Mastering Digital Replantation and Revascularization: An Intraoperative Masterclass

Key Takeaway
This masterclass details digital replantation and revascularization, covering essential anatomy, precise intraoperative techniques, and comprehensive patient management. Fellows will learn to navigate complex injuries, perform meticulous repairs, and manage postoperative care, ensuring optimal functional outcomes for amputated or dysvascular digits. Emphasis is placed on detailed surgical execution and complication avoidance.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater. Today, we embark on one of the most intricate, demanding, and ultimately rewarding procedures in the entirety of orthopaedic surgery: digital replantation and revascularization. This surgical endeavor demands meticulous attention to detail, profound anatomical knowledge, and unwavering patience. Think of yourselves as micro-surgeons, operating on the smallest, yet most functionally critical, structures of the human hand. The integration of skeletal stability, tendon excursion, and microvascular perfusion requires a symphony of surgical disciplines executed flawlessly under the microscope.
Before we even consider making our first incision, we must solidify our understanding of our primary objectives and the precise nomenclature defining our interventions. Replantation is defined as the reattachment of a completely amputated body part. In this scenario, the digit is entirely severed from the body, exhibiting zero continuous tissue bridges. This necessitates the absolute de novo restoration of all essential structures: bone, flexor and extensor tendons, nerves, arteries, and veins. Our overarching goal is not merely tissue survival, but the salvage of a viable, sensate, and functionally superior digit compared to a prosthesis or amputation stump.

Conversely, revascularization refers to the restoration of circulation and the comprehensive repair of all injured structures in an incompletely amputated, dysvascular body part. In these complex cases, a tissue bridge remains—often consisting of contused skin, a single tendon, or a crushed nerve—but the critical arterial blood supply is critically compromised or entirely absent. Revascularization intrinsically mandates the repair or grafting of arteries to re-establish critical inflow. Finally, we must acknowledge revision amputation. Sometimes, despite our highest aspirations, replantation is physiologically contraindicated or functionally inadvisable. In such scenarios, a revision amputation is performed to achieve optimal soft tissue coverage, minimize neuroma formation, and create a highly functional stump that allows the patient an expedited return to activities.

The pathophysiology of amputations and the subsequent ischemia-reperfusion injury cascade dictate our operative timeline and success rates. When a digit is amputated, cellular hypoxia immediately initiates a shift from aerobic to anaerobic metabolism, rapidly depleting intracellular ATP stores. This metabolic crisis leads to the failure of sodium-potassium pumps, intracellular swelling, and the accumulation of toxic metabolites such as lactic acid and hypoxanthine. The duration of this ischemic window is the primary determinant of tissue viability. Furthermore, upon the restoration of blood flow—the reperfusion phase—the sudden influx of oxygen interacts with accumulated hypoxanthine to generate massive quantities of reactive oxygen species (ROS). This oxidative stress damages endothelial linings, promotes microvascular thrombosis, and can lead to the dreaded "no-reflow phenomenon," where despite a patent macroscopic anastomosis, capillary-level perfusion fails.
Mechanism of Injury and Prognostic Value
The mechanism of injury is arguably the most critical prognostic indicator we evaluate during the initial trauma bay assessment. Sharp amputations, such as those inflicted by a guillotine, a clean knife, or a high-speed table saw, represent the ideal candidates for replantation. These mechanisms produce a remarkably narrow zone of injury. The tissue disruption is localized, allowing for conservative but effective débridement and facilitating primary repair of vessels and nerves without excessive tension. The intimal damage to the vessels is minimal, drastically reducing the risk of postoperative thrombosis.
In stark contrast, crush and avulsion injuries present a formidable reconstructive challenge. These mechanisms impart tremendous kinetic energy to the tissues, resulting in substantially increased cellular death and a wide zone of injury that extends far proximal and distal to the visible amputation site. Avulsion injuries, often sustained when a ring catches on a moving object or during agricultural accidents, physically tear the neurovascular bundles from their origins. The intimal lining of the arteries may be stripped away for centimeters beyond the gross laceration. This extensive damage strictly prohibits primary anastomosis; attempting to suture these contused vessels together guarantees failure. Instead, these injuries necessitate aggressive resection back to healthy, pulsatile intima and the mandatory utilization of interpositional vein grafts.

