First MTP Arthrodesis and Lesser MTP Resection: A Comprehensive Surgical Guide
Key Takeaway
Arthrodesis of the first metatarsophalangeal (MTP) joint combined with resection of the lesser MTP joints is a highly effective salvage procedure for severe forefoot deformities, particularly in rheumatoid arthritis. This technique reestablishes the plantar fat pad, corrects fixed deformities, and restores weight-bearing biomechanics. Success relies on precise osteotomies, optimal hallux positioning (20 degrees valgus, 15 degrees dorsiflexion), and meticulous soft-tissue balancing to ensure a stable, plantigrade foot.
Introduction and Biomechanical Rationale
Arthrodesis of the first metatarsophalangeal (MTP) joint combined with resection arthroplasty of the lesser MTP joints is a cornerstone salvage procedure for patients presenting with severe, end-stage forefoot deformities. Historically popularized for the management of the rheumatoid forefoot, this procedure addresses the complex pathoanatomy characterized by severe hallux valgus, dorsal dislocation of the lesser toes, and the painful distal migration of the plantar fat pad.
In the classic rheumatoid foot, chronic synovitis leads to capsular distension and attenuation of the collateral ligaments and plantar plate. As the proximal phalanges dislocate dorsally, the lesser metatarsal heads are driven plantarward. This biomechanical collapse forces the protective plantar fat pad distally, leaving the prominent metatarsal heads covered only by atrophic skin, resulting in intractable plantar keratoses (IPKs) and severe weight-bearing pain.
Thompson and Mann extensively documented the efficacy of this combined approach. They demonstrated that meticulous resection of the lesser metatarsal heads, combined with a stable medial column provided by the first MTP arthrodesis, effectively reestablishes the fat pad beneath the weight-bearing metatarsal stumps. Furthermore, they noted that this reconstruction allows patients to tolerate a significantly greater variety of footwear. Notably, even if the tips of the lesser toes do not achieve full ground contact during static stance, dynamic balance and proprioception remain unimpaired.
💡 Clinical Pearl: Managing PIP Joint Deformity
While historical techniques utilized osteoclasis to correct fixed flexion contractures at the proximal interphalangeal (PIP) joints, long-term follow-up frequently revealed recurrence of the deformity. Contemporary evidence-based practice strongly favors excisional phalangeal arthroplasty—specifically, the removal of the head and neck of the proximal phalanges—to achieve durable correction of fixed PIP deformities.
Preoperative Evaluation and Surgical Planning
Thorough preoperative assessment is critical. Patients typically present with a triad of severe hallux valgus, overriding or crossover lesser toes, and painful plantar callosities.
Clinical Assessment
- Vascular Status: Given the extensive soft-tissue dissection and realignment required, robust vascular inflow is mandatory. Palpate pedal pulses and obtain non-invasive vascular studies (ABI, TBI) if any ischemic concerns exist.
- Skin Integrity: Evaluate the dorsal skin for thinning or ulceration over prominent PIP joints, and the plantar skin for ulcerated IPKs.
- Bone Quality: Rheumatoid patients frequently exhibit profound osteopenia, which dictates the choice of internal fixation (e.g., Steinmann pins vs. plate and screw constructs).
Radiographic Assessment
Weight-bearing anteroposterior (AP), lateral, and oblique radiographs of the foot are essential. Assess the degree of first MTP joint destruction, the extent of lesser MTP joint subluxation/dislocation, and the relative lengths of the metatarsals to plan the resection cascade.
Surgical Technique: First MTP Joint Arthrodesis
The procedure begins with the stabilization of the medial column. Establishing the correct length and alignment of the first ray dictates the subsequent resection levels for the lesser metatarsals.
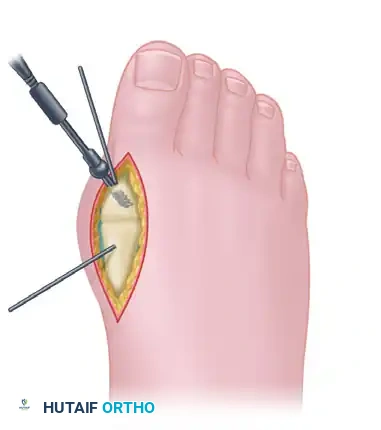
1. Incision and Exposure
- Make a dorsal longitudinal incision centered over the first MTP joint, positioned just medial to the extensor hallucis longus (EHL) tendon.
- Surgical Warning: In patients with compromised soft-tissue envelopes or those at high risk for wound healing complications (e.g., severe rheumatoid disease, chronic corticosteroid use), a direct medial approach may be preferable to avoid dorsal skin necrosis.
- Carefully identify and retract the dorsomedial branch of the superficial peroneal nerve.
- Incise the joint capsule in line with the skin incision. Perform a meticulous synovectomy, removing all hypertrophic, destructive rheumatoid synovium.
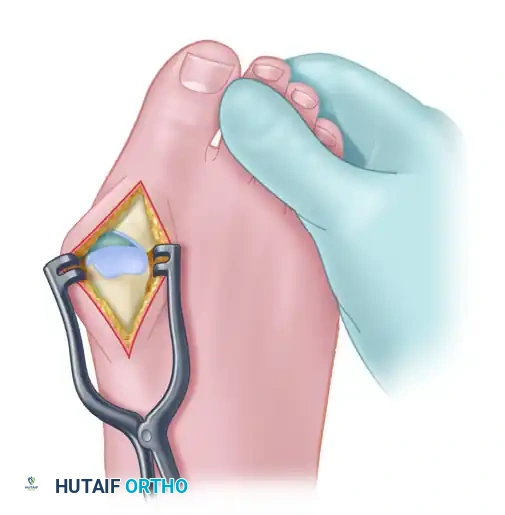
2. Joint Preparation
- Release the joint capsule medially and laterally to achieve full exposure of the articular surfaces.
- Using a sagittal saw, create a flat cut across the first metatarsal head. Remove approximately 5 mm of the distal metatarsal head.
- Critical Positioning: The saw cut must be made with the hallux held in approximately 20 degrees of valgus and 15 degrees of dorsiflexion relative to the plantar aspect of the foot (not the declinated metatarsal shaft).
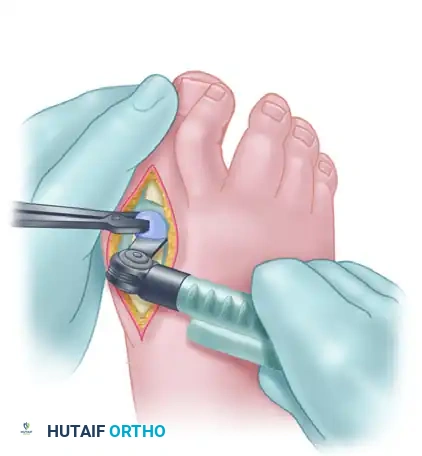
- Next, completely free the base of the proximal phalanx from its soft-tissue attachments. Excise the proximal 3 to 5 mm of the proximal phalanx.
- Ensure the osteotomy of the phalanx is perfectly parallel to the metatarsal cut while holding the toe in the aforementioned optimal position.
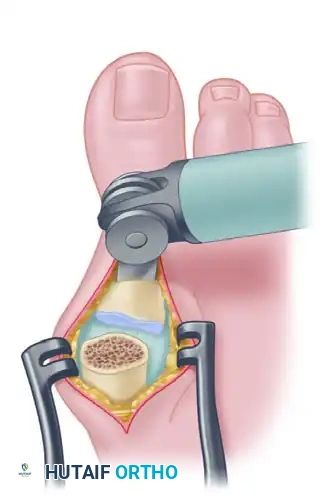
- Appose the two flat cancellous surfaces and critically evaluate the alignment.
- Alternative Technique: Commercially available cannulated conical reamers (cup and cone technique) can be utilized. This method allows for infinite multiplanar adjustment of the MTP joint position and provides excellent cancellous bone contact, though it may lack the intrinsic rotational stability of a congruent flat cut.
⚠️ Surgical Warning: Length Considerations in Rheumatoid Arthritis
In patients with rheumatoid arthritis undergoing concurrent lesser metatarsal head resections, significantly more bone must be removed from the first MTP joint compared to standard osteoarthritis cases. This compensatory shortening prevents the hallux from remaining excessively long relative to the newly shortened lesser rays, which would otherwise lead to devastating medial column overload and shoe-wear failure.
Surgical Technique: Lesser MTP Joint Resection
Once the first MTP joint is prepared (but prior to definitive fixation), attention is turned to the lesser rays.
1. Incision Strategy
- Approach the lesser MTP joints through two dorsal longitudinal incisions placed in the second and fourth web spaces.
- Begin each incision deep in the web space and extend it proximally for 3 to 4 cm.

2. Soft Tissue Dissection
- Identify the extensor tendons. Trace them distally to the base of the proximal phalanx. Note that the extensor digitorum brevis (EDB) lies slightly lateral and deep to the extensor digitorum longus (EDL).
- Transect or perform a Z-lengthening of the EDL if severe contractures are present.
- Enter the MTP joints strategically: medial to the extensor tendons for the second and third joints, and lateral to the extensor tendons for the fourth and fifth joints.
- Circumferentially free the base of the proximal phalanx from all soft-tissue attachments using sharp dissection.
- Perform a thorough synovectomy. In cases of severe, chronic dislocation, the base of the proximal phalanx may be ankylosed to the dorsal neck of the metatarsal; it must be carefully pried off before soft tissues can be fully detached.
3. Metatarsal Head Resection
- Apply longitudinal traction to the toe. Make a longitudinal incision along the dorsal aspect of the distal metatarsal.
- Strip the soft tissues medially and laterally off the distal metatarsal. Use a Freer elevator to circumferentially clear the metatarsal head and neck.
- Neurovascular Protection: Strictly limit deep dissection to the shafts of the metatarsals to preserve the common digital nerves and arteries located in the intermetatarsal spaces. Preserve dorsal sensory nerves where possible; if transection is unavoidable, coagulate them meticulously to prevent painful neuroma formation.
- Resect the lesser metatarsal heads at the level of the surgical neck. The resection must create a gentle, laterally sloping cascade to mimic the normal metatarsal parabola.
- A curved McGlamry or Hohmann retractor is highly effective for protecting plantar structures during the saw cut.
- Pitfall: Failing to remove the entire metatarsal head (e.g., leaving the plantar condyles) will inevitably result in recurrent plantar keratosis and stiffness.

4. Plantar Cyst Management
- If significant adventitial synovial cysts are present on the plantar aspect, excise only the dorsal half of the cyst.
- Use a rongeur to gently debride the underlying soft tissues.
- Crucial Step: Do not aggressively resect plantar tissue. Preserving the remaining fat is vital to ensure adequate plantar padding beneath the newly resected metatarsal stumps.
5. Final Length Balancing
- Realign the lesser toes and manually collapse the joint spaces.
- Evaluate the first MTP joint to determine if further shortening is required to match the lesser rays. Typically, an additional 1 cm of shortening is necessary. This additional bone should be resected from the first metatarsal rather than the proximal phalanx.
- The final alignment should yield a first and second toe of approximately equal length, with the third, fourth, and fifth toes forming a smooth, laterally sloping cascade.
Fixation Strategies
First MTP Joint Fixation
The choice of fixation depends heavily on the patient's bone stock.
Option A: Interfragmentary Screw and K-wires (Good Bone Stock)
* Stabilize the joint temporarily with two 0.054-inch (1.4-mm) Kirschner wires.
* If bone density permits, place a lag screw across the MTP joint from medial to lateral to achieve robust interfragmentary compression.
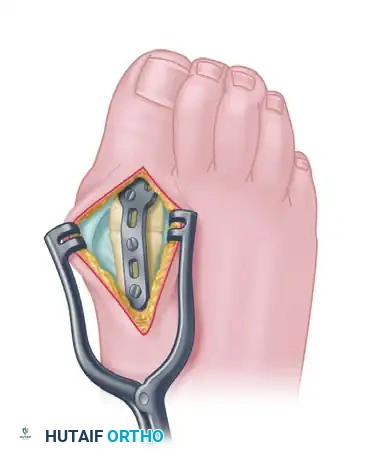
Option B: Dorsal Plate Construct (Gold Standard for Normal Bone)
* Apply a precontoured, low-profile MTP fusion plate to the dorsal aspect of the joint.
* Secure the plate using 3.2-mm or 4.0-mm cancellous screws. This provides superior biomechanical stability and allows for earlier mobilization.
Option C: Steinmann Pins (Severe Osteopenia)
* If the bone is too soft to achieve screw purchase, utilize two 1/8-inch, double-threaded Steinmann pins.
* Drill the pins in a retrograde fashion, starting at the base of the proximal phalanx and exiting through the tip of the toe.
* Reduce the joint into the perfect position, then drive the pins antegrade across the MTP joint and deep into the metatarsal shaft.
* Note: While this provides excellent stability in osteoporotic bone, it violates the interphalangeal joint and is therefore not recommended for patients with healthy bone stock.

Lesser MTP Joint Fixation
- Address severe fixed PIP deformities via excisional arthroplasty (resecting the head and neck of the proximal phalanx) or mild deformities via osteoclasis.
- Stabilize each lesser ray with a 6-inch-long, 0.054-inch (1.4-mm) Kirschner wire.
- Drive the wire retrograde through the tip of the toe, across the straightened PIP joint.
- Hold the toe in perfect alignment and advance the wire proximally across the resected MTP space and down the metatarsal shaft. Ensure the wire is embedded deeply into the base of the metatarsal for maximum stability.
Closure and Postoperative Protocol
Wound Closure
- Irrigate all wounds copiously.
- Close the subcutaneous layers with interrupted absorbable sutures (e.g., poliglecaprone 25 / Monocryl).
- Close the skin with simple interrupted non-absorbable sutures (e.g., nylon).
- Apply a meticulous, sterile, firm compression dressing to control edema and maintain alignment.
Postoperative Vascular Monitoring
🚨 Surgical Warning: The 30-Minute Rule
The circulatory status of the toes must be monitored obsessively immediately following surgery, particularly after correcting severe, chronic deformities.
* Blanching (White Toe): Indicates arterial compromise, usually because the toe has been stretched too far longitudinally along the K-wire, tethering the digital arteries.
* Cyanosis (Blue Toe): Indicates venous congestion, often because the toe has been shortened too much, causing the delicate veins to fold and kink.Protocol: If normal color does not return within 30 minutes, the postoperative compression dressing must be released immediately. If the color remains unsatisfactory after 2 hours, the longitudinal K-pin must be removed to salvage the digit.
Rehabilitation Timeline
- 0 to 24 Hours: Maintain the firm compression dressing.
- Day 1: Transition to a lighter-weight compression dressing. The patient is permitted to ambulate in a rigid-soled postoperative shoe, bearing weight on the heel and lateral border of the foot.
- 4 to 6 Weeks: The longitudinal K-wires in the lesser toes (and Steinmann pins in the hallux, if used) are removed in the clinic.
- 10 to 12 Weeks: Immobilization in the postoperative shoe is continued until clinical and radiographic evidence confirms complete arthrodesis of the first MTP joint. Transition to supportive, wide-toe-box footwear can then begin.
You Might Also Like