Revascularization and Replantation of the Digits L. Scott Levin

Introduction and Epidemiology
Replantation is strictly defined as the surgical reattachment of a completely amputated body part, a procedure that mandates the meticulous restoration of both arterial inflow and venous outflow to ensure tissue survival. In contrast, revascularization refers to the restoration of circulation and the comprehensive repair of injured structures in an incompletely amputated, dysvascular body part. By definition, revascularization inherently requires the repair or reconstruction of blood vessels to reestablish perfusion to the compromised distal segment. Revision amputation, or terminalization, is the surgical procedure performed at the amputation site to secure stable, sensate soft tissue coverage, address concomitant osseous and tendinous injuries, and optimize the functional length of the residual limb to facilitate early rehabilitation.
The clinical decision matrix dictating whether to proceed with replantation, revascularization, or revision amputation is highly multifactorial. It necessitates a rigorous assessment of patient demographics, systemic comorbidities, the specific mechanism of injury, warm and cold ischemia times, and the patient's occupational and functional demands. The advent of clinical microsurgery in the 1960s fundamentally revolutionized the management algorithm for upper extremity amputations. Following the seminal first successful arm replantation by Malt and McKhann in 1962, and the first successful microvascular digit replantation by Komatsu and Tamai in 1968, the surgical techniques, optical magnification, and ultrafine instrumentation required for microvascular surgery have undergone profound evolution.
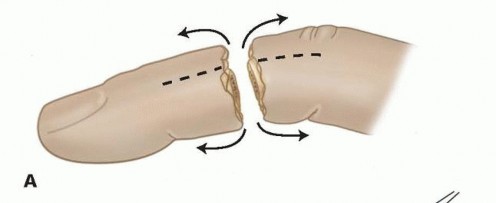
From an epidemiological standpoint, digital amputations disproportionately affect young, working-age males. These injuries frequently result from occupational hazards involving heavy industrial machinery, table saws, or severe crush mechanisms. The mechanism of injury remains the single most critical prognostic determinant of both graft survival and ultimate functional outcome. Sharp, guillotine-type amputations present the most favorable physiological scenario for replantation, as the zone of injury is highly localized. Conversely, crush, avulsion, and degloving injuries inflict extensive, longitudinal zones of trauma on the neurovascular bundles, inducing widespread intimal damage that severely compromises the viability and patency of microvascular anastomoses.

Surgical Anatomy and Biomechanics
An exhaustive, three-dimensional understanding of digital anatomy over its complete longitudinal extent is an absolute prerequisite for successful replantation and the subsequent restoration of biomechanical function. The anatomical architecture of the thumb differs significantly from that of the four lesser digits, particularly regarding its intrinsic musculotendinous insertions, degrees of freedom, and vascular dominance.
Ligamentous Architecture
The palmar and dorsal cutaneous ligaments are critical for maintaining the anatomical position of the neurovascular bundle during the full arc of digital motion. Grayson's ligament is situated palmar to the neurovascular bundle; it originates from the volar aspect of the flexor tendon sheath and inserts directly into the volar skin. Its primary biomechanical function is to stabilize the volar skin during active flexion, preventing cutaneous bunching. Cleland's ligament travels dorsal to the neurovascular bundle, extending from the lateral aspect of the phalanges to the overlying lateral skin. Cleland's ligament serves as a robust, crucial protective barrier for the neurovascular bundle during digital motion and is typically preserved during the surgical dissection of the neurovascular pedicles.

Vascular Anatomy
A radial and ulnar proper digital artery supplies each digit, traveling in tandem with their respective radial and ulnar proper digital nerves. At the level of the digit, the proper digital artery consistently lies dorsal to the digital nerve. Vessel dominance exhibits predictable anatomical variance. The ulnar digital artery is typically larger in caliber and dominant in the thumb and index fingers. Conversely, the radial digital artery usually exhibits a larger caliber and dominance in the small finger. The middle and ring fingers exhibit variable dominance.
Three major palmar arches arise from the digital arteries, providing critical collateral circulation across the volar surface. The proximal, middle, and distal arches are consistently located at the level of the C1 pulley, the C3 pulley, and immediately distal to the flexor digitorum profundus (FDP) insertion, respectively. Furthermore, four palmar and four dorsal branches typically extend from each digital artery to supply the integumentary and osseous structures.

Microangiographic injection studies have demonstrated that the venous system of the digit consists of a complex series of arcades on the dorsal and palmar surfaces, interconnected by oblique and transverse anastomotic bridging veins. The dorsal veins possess a significantly larger caliber and thinner walls than the palmar veins, making them the primary targets for venous anastomosis during replantation. Unlike the arterial system, the palmar veins do not consistently travel in a predictable anatomical relationship with the digital artery and nerve.

Neural Anatomy
A radial and ulnar proper digital nerve travels with each proper digital artery. The digital nerve is entirely sensory and typically contains one to three distinct fascicles surrounded by a well-defined epineurium. It reliably trifurcates at the level of the distal interphalangeal (DIP) joint to provide critical tactile sensation to the fingertip pad and the nail bed complex.
Musculotendinous and Pulley Anatomy
Each lesser digit contains two flexor tendons within a highly specialized fibro-osseous flexor tendon sheath. The FDP tendon inserts at the proximal volar base of the distal phalanx, mediating active flexion of the DIP joint. The flexor digitorum superficialis (FDS) tendon inserts as two distinct slips into the midportion of the middle phalanx. Biomechanically, the FDS tendon splits into two slips, and its relative position to the FDP tendon switches from palmar to dorsal at Camper's chiasm. This complex anatomical decussation allows the deeper FDP tendon to pass through and continue to its more distal insertion point.
The flexor mechanism is stabilized by a series of five annular (A1-A5) and three cruciform (C1-C3) pulleys, which represent discrete, localized thickenings of the fibro-osseous sheath. The annular pulleys prevent biomechanical bowstringing of the flexor tendons during active flexion, whereas the cruciate pulleys are thin and collapsible, accommodating the mechanical deformation of the sheath during finger flexion. The odd-numbered annular pulleys (A1, A3, A5) are located over the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and DIP joints, respectively. The even-numbered annular pulleys (A2, A4) are located over the proximal and middle phalanges. The A2 and A4 pulleys are mechanically the most vital structures for preventing bowstringing and must be meticulously preserved or reconstructed during replantation.
On the dorsal aspect, each lesser digit receives a tendon from the extensor digitorum communis (EDC). The index and small fingers possess independent extensor function via a second proprietary extensor tendon, the extensor indicis proprius (EIP) and extensor digiti minimi (EDM), respectively. Both of these proprietary tendons are positioned ulnar to the EDC tendons at the level of the MCP joint.
Indications and Contraindications
The surgical decision to proceed with replantation versus revision amputation is highly nuanced and demands mature clinical judgment. The surgeon must systematically evaluate the mechanism of injury, the anatomical level of amputation, ischemia time, patient age, occupational requirements, and systemic comorbidities.

Absolute indications for replantation include amputations of the thumb (given its contribution to 40-50% of hand function), multiple digit amputations, amputations in pediatric patients (due to superior neural plasticity and regenerative capacity), and amputations occurring at the wrist or forearm level. Single digit amputations distal to the FDS insertion (Zone I) are also strong indications for replantation, as the functional outcome, pinch grip preservation, and aesthetic restoration are generally far superior to revision amputation.
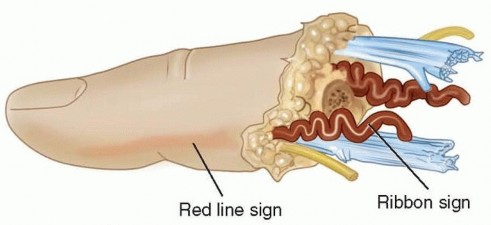
Relative contraindications include severe crush or avulsion injuries with extensive segmental vessel damage (evidenced by the "red line" or "ribbon" signs in the intima), prolonged ischemia time (greater than 12 hours of warm ischemia or 24 hours of cold ischemia for digits lacking muscle bellies), and single digit amputations proximal to the FDS insertion (Zone II). In Zone II amputations in adults, the high risk of profound post-operative stiffness may severely compromise overall hand function, often making revision amputation the more functional choice. Absolute contraindications include life-threatening concomitant injuries requiring damage control surgery, severe systemic illnesses precluding prolonged general anesthesia, and profound psychiatric instability or self-inflicted amputations.