Concomitant systemic injuries must always be evaluated before focusing on the extremity. While most digit amputations are isolated events, high-energy trauma can produce polytrauma scenarios. Adherence to Advanced Trauma Life Support (ATLS) protocols is non-negotiable. Life-threatening injuries—airway compromise, massive hemorrhage, tension pneumothorax—always take absolute precedence over limb salvage. A patient cannot utilize a perfectly replanted digit if they do not survive the initial trauma. Only once the patient is hemodynamically stable and cleared by the trauma team do we shift our focus to the microvascular reconstruction of the hand.
Detailed Surgical Anatomy and Biomechanics
An exhaustive, three-dimensional understanding of digital anatomy, from the metacarpophalangeal (MCP) joint to the distal tuft, is the absolute bedrock of successful replantation. The surgeon must navigate the complex interplay of the flexor mechanism, the intricate extensor hood, and the delicate neurovascular bundles. The thumb, presenting unique anatomical variations such as the adductor pollicis insertion and a distinct pulley system (oblique pulley), requires specific biomechanical consideration compared to the lesser digits.
The Flexor Tendon and Pulley System
The flexor tendons of the hand are marvels of biological engineering, designed to transmit immense force while navigating tight anatomical constraints. The Flexor Digitorum Profundus (FDP) tendon inserts distally at the palmar base of the distal phalanx. It is the sole flexor of the distal interphalangeal (DIP) joint and is critical for power grip and fine pinch. The Flexor Digitorum Superficialis (FDS) tendon, responsible for proximal interphalangeal (PIP) joint flexion, bifurcates into two slips that insert into the midportion of the middle phalanx.

Crucially, the FDS splits, and its relative position to the FDP tendon switches from palmar to dorsal at a highly specialized anatomical structure known as Camper’s chiasm. This ingenious spatial arrangement allows the deeper FDP tendon to emerge superficially and continue its path distally to its insertion without biomechanical impingement. During replantation, particularly in Zone II injuries, the meticulous repair of both tendons is ideal for optimal independent joint motion, though isolated FDP repair may be elected in severely comminuted or contaminated wounds to minimize the risk of restrictive adhesions.
Encasing these flexor tendons is the fibro-osseous sheath, characterized by discrete, thickened bands known as pulleys. There are five annular pulleys (A1-A5) and three cruciform pulleys (C1-C3). The annular pulleys are robust, rigid structures that prevent bowstringing of the flexor tendons during contraction, thereby maintaining the mechanical advantage and moment arm of the tendon. The odd-numbered annular pulleys (A1, A3, A5) are strategically located over the palmar plates of the MCP, PIP, and DIP joints, respectively. The even-numbered annular pulleys (A2, A4) are situated over the diaphyses of the proximal and middle phalanges.
The A2 and A4 pulleys are the most critical in preventing significant bowstringing and must be preserved or reconstructed whenever surgically possible. Their loss severely compromises grip strength, reduces functional tendon excursion, and leads to flexion contractures. The cruciate pulleys, in contrast, are thin and collapsible, accommodating the significant changes in tendon sheath geometry during full finger flexion without buckling.
Extensor Anatomy and Neurovascular Spatial Relationships
The extensor mechanism is a highly complex, interconnected web of tendons and ligaments. Each lesser digit receives a primary extensor tendon from the extensor digitorum communis (EDC). The index finger possesses a secondary extensor, the extensor indicis proprius (EIP), located ulnar to the EDC, while the small finger has the extensor digiti minimi (EDM), also positioned ulnar to its respective EDC slip. These accessory tendons provide independent extension and are crucial for fine motor control. At the PIP joint, the extensor tendon divides into a central slip, which inserts on the base of the middle phalanx to extend the PIP joint, and lateral bands, which converge distally to form the terminal tendon inserting on the distal phalanx.

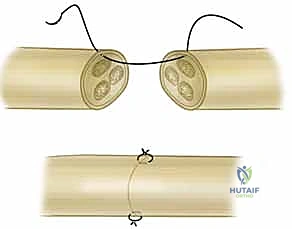
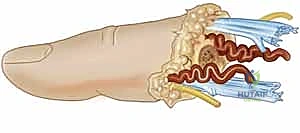
The neurovascular supply to the digits is highly organized and predictable, a fact we rely heavily upon during microscopic dissection. Each digit is supplied by a radial and an ulnar proper digital artery, which travel alongside their respective radial and ulnar proper digital nerves. A critical anatomical relationship to memorize is that at the level of the digit, the artery consistently lies dorsal to the nerve. This relationship dictates our surgical approach; we typically identify the larger, more superficial nerve first and dissect dorsally to locate the artery. The digital nerves are sensory-only, containing one to three distinct fascicles, and trifurcate at the level of the DIP joint to innervate the highly sensitive digital pulp.
Supporting the neurovascular bundles are distinct fibrous septa. Palmar and dorsal cutaneous ligaments play a vital role in maintaining the stable position of the bundle during the digit's full range of motion. Grayson’s ligament is situated palmar to the neurovascular bundle, originating from the flexor tendon sheath and inserting into the overlying skin. Conversely, Cleland’s ligament travels dorsal to the neurovascular bundle, extending from the phalanx to the skin. These ligaments must often be released during dissection to mobilize the vessels for tension-free anastomosis.

Digital Arches and the Venous Network
The arterial supply forms a redundant network via three major palmar arches that consistently arise from the digital arteries: the proximal arch at the level of the C1 pulley, the middle arch at the C3 pulley, and the distal arch just proximal to the FDP insertion. This collateral circulation is why repairing a single digital artery can often salvage an entire digit. However, be aware of digital artery dominance. The ulnar digital artery is typically dominant (larger caliber) in the thumb and index finger, while the radial digital artery is usually dominant in the small finger. The middle and ring fingers exhibit more variability.
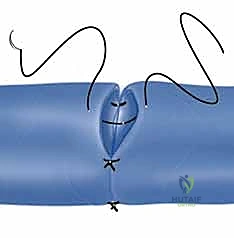
The venous system is equally critical; a replanted digit will fail just as quickly from venous congestion as it will from arterial insufficiency. Injection studies demonstrate that the venous system consists of a complex series of arcades on both the dorsal and palmar surfaces. Clinically, the dorsal veins are of paramount importance. They generally have a larger caliber, thinner walls, and are more anatomically consistent, making them the primary targets for venous anastomosis. The palmar veins are smaller, more friable, and do not consistently travel with the neurovascular bundle, making them secondary targets used only when dorsal veins are unavailable or severely traumatized.
Exhaustive Indications and Contraindications
The decision to replant an amputated digit is among the most nuanced in hand surgery, requiring the surgeon to balance technical feasibility with the patient's ultimate functional outcome, physiological reserve, and psychological resilience. The mere presence of an amputated part does not mandate replantation. A poorly functioning, insensate, stiff, and painful replanted digit is a significant detriment to the patient, often resulting in worse overall hand function than a well-constructed revision amputation.

Absolute indications for replantation are scenarios where the functional deficit of amputation is so severe that the risks of surgery are heavily outweighed by the potential benefits. The thumb is paramount; it provides 40-50% of total hand function through its unique ability to oppose the other digits. Any amputated thumb, regardless of the level, should be considered for replantation. Multiple digit amputations also constitute an absolute indication, as the loss of multiple fingers devastatingly impairs grip strength and hand mechanics. Furthermore, any amputation in a pediatric patient is an absolute indication. Children possess extraordinary regenerative capabilities, neuroplasticity, and adaptability, often achieving functional outcomes that would be impossible in adults. Finally, amputations through the palm, wrist, or forearm (macro-replantations) are generally indicated due to the massive functional loss associated with proximal amputations.
Relative indications require careful clinical judgment. Single digit amputations distal to the FDS insertion (Zone I) are often replanted primarily for cosmetic reasons and to preserve the nail complex, though functional gains in grip strength are minimal. In contrast, single digit amputations in Zone II (the "no man's land" between the A1 pulley and FDS insertion) are highly controversial. Historically, these were considered contraindications due to the high likelihood of severe tendon adhesions and profound stiffness. However, advances in microsurgical technique and early active motion rehabilitation protocols have made Zone II single-digit replantations viable in highly selected, compliant patients.
Contraindications must be strictly adhered to in order to prevent patient morbidity. Absolute contraindications include life-threatening concomitant injuries (the "life over limb" principle), severe crush or avulsion injuries with a zone of injury so extensive that vascular reconstruction is impossible, and prolonged ischemia times that exceed the viability threshold of the tissues. Relative contraindications involve severe medical comorbidities (e.g., advanced peripheral vascular disease, uncontrolled diabetes, hypercoagulable states) that preclude prolonged anesthesia or jeopardize microvascular patency. Active, heavy tobacco use is a profound relative contraindication, as nicotine-induced vasospasm significantly increases the risk of anastomotic failure. Finally, severe psychiatric instability or a history of self-inflicted amputation strongly predicts non-compliance with the arduous postoperative rehabilitation protocol, often leading to functional failure.
Replantation Decision Matrix
| Clinical Scenario | Indication Level | Rationale / Considerations |
|---|---|---|
| Thumb Amputation | Absolute Indication | Thumb provides ~50% of hand function; opposition is critical. |
| Multiple Digits | Absolute Indication | Preserves essential grip span and pinch mechanics. |
| Pediatric Patient | Absolute Indication | Superior nerve regeneration and neuroplasticity in youth. |
| Zone I Single Digit | Relative Indication | Primarily for cosmesis and nail preservation; minimal functional gain. |
| Zone II Single Digit | Relative Indication | High risk of stiffness; requires perfect technique and highly compliant patient. |
| Severe Crush/Avulsion | Contraindication | Extensive intimal damage; high risk of thrombosis even with vein grafts. |
| Prolonged Ischemia | Contraindication | >6h warm ischemia (muscle), >12h cold ischemia (digits). Risk of reperfusion toxicity. |
| Unstable Polytrauma | Absolute Contraindication | ATLS protocol: Life preservation supersedes limb salvage. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a replantation begins long before the microscope is draped. It begins in the Emergency Department with a rapid, systematic evaluation. Eliciting a precise history regarding the mechanism of injury (e.g., clean table saw versus a dirty agricultural auger) informs the surgeon about the potential for contamination and the expected zone of injury. Ischemia time must be calculated immediately. Warm ischemia time for digits should ideally be less than 6 hours, while cold ischemia time can be tolerated for up to 12 hours.
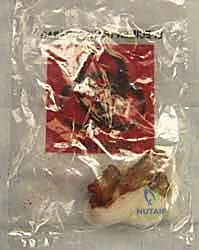
Proper transportation of the amputated part is a non-negotiable standard of care. The part must never be placed directly on ice, as this induces irreversible frostbite and cellular lysis. The correct method involves wrapping the amputated part in sterile gauze moistened with Ringer’s lactate or normal saline. This wrapped part is sealed in a leak-proof plastic bag, which is then submerged in a secondary container filled with a slurry of ice and water. This achieves the optimal target temperature of approximately 4°C, drastically reducing metabolic demand, slowing bacterial proliferation, and extending the viable ischemia window.
During the physical examination, specific pathognomonic signs of avulsion injury must be identified. The "red-line sign" is a longitudinal streak of ecchymosis along the lateral border of the digit, resulting from hemorrhage of avulsed branches of the digital artery following extreme traction. The "ribbon sign" is visible upon direct inspection of the amputated stump; it describes the tortuous, coiled appearance of the avulsed artery, indicating severe disruption of the tunica intima and media. When these signs are present, the surgeon must immediately anticipate the need for extensive arterial resection and interpositional vein grafting.
Standard anteroposterior and lateral radiographs of both the injured extremity and the amputated part are mandatory. These images allow for precise preoperative templating. The surgeon must assess the level of bone loss, the degree of comminution, and the involvement of articular surfaces. This dictates the method of skeletal fixation—whether longitudinal K-wires, interosseous wiring, or miniature plates will be required.
In the operating room, patient positioning is critical for surgeon ergonomics during a procedure that may last 6 to 12 hours. The patient is positioned supine with the arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the upper arm. Anesthesia is typically a prolonged regional block (e.g., axillary or supraclavicular brachial plexus block) combined with general anesthesia. Regional anesthesia provides the distinct advantage of a sympathectomy effect, inducing profound peripheral vasodilation which dramatically aids microvascular perfusion in the immediate postoperative period.
Step-by-Step Surgical Approach and Fixation Technique
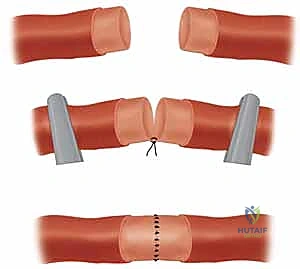
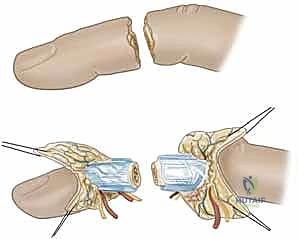
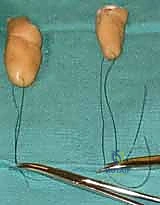
The sequence of surgical repair in digital replantation is highly standardized, designed to optimize exposure, minimize iatrogenic injury, and sequentially build stability. The classic sequence is: 1) Identification and tagging of structures, 2) Bone debridement and shortening, 3) Skeletal fixation, 4) Extensor tendon repair, 5) Flexor tendon repair, 6) Arterial anastomosis, 7) Nerve repair, 8) Venous anastomosis, and 9) Skin coverage. Some surgeons prefer to repair veins prior to arteries to minimize blood loss and maintain a bloodless field for the venous anastomosis, though this can lead to venous congestion if the arterial inflow is not established promptly.

The procedure commences with thorough, aggressive debridement of both the amputated part and the proximal stump under loupe magnification. All devitalized tissue, foreign debris, and contaminated
Clinical & Radiographic Imaging Archive