Metacarpophalangeal Joint Arthrodesis: Comprehensive Surgical Guide
Key Takeaway
Metacarpophalangeal (MCP) joint arthrodesis is a highly reliable salvage procedure for severe arthritis, instability, or deformity. The modified tension band technique by Stern and Segmüller provides robust fixation, utilizing Kirschner wires and a figure-of-eight stainless steel wire. Optimal fusion angles range from 20 to 30 degrees of flexion, depending on the digit. Meticulous joint preparation and rigid internal fixation ensure high union rates and excellent functional outcomes.
Introduction to Metacarpophalangeal Joint Arthrodesis
Metacarpophalangeal (MCP) joint arthrodesis is a definitive, highly reliable salvage procedure utilized in the management of severe joint destruction, intractable pain, and gross instability. While motion-preserving alternatives such as silicone or pyrolytic carbon arthroplasty are frequently favored—particularly in the rheumatoid hand—arthrodesis remains the gold standard for young, high-demand patients, manual laborers, and individuals with profound bone loss or unreconstructable paralytic deformities.
The primary goal of MCP joint arthrodesis is to provide a stable, painless pillar against which the thumb can effectively pinch, or to restore the functional cascade of the digits for power grip. Achieving a solid osseous union in the optimal biomechanical position requires meticulous surgical technique, precise osteotomies, and rigid internal fixation.
Clinical Pearl: The decision to fuse the MCP joint must be weighed carefully against the loss of motion. A fused MCP joint places increased biomechanical stress on the adjacent interphalangeal (IP) joints. Therefore, the status of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints must be thoroughly evaluated preoperatively.
Indications and Contraindications
Primary Indications
- Post-Traumatic Osteoarthritis: Severe articular comminution or chronic instability following high-energy trauma.
- Rheumatoid Arthritis (RA): Advanced disease with severe ulnar drift, volar subluxation, and inadequate bone stock or soft tissue integrity for arthroplasty.
- Paralytic Deformities: Intractable claw hand deformities (e.g., combined median and ulnar nerve palsy) where tendon transfers are not viable.
- Infection: Sequelae of septic arthritis resulting in joint destruction (performed after complete eradication of infection).
- Failed Arthroplasty: Salvage of a failed silicone or implant arthroplasty with significant bone loss.
Contraindications
- Active, untreated local or systemic infection.
- Severe vascular compromise to the digit.
- Non-compliant patients unable to adhere to postoperative protocols.
- Concomitant severe arthritis of the PIP and DIP joints in the same digit (relative contraindication, as a completely stiff ray severely limits hand function).
Biomechanics and Preoperative Planning
The functional utility of the hand is heavily dependent on the spatial orientation of the fused MCP joint. The optimal angle of fusion varies depending on the specific digit involved, adhering to the natural cascade of the hand.
Optimal Angles of Fusion
- Index Finger: 20 to 25 degrees of flexion. This relatively extended position optimizes pulp-to-pulp and key pinch with the thumb.
- Long Finger: 25 to 30 degrees of flexion.
- Ring Finger: 30 to 35 degrees of flexion.
- Small Finger: 35 to 40 degrees of flexion. This greater degree of flexion is critical for maintaining a strong power grip and accommodating the natural cupping of the transverse metacarpal arch.
Surgical Warning: Malrotation is the most poorly tolerated error in finger arthrodesis. Even a 5-degree rotational error at the MCP joint can result in 1.5 cm of digital overlap at the fingertips during flexion, severely impairing grip.
Patient Positioning and Anesthesia
- Anesthesia: The procedure is typically performed under regional anesthesia (brachial plexus block) or general anesthesia, depending on patient preference and anticipated surgical duration.
- Positioning: The patient is placed supine with the operative extremity extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic tourniquet is applied to the upper arm and inflated to 250 mmHg (or 100 mmHg above systolic blood pressure) following exsanguination with an Esmarch bandage.
- Fluoroscopy: A mini-C-arm must be draped and readily available to confirm osteotomy angles, hardware placement, and joint reduction.
Surgical Technique: Tension Band Arthrodesis (Stern et al.; Segmüller, Modified)
The modified tension band technique provides excellent biomechanical stability. By placing the tension band dorsally, the physiological flexion forces exerted by the flexor tendons are converted into dynamic compressive forces across the palmar aspect of the arthrodesis site.
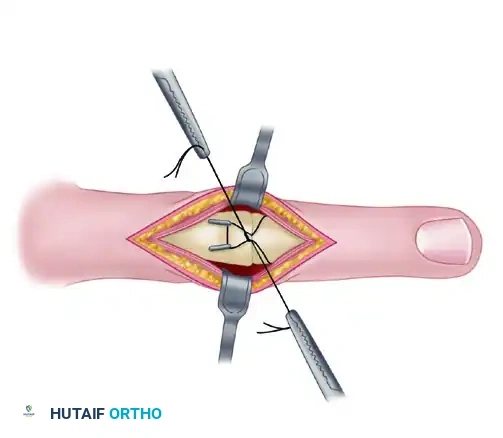
Step 1: Incision and Exposure
- Make a transverse dorsal incision directly over the metacarpophalangeal joint to be fused. Alternatively, a longitudinal incision may be utilized if multiple joints are being addressed or if future hardware removal is anticipated.
- Carefully dissect through the subcutaneous tissues, preserving the dorsal sensory branches of the radial and ulnar nerves.
- Identify the extensor mechanism. Split the extensor hood and joint capsule longitudinally, precisely in the center of the central extensor tendon.
- Retract the extensor mechanism radially and ulnarly. Remove sufficient dorsal capsule to gain comprehensive exposure of the joint.
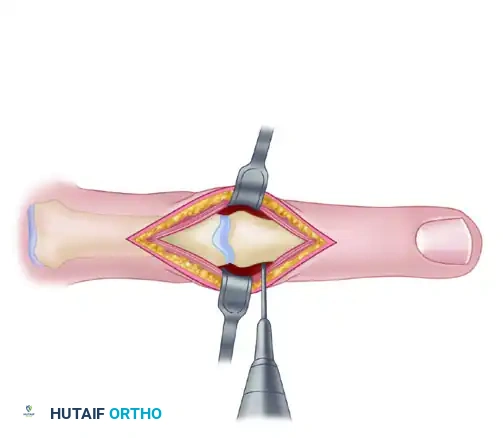
Step 2: Joint Preparation and Dislocation
- Release the collateral ligaments bilaterally from their metacarpal origins. This is a critical step that allows for full palmar flexion (the "shotgun" approach) of the joint, completely exposing the articular surfaces of both the metacarpal head and the proximal phalangeal base.
- Using a rongeur or curette, remove any remaining articular cartilage from the destroyed joint.
- Aggressively debride the subchondral bone down to healthy, bleeding cancellous bone to optimize the biologic environment for fusion.
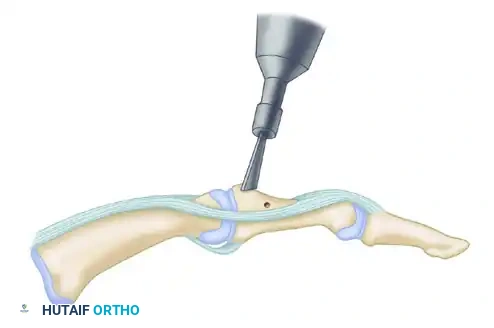
Step 3: Osteotomy and Surface Shaping
Use one of two established techniques to shape the articular surfaces:
1. Flat Cuts (Osteotome or Oscillating Saw): Resect the joint surfaces to achieve the desired angle (20 to 30 degrees, depending on the digit). The cuts must be perfectly parallel when the joint is placed in the target fusion angle.
2. Cup-and-Cone (Ball-and-Socket) Technique: Remove the metacarpal head to form a convex "ball" and ream the proximal phalangeal base to create a concave "socket." This technique is highly advantageous as it preserves digital length and allows for infinite micro-adjustments in angulation and rotation prior to definitive fixation.
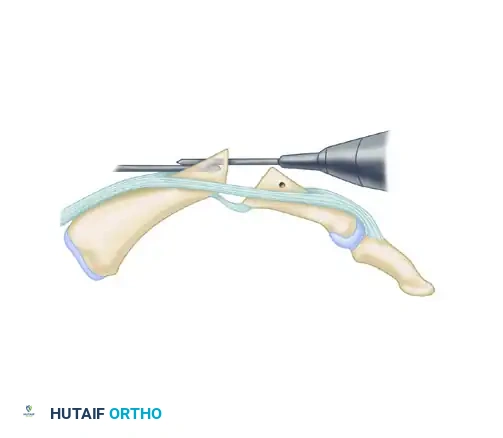
Step 4: Preparation for the Tension Band
- With a 0.028-inch Kirschner wire (K-wire), drill a transverse hole through the proximal phalanx.
- This hole must be positioned 5 to 10 mm distal to the fusion site and slightly dorsal to the midaxial line to ensure the tension band functions correctly.
- Thread a 25-gauge or 26-gauge stainless steel wire through this transverse hole, leaving equal lengths of wire on both sides.
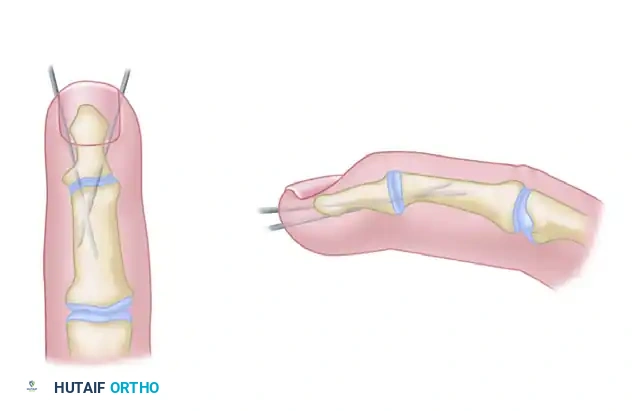
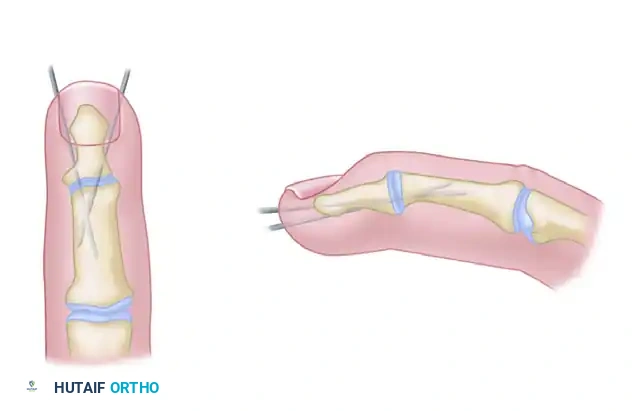
Step 5: Retrograde Kirschner Wire Insertion
- Drive two 0.028-inch or 0.035-inch K-wires retrograde into the metacarpal head.
- These wires should be directed proximally and dorsally, exiting the dorsal cortex of the metacarpal approximately 10 to 15 mm proximal to the fusion site.
- Withdraw the wires until their distal tips are flush with the resected surface of the metacarpal head.
Step 6: Joint Reduction and Antegrade Wire Advancement
- Reduce the joint, meticulously compressing the cut bone surfaces together.
- Critical Check: Assess the digit for malrotation. Flex the adjacent digits to ensure the fingertips point symmetrically toward the scaphoid tubercle.
- Once alignment is perfect, drive the K-wires antegrade across the arthrodesis site and into the proximal phalanx.
- Crucial Biomechanical Step: Seat the tips of the K-wires firmly into the palmar cortex of the proximal phalanx without penetrating it. This prevents the wires from backing out and protects the flexor tendons from irritation.
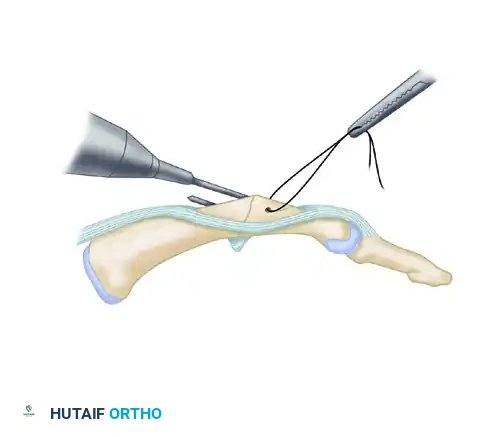
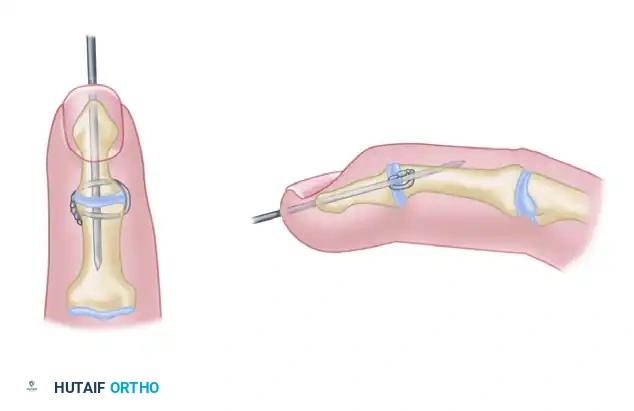
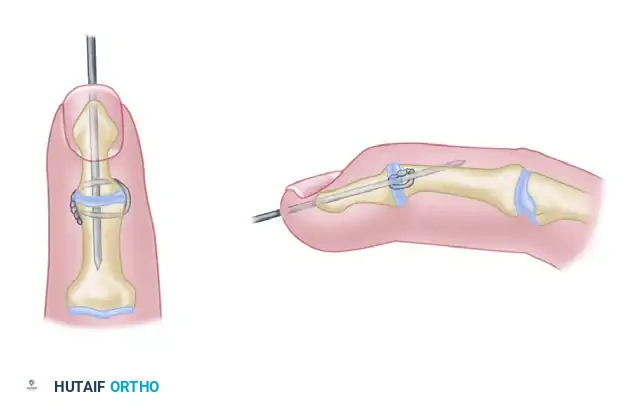
Step 7: Tension Band Application
- Loop the previously placed stainless steel wire around the protruding dorsal ends of the K-wires in a figure-of-eight manner.
- Obtain biplanar fluoroscopic radiographs to definitively assess bony apposition, the angle of fusion, and the exact position of the K-wires.
- Using a heavy needle holder or wire twister, twist the ends of the steel wire together symmetrically to generate compression across the dorsal cortex.
- Bend the proximal ends of the K-wires 180 degrees over the steel wire loops to lock the tension band in place.
- Cut the K-wires and the twisted steel wire close to the bone, burying the sharp ends deep to the extensor mechanism to prevent soft tissue irritation.
Alternative Fixation Techniques
While the tension band technique is highly effective, the thin skin over the dorsal MCP joint can sometimes make elaborate internal fixation problematic due to hardware prominence. In such cases, alternative methods are frequently employed. Union rates across these techniques remain comparable when performed correctly.
Crossed Kirschner Wires
A simple, cost-effective method involving two crossed 0.045-inch K-wires. While it lacks the dynamic compression of a tension band, it is highly effective for patients with poor soft tissue envelopes. The wires can be left proud for easy removal in the clinic after clinical union is achieved.
Interfragmentary Wire and Longitudinal K-wire
This technique utilizes a single longitudinal K-wire for axial stability, supplemented by an interosseous wire loop (often 26-gauge) placed in the dorsal cortex to provide compression and control rotation.
Headless Compression Screws (Herbert Screw)
Because of the ease of insertion and the ability to completely bury the hardware, headless compression screws (e.g., Herbert screws, Acutrak screws) are increasingly preferred by many hand surgeons.
* The screw is typically inserted antegrade from the dorsal base of the proximal phalanx into the metacarpal shaft.
* This technique provides excellent interfragmentary compression and eliminates the risk of dorsal hardware prominence, allowing the limb to heal with almost imperceptible scars.
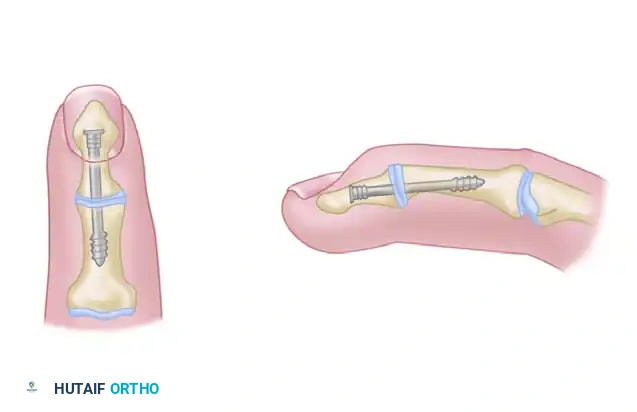
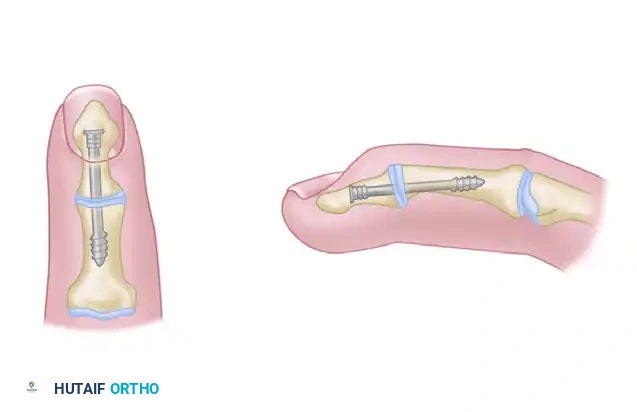
Clinical Pearl: When utilizing headless compression screws, the cup-and-cone preparation is highly recommended. It provides intrinsic stability and maximizes the cancellous bone contact area, which is vital since the screw provides compression along only a single axis.
Closure and Postoperative Protocols
Incision Closure
- Thoroughly irrigate the wound to remove bone debris.
- Repair the extensor mechanism with 4-0 absorbable sutures (e.g., Vicryl) using a continuous or interrupted technique. Ensure the tendon glides smoothly over the buried hardware.
- Close the skin with 4-0 or 5-0 non-absorbable sutures (e.g., Nylon).
Rehabilitation and Splinting
- Immediate Postoperative Phase (0-2 Weeks): The hand is placed in a bulky, non-compressive soft dressing reinforced with a volar plaster splint. The wrist is positioned in 20 degrees of extension, and the fused MCP joint is protected. Elevation is strictly enforced to minimize edema.
- First Clinic Visit (10-14 Days): Sutures are removed. If fixation is rigid (e.g., tension band or compression screw) and the patient is compliant, external splinting usually is not required for a prolonged period. A custom thermoplastic splint may be fabricated for protection during high-risk activities or sleep.
- Active Motion (2-6 Weeks): Aggressive active and active-assisted range of motion (ROM) of the PIP and DIP joints is initiated immediately to prevent tendon adhesions and joint stiffness.
- Radiographic Follow-up: Serial radiographs are obtained at 4, 8, and 12 weeks to assess for bridging trabeculae. Full unrestricted activity is permitted only after radiographic union is confirmed, typically between 8 to 12 weeks.
Complications and Pitfalls
- Nonunion: Occurs in approximately 5-10% of cases. Risk factors include smoking, inadequate bone debridement, and thermal necrosis from power saws. Treatment requires revision arthrodesis with bone grafting and rigid plate fixation.
- Malunion: Rotational malunion is a severe functional complication. It must be prevented intraoperatively by meticulously checking the digital cascade before final hardware tightening.
- Hardware Prominence: The dorsal skin over the MCP joint is thin. Prominent K-wires or wire knots can cause skin breakdown, extensor tendon irritation, or rupture. If symptomatic after union, hardware removal is indicated.
- Infection: Superficial pin tract infections (if K-wires are left exposed) are managed with oral antibiotics and local pin care. Deep infections require aggressive surgical debridement and hardware removal.
By adhering to strict biomechanical principles, ensuring meticulous joint preparation, and selecting the appropriate fixation construct, surgeons can achieve highly successful outcomes in metacarpophalangeal joint arthrodesis, restoring powerful grip and alleviating debilitating pain.
You Might Also Like