow for immediate active mobilization, they are often too time-consuming to apply and too bulky for distal replantations, frequently causing skin necrosis over the dorsal aspect of the digits. Therefore, Kirschner wires (K-wires) and intraosseous wiring remain the undisputed workhorses of digital replantation.
Kirschner Wire Fixation
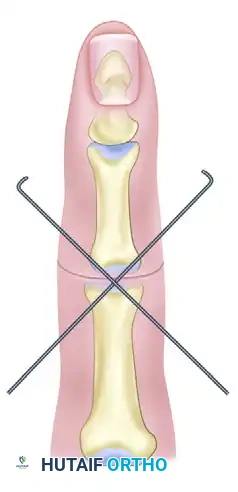
Fixation is most commonly achieved using either two parallel medullary axial K-wires or a single axial K-wire supplemented by an oblique K-wire. The oblique wire is absolutely critical to control rotational forces, which a single axial wire cannot resist. Rotational malalignment is disastrous in the hand, leading to overlapping digits during flexion and profound functional impairment.
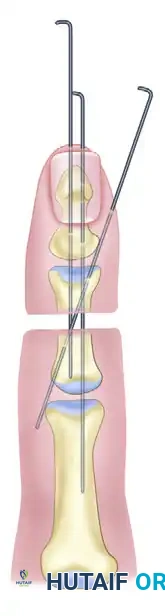
Parallel K-wires provide excellent bending stability but require sufficient bone width, making them more suitable for metacarpals and proximal phalanges. The axial plus oblique K-wire technique is ideal for narrower phalanges. The axial wire is driven retrogradely through the distal segment, the fracture is reduced, and the wire is advanced antegrade into the proximal segment. The oblique wire is then driven across the fracture site, ensuring it engages the opposite cortex for maximal purchase. Wires should be placed to allow joint motion whenever possible; transarticular pinning should be strictly avoided unless necessary for stability in very proximal or highly comminuted fractures.
Intraosseous Wiring Techniques
When the amputation occurs near an undamaged joint, standard longitudinal K-wires may violate the articular surface, leading to chondrolysis and post-traumatic arthritis. In these instances, wire loops passed through transverse drill holes provide excellent compression and stability without articular compromise.
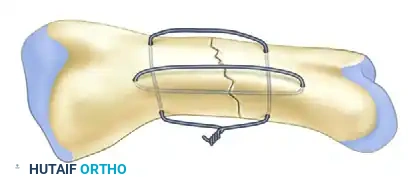
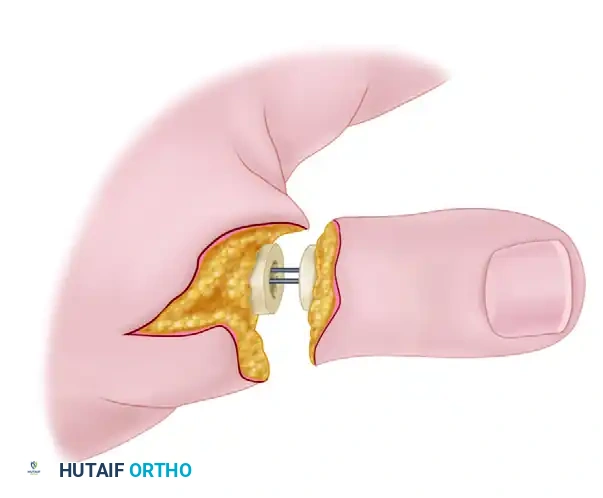
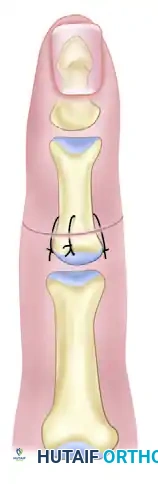
Intraosseous wiring is typically performed utilizing a 90-90 wiring technique or a single palmar loop combined with a dorsal stabilizing K-wire. Using a 0.035-inch K-wire, transverse holes are drilled 3 to 5 millimeters from the resected bone ends. A 24-gauge or 26-gauge stainless steel wire is passed through the holes. The fracture is meticulously reduced, and the wire is tightened, creating dynamic compression across the osteotomy site. This technique offers a remarkably low-profile construct that does not interfere with the delicate gliding of the extensor mechanism.
Periosteal repair should be performed whenever feasible. Suturing the periosteum with 4-0 or 5-0 absorbable suture after bone fixation enhances the biological environment for osteogenesis, contains the fracture hematoma, and provides a smooth gliding surface for the extensor mechanism, significantly reducing post-operative tendon adhesions.
Management of Articular Amputations
Amputations that directly damage the digital joints present a unique reconstructive challenge. The surgeon must decide between primary arthrodesis and joint arthroplasty based on the mechanism of injury, the level of contamination, and the patient's occupational requirements. Amputations involving severe crush or avulsion injuries to the articular surfaces are unequivocally treated by primary arthrodesis. The damaged articular cartilage is resected to healthy, bleeding subchondral bone using a cup-and-cone reamer or flat saw cuts.
Positioning for arthrodesis is critical for hand function. The distal interphalangeal (DIP) joint is typically fused at 10° to 15° of flexion, the proximal interphalangeal (PIP) joint at 30° to 40° of flexion (increasing from index to small finger), and the metacarpophalangeal (MCP) joint at 25° to 35° of flexion. Fixation is achieved with crossed K-wires or tension-band wiring.
In highly selected cases, joint motion can be preserved by the primary insertion of a silicone (Silastic) implant. This method is strictly reserved as a primary procedure for amputations that are sharp and clean (guillotine-type), devoid of significant crush or contamination, and occurring in patients whose occupational requirements demand mobile joints.
Placing a Silastic implant in a contaminated or severely crushed wound guarantees infection and subsequent implant extrusion. When in doubt, primary arthrodesis or temporary placement of an antibiotic cement spacer is the safer oncologic and functional choice.
Management of Proximal Amputations (Carpus, Forearm, and Arm)
The management of the skeleton in more proximal amputations is highly varied and requires advanced skill in the handling of medullary fixation devices, bone plates, and screws. The biomechanical forces in the forearm and arm are exponentially greater than in the digits. Ischemia time becomes a critical limiting factor in major limb replantation, often dictating the choice of fixation. If the amputation level is through the carpus, shortening is easily achieved, and wrist motion can often be partially preserved by the excision of the damaged carpal bones (e.g., proximal row carpectomy). Temporary fixation is achieved with heavy transarticular Steinmann pins to stabilize the radiocarpal or midcarpal joints while the soft tissues heal.
Amputations through the forearm and arm usually require shortening of 2 to 5 cm. Distal radial metaphyseal amputations are usually fixed rapidly with crossed Steinmann pins. Plates and screws are used less often due to the time required for application and the bulk of the hardware under a potentially compromised soft-tissue envelope. Diaphyseal forearm amputations are fixed with 3.5mm dynamic compression plates (DCP) or limited contact dynamic compression plates (LC-DCP) on both bones if ischemia time permits. If time is critical, intramedullary fixation with Rush rods or Steinmann pins is utilized. Hybrid combinations are highly effective, such as rigid plate and screw fixation for the radius to restore the radial bow and pronosupination axis, combined with rapid intramedullary fixation for the ulna.
Amputations through the humerus are ideally fixed with 4.5mm dynamic compression plates to provide absolute stability. However, complex fracture configurations and strict time considerations regarding muscle ischemia may require the rapid deployment of interfragmentary Steinmann pins or intramedullary rods to establish immediate continuity before proceeding to vascular shunting or repair.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, skeletal complications in replantation surgery are frequent and can severely compromise the functional outcome. The most devastating complication is the failure of the skeletal construct leading to microvascular disruption. If the bone fixation fails, the resulting shear forces instantly thrombose the delicate venous and arterial anastomoses, leading to rapid replant demise.
Nonunion and delayed union are common, particularly in cases of severe crush injuries where periosteal stripping is extensive and the biological envelope is compromised. The incidence of nonunion in digital replantation ranges from 5% to 15%, depending on the fixation method and injury severity. Malunion, particularly rotational malunion, is a frequent technical error. Even a 5-degree rotational deformity at the metacarpal level can result in a 1.5 cm overlap at the fingertip during composite flexion, severely impairing grip.
Infection is a constant threat given the contaminated nature of traumatic amputations. Osteomyelitis necessitates aggressive surgical débridement, removal of hardware, and placement of antibiotic-impregnated cement spacers, often culminating in delayed bone grafting or eventual amputation. Joint stiffness and tendon adhesions are nearly universal complications, resulting from the combination of intra-articular trauma, prolonged immobilization, and the extensive scarring inherent to replantation.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management |
|---|---|---|---|
| Nonunion / Delayed Union | 5% - 15% | Excessive periosteal stripping, thermal necrosis, inadequate fixation | Revision osteosynthesis, autologous bone grafting (iliac crest or distal radius) |
| Rotational Malunion | 10% - 20% | Failure to use oblique K-wire, poor intraoperative assessment | Corrective osteotomy (metacarpal or phalangeal) once soft tissues mature |
| Osteomyelitis | 3% - 8% | Severe contamination, crush injury, inadequate initial débridement | Hardware removal, aggressive débridement, antibiotic spacers, IV antibiotics |
| Hardware Failure | 5% - 10% | Premature mobilization, inadequate construct rigidity, patient non-compliance | Revision fixation, conversion to arthrodesis if joint involved |
| Severe Joint Stiffness | > 50% | Prolonged immobilization, intra-articular fracture, tendon adhesions | Intensive hand therapy, tenolysis, capsulotomy, eventual arthroplasty/arthrodesis |
Salvage management for skeletal complications requires a staged approach. Once the microvascular repairs have definitively healed and the soft tissue envelope is stable (typically 3 to 6 months post-operatively), secondary reconstructive procedures can be undertaken. Corrective osteotomies, structural bone grafting, tenolyses, and capsulotomies are frequently required to maximize the functional potential of the replanted limb.
Phased Post-Operative Rehabilitation Protocols
The postoperative management of the skeletal framework in replantation is inextricably linked to the survival of the microvascular repairs and the ultimate functional outcome. A delicate balance must be struck between protecting the fragile skeletal fixation and vascular anastomoses, and initiating early motion to prevent debilitating tendon adhesions and joint contractures.
Immediately postoperatively, the limb is placed in a bulky, non-compressive dressing and a custom-molded plaster or fiberglass splint. For digital replants, the wrist is typically splinted in slight extension (20° to 30°), the MCP joints in 70° to 90° of flexion, and the IP joints in full extension. This "intrinsic-plus" position maintains the collateral ligaments of the MCP joints at their maximal length, preventing extension contractures, while preventing flexion contractures at the IP joints. However, this optimal skeletal positioning must be modified if it places undue tension on the vascular or tendon repairs.
The limb is elevated continuously on a foam wedge or suspended to promote venous drainage and minimize edema. Post-operative edema is the enemy of microvascular flow; it increases interstitial pressure, which can cause secondary venous congestion and, in severe cases, compartment syndrome. The replanted part is monitored hourly for the first 48 to 72 hours, assessing skin color, temperature, turgor, and capillary refill. Surface temperature probes and implantable Doppler probes are frequently utilized for objective monitoring.
Radiographic evaluation is performed at 2 weeks, 6 weeks, and 12 weeks to assess the progression of bone healing and monitor for hardware migration. K-wires are typically removed between 4 to 6 weeks in the clinic once clinical and radiographic signs of early union (callus formation, absence of pain at the fracture site) are present.
Early protected mobilization is initiated as soon as the skeletal fixation and tendon repairs allow, often within the first 3 to 5 days. Dynamic splinting protocols, such as the Kleinert or modified Duran protocols, are employed to provide controlled passive flexion and active extension within a safe arc of motion. The presence of rigid internal fixation, such as intraosseous wiring or mini-plates, allows for more confident early mobilization compared to single K-wire constructs. Hand therapy is a rigorous, months-long process requiring intense patient compliance and close coordination between the surgeon and the specialized hand therapist.
Summary of Landmark Literature and Clinical Guidelines
The evolution of skeletal management in replantation has been heavily guided by landmark biomechanical and clinical studies. The foundational principles established by pioneers such as Buncke and Kleinert emphasized that skeletal shortening is not a compromise, but rather an absolute necessity for microvascular survival. Their early work demonstrated that tension on microvascular anastomoses is the primary driver of intimal damage and subsequent thrombosis.
Regarding specific fixation techniques, Whitney et al. provided critical evidence-based guidance in their evaluation of clinical results comparing single K-wires, crossed K-wires, and intraosseous wires (with and without K-wire support). Although initial results showed similar early angulation deformities across all groups, intraosseous wires were found to have the lowest nonunion and complication rates. This study solidified intraosseous wiring as the gold standard for metaphyseal and peri-articular digital replantations, balancing low-profile mechanics with high compressive stability.
Current clinical guidelines from the American Society for Surgery of the Hand (ASSH) and major orthopedic trauma bodies reinforce the absolute necessity of minimizing ischemia time. Guidelines dictate that skeletal fixation must be executed swiftly, prioritizing stability over perfect anatomical reduction if ischemia time is critical. Furthermore, modern literature increasingly supports the use of primary arthrodesis for severely damaged joints in the replant setting, noting that attempts at complex joint reconstruction during the index procedure often lead to prolonged operative times, higher infection rates, and ultimately stiff, painful joints that require secondary fusion regardless. By adhering to these rigorous, evidence-based principles of bone and joint management, the orthopedic surgeon provides the essential mechanical foundation required for the survival and ultimate functional success of the replanted extremity.