| Clinical Scenario | Operative Replantation Indicated | Revision Amputation Indicated |
|---|---|---|
| Thumb Amputation | Yes (Absolute indication at any level) | No (Unless severe crush/completely non-viable) |
| Multiple Digits | Yes (Attempt to restore pinch/grasp) | No (Salvage parts for "spare parts" concept) |
| Pediatric Patient | Yes (High success rate, superior neural plasticity) | No (Only if tissues are completely non-viable) |
| Single Digit Zone I | Yes (Distal to FDS insertion) | Relative (Based on patient preference/comorbidities) |
| Single Digit Zone II | Relative (High risk of PIP joint stiffness) | Yes (Often preferred in heavy manual laborers) |
| Severe Avulsion/Crush | No (Extensive intimal damage, high thrombosis rate) | Yes (Primary closure, bone shortening, or local flap) |
| Prolonged Ischemia | No (>12h warm / >24h cold for digits) | Yes (Avoid systemic reperfusion toxicity/myoglobinuria) |

Pre Operative Planning and Patient Positioning
Successful replantation begins with aggressive and appropriate management in the emergency department. The amputated part must be managed meticulously to halt cellular metabolism and minimize warm ischemia time. The part should be wrapped in saline-moistened gauze, placed inside a sealed, watertight plastic bag, and then immersed in an ice-water slurry. Direct contact between the amputated tissue and ice must be strictly avoided to prevent frostbite and irreversible cellular necrosis.

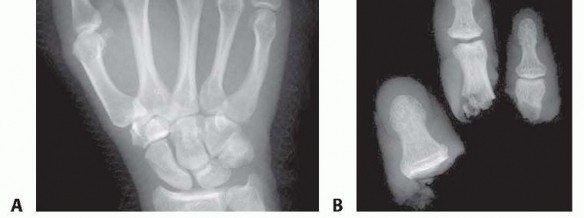
Standard orthogonal radiographs (AP and Lateral) of both the proximal amputation stump and the amputated part are mandatory. These are utilized to assess remaining bone stock, joint integrity, and the feasibility of osteosynthesis. The patient is evaluated for tetanus prophylaxis, and broad-spectrum intravenous antibiotics (typically a first-generation cephalosporin, escalated for heavily contaminated wounds) are initiated immediately.

In the operating theater, the patient is positioned supine with the affected extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Because replantation procedures are typically lengthy, patient positioning must account for pressure point padding, deep vein thrombosis prophylaxis (SCDs), and rigorous core temperature management using forced-air warming blankets. Maintaining normothermia is critical to prevent peripheral vasospasm. Anesthesia is generally achieved via a continuous regional block (axillary or supraclavicular) supplemented with intravenous sedation or general anesthesia. Regional anesthesia is highly advantageous as it provides a robust sympathectomy, thereby maximizing peripheral vasodilation and optimizing distal microvascular flow.
Detailed Surgical Approach and Technique
The surgical sequence of replantation is strategically designed to minimize ischemia time while providing a stable, rigid foundation for subsequent delicate microvascular anastomoses. The classic, widely accepted sequence is: Bone fixation, Extensor tendon repair, Flexor tendon repair, Arterial anastomosis, Nerve repair, Venous anastomosis, and Skin closure. However, some microsurgeons advocate for repairing the dorsal structures (extensor tendon and veins) before the volar structures to minimize the need to flip the digit multiple times, which can torque and traumatize fresh anastomoses.
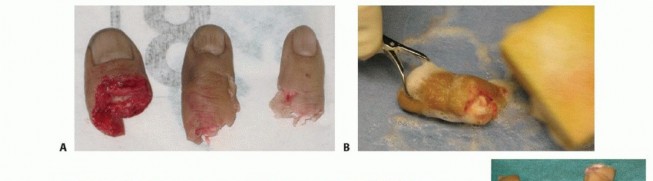
Preparation of the Amputated Part
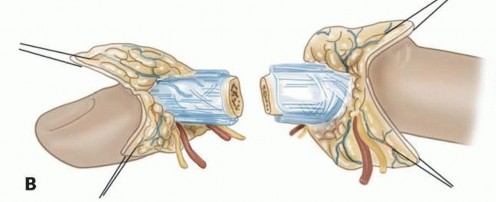
While the patient is being anesthetized and the proximal stump prepared, a second surgical team prepares the amputated part on a separate back table under loupe magnification or the operating microscope. The neurovascular bundles are carefully dissected, identified, and tagged with micro-hemoclips or fine sutures (e.g., 8-0 nylon). The vessels are flushed gently with heparinized saline to clear microthrombi and assess for intimal damage. Debridement must be aggressive and uncompromising; all devitalized, crushed, or contaminated tissue is excised until healthy, bleeding edges are encountered.

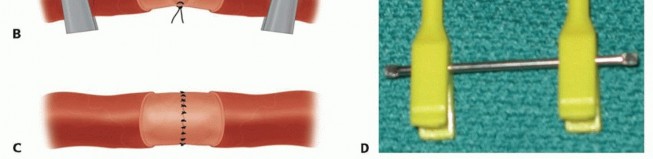
Osteosynthesis Techniques
Bone shortening is a fundamental, non-negotiable principle of replantation. Shortening the bone by 5 to 10 millimeters reduces tension on the subsequent neurovascular and tendinous repairs, frequently eliminating the need for interpositional vein or nerve grafts. Fixation must be rigid enough to allow early mobilization but low-profile enough to avoid soft tissue impingement. Common techniques include crossed or parallel Kirschner wires, intraosseous 90-90 wiring, or low-profile titanium mini-plates and screws. If the amputation occurs directly through a joint, primary arthrodesis is typically performed at a functional angle (e.g., 30 degrees of flexion for the PIP joint).

Tendon Repair
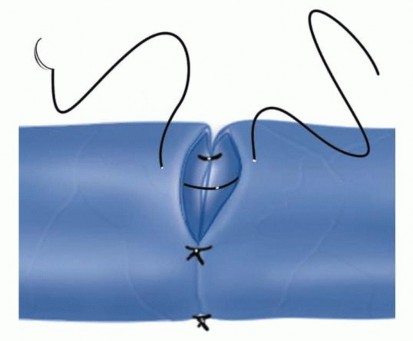
Extensor tendons are repaired using a non-absorbable synthetic suture in a figure-of-eight or horizontal mattress configuration. The FDP is repaired using a robust core suture technique (e.g., a 4-strand or 6-strand modified Kessler or cruciate repair using 3-0 or 4-0 core suture) supplemented by a running epitendinous suture (e.g., 6-0 prolene) to facilitate smooth gliding within the fibro-osseous sheath and increase construct strength. The FDS is often excised to prevent crowding and subsequent adhesions within the fibro-osseous canal, unless the amputation is very proximal and isolated FDS function is deemed critical.
Microvascular Anastomosis
Vascular repair is performed under the operating microscope using 9-0 to 11-0 nylon sutures. The tourniquet is deflated prior to arterial anastomosis to identify the proximal pulsatile vessel and ensure adequate inflow. The adventitia is stripped back precisely to prevent it from being dragged into the lumen, which is a primary, iatrogenic cause of microvascular thrombosis. The intima is inspected under high magnification; any evidence of the "red line" sign (subintimal hemorrhage), contusion, or intimal separation dictates further resection until normal vessel wall is reached. If this resection results in a tension-mismatch, a reversed interpositional vein graft (typically harvested from the distal volar forearm or volar wrist) is mandatory.
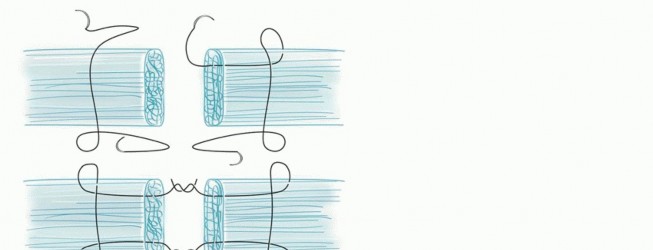
Following arterial repair, the microvascular clamps are released to confirm robust capillary refill and brisk bleeding from the distal wound edges. Venous anastomosis is then performed on the dorsal aspect of the digit. A general surgical tenet is to repair two veins for every one artery to ensure adequate outflow, accommodate post-operative edema, and prevent catastrophic venous congestion.

Neurorrhaphy
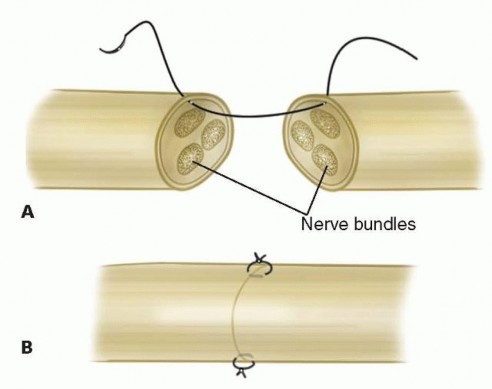
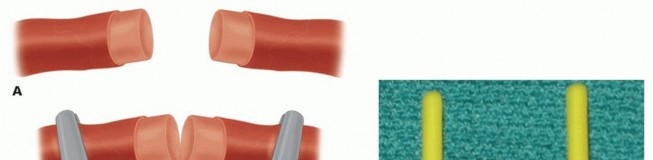
Primary epineurial repair of the proper digital nerves is performed using 9-0 or 10-0 nylon under the microscope. The repair must be entirely tension-free to allow for optimal axonal regeneration. If primary approximation is impossible due to the zone of injury or required resection, nerve conduits (for gaps <3cm) or autologous nerve grafts (e.g., medial antebrachial cutaneous nerve or sural nerve) are utilized.
Soft Tissue Coverage
Skin closure must be exceptionally loose. Circumferential tight sutures will inevitably lead to venous congestion and subsequent arterial thrombosis as post-operative edema peaks over the first 48 hours. If primary closure causes any tension over the vascular pedicles, local advancement flaps (e.g., V-Y advancement), full-thickness skin grafts, or simply allowing the wound to heal by secondary intention are employed. Prophylactic fasciotomies of the digit or hand may be indicated in cases of prolonged ischemia, severe crush injuries, or massive fluid resuscitation.

Complications and Management
The post-operative period following digit replantation is fraught with potential complications, requiring vigilant monitoring. The most catastrophic complication is vascular thrombosis, which threatens the survival of the replant.
Arterial thrombosis typically presents within the first 12 to 24 hours. Clinically, the digit will appear pale or white, with a complete loss of tissue turgor, absent capillary refill, and a drop in surface temperature. Venous congestion, conversely, usually manifests between 24 and 72 hours post-operatively. The digit appears cyanotic or violaceous, heavily swollen, and exhibits an abnormally rapid capillary refill. Pricking the skin with a needle yields dark, venous blood rather than bright red arterial blood.
If surgical exploration and revision of the venous anastomosis are not technically feasible or fail, medicinal leeches (Hirudo medicinalis) are utilized to salvage the congested digit. Leeches secrete hirudin, a potent local direct thrombin inhibitor, and actively decongest the tissue through feeding and subsequent prolonged oozing from the bite site. Patients undergoing leech therapy must receive prophylactic antibiotics (e.g., Ciprofloxacin, Ceftriaxone, or Trimethoprim-Sulfamethoxazole) to prevent aggressive soft tissue infection by Aeromonas hydrophila, an enteric Gram-negative bacterium symbiotic within the leech gut.
| Complication | Incidence | Clinical Presentation | Salvage Strategy |
|---|---|---|---|
| Arterial Thrombosis | 10-15% | Pale, cool digit, absent turgor, no capillary refill | Urgent surgical exploration, thrombectomy, revision with vein grafting |
| Venous Congestion | 15-20% | Blue/purple digit, engorged, rapid capillary refill | Suture removal, medicinal leeches, topical heparin pledgets |
| Infection | 5-10% | Erythema, purulent drainage, systemic signs (fever, leukocytosis) | Aggressive surgical debridement, targeted intravenous antibiotics |
| Tendon Adhesions | >50% | Loss of active range of motion, severe stiffness | Tenolysis after 6 months, only once revascularization is fully stable |
| Cold Intolerance | >80% | Severe pain and vasospasm in cold environments | Conservative management, calcium channel blockers (Nifedipine), biofeedback |
Post Operative Rehabilitation Protocols
The post-operative environment must be meticulously controlled to prevent sympathetically mediated vasospasm. The patient is kept in a warm room (ambient temperature >75°F), and strict avoidance of caffeine, nicotine, and chocolate is enforced for a minimum of four weeks, as these substances are potent vasocon
Clinical & Radiographic Imaging


You Might Also Like

