Upper Limb Reconstruction in Tetraplegia | Surgical Guide
Key Takeaway
Surgical rehabilitation of the upper limb in tetraplegia aims to restore independence by reconstructing elbow extension and key pinch grip. Successful outcomes rely on meticulous patient selection, adherence to the International Classification for Surgery of the Hand in Tetraplegia, and precise tendon transfer biomechanics. Reconstructive efforts typically commence at least twelve months post-injury, ensuring neurological plateau and optimal joint suppleness before executing procedures like the Moberg deltoid-to-triceps transfer.
Introduction to Upper Limb Reconstruction in Tetraplegia
Improved acute management, advanced neurosurgical interventions, and subsequent long-term care of victims of motor vehicle accidents and sporting injuries have placed increased emphasis on the functional rehabilitation of patients with tetraplegia. The demographic profile of patients who survive cervical spinal cord injuries predominantly consists of young men with 25 to 30 years of life expectancy remaining. Notably, nearly two-thirds of survivors of cervical cord-level injuries retain C6 root-level function.
Subjectively, most patients consider their quality of life to be profoundly improved by upper limb reconstructive surgery. In comprehensive surveys, three-fourths of young tetraplegic patients prioritize the restoration of hand and upper extremity function above all other neurological deficits. For these individuals, regaining the ability to feed themselves, perform independent transfers, and manage personal hygiene is often considered more critical than the restoration of lower extremity use, bladder and bowel control, or sexual function.
While few surgeons possess vast, high-volume experience in the surgical treatment of these complex patients, foundational and excellent evidence-based work has been published by pioneers such as Freehafer, Moberg, Lamb, Zancolli, Hentz, McDowell, House, and Waters. Their collective research forms the bedrock of modern tetraplegic upper limb reconstruction.
The International Classification for Surgery of the Hand in Tetraplegia
To standardize communication, surgical planning, and outcomes assessment, McDowell, Moberg, and House established a comprehensive classification scheme following the Second International Conference on Surgical Rehabilitation of the Upper Limb in Tetraplegia (Giens, France, 1984).
This classification system is bipartite, evaluating both sensory afferent status and motor efferent capacity.
Sensory Classification
The sensory afferent status is designated based on the presence of protective and tactile sensibility:
* O (Ocular): The patient relies entirely on visual cues for hand function due to the absence of tactile feedback.
* Cu (Cutaneous): The patient possesses at least 10-mm two-point discrimination in the thumb and index finger, allowing for proprioceptive and tactile feedback without requiring constant visual monitoring.
Clinical Pearl: If cutaneous sensibility is absent (Group O), visual feedback is absolutely necessary for extremity control. In such instances, reconstructive surgery should be limited to only one upper extremity. Operating on both limbs in a Group O patient deprives them of the ability to visually monitor both hands simultaneously during bimanual tasks.
Motor Classification
The motor groupings fall into ten distinct categories (0 through 9), determined by the lowest level of grade 4 (Medical Research Council grading scale) or better motor function remaining.
- Group 0: No muscle below the elbow is suitable for transfer. (Function: Elbow flexion and forearm supination).
- Group 1: Brachioradialis (BR) is grade 4+.
- Group 2: Extensor Carpi Radialis Longus (ECRL) is grade 4+. (Function: Weak or strong wrist extension).
- Group 3: Extensor Carpi Radialis Brevis (ECRB) is grade 4+. (Function: Strong wrist extension). Note: It is clinically impossible to accurately differentiate the strength of the ECRB from the ECRL without direct surgical exposure.
- Group 4: Pronator Teres (PT) is grade 4+. (Function: Wrist extension and forearm pronation).
- Group 5: Flexor Carpi Radialis (FCR) is grade 4+. (Function: Wrist flexion).
- Group 6: Finger Extensors are grade 4+. (Function: Extrinsic extension of the fingers).
- Group 7: Thumb Extensor is grade 4+. (Function: Extrinsic extension of the thumb).
- Group 8: Partial Digital Flexors are grade 4+. (Function: Weak extrinsic flexion of the fingers).
- Group 9: Lacks only intrinsics. (Function: Extrinsic flexion of the fingers).
- Group X: Exceptions. Added to accommodate patients with asymmetrical or skip lesions who do not fit neatly into the standard categories.
While motor examinations generally follow a predictable root-level pattern, asymmetrical upper extremity involvement and skip lesions in both sensory and motor function are frequently encountered.
Principles of Management and Patient Evaluation
Careful, repeated analysis of the motor and sensory status is mandatory to determine which surgical procedure is warranted. Same-level cervical spine injuries may yield vastly different physical findings, and asymmetrical procedures may be indicated for the right and left upper extremities of a single individual.
The Three Phases of Tetraplegia Management
Murphy and Chuinard developed a highly effective, structured protocol for the management of tetraplegia, divided into three phases:
1. Acute Phase:
* Stabilize the cervical spine to preserve remaining neurological function and allow early mobilization.
* Manage associated life-threatening body system problems (pulmonary, hemodynamic).
* Aggressively manage any associated upper extremity trauma (fractures, compartment syndrome).
* Institute an immediate occupational therapy program to prevent joint contractures and maintain passive joint mobility.
2. Subacute Phase:
* Begin an aggressive, holistic rehabilitation program.
* Treat associated complications (e.g., decubitus ulcers, neurogenic bladder, autonomic dysreflexia).
* Address psychological adjustment and depression.
* Perform serial examinations by the reconstructive surgeon at 3-month intervals to map the plateau of neurological recovery.
3. Reconstructive Phase:
* Ensure the patient is medically stable, psychologically well-adjusted, and that neurological recovery has definitively plateaued (minimum 12 months post-injury).
* Begin reconstruction on the side with the most intact function. If both sides are equal, begin with the dominant extremity.
* Keep the surgical treatment plan simple and goal-oriented.
* Restore active elbow extension (e.g., Moberg deltoid-to-triceps transfer) before proceeding to distal hand reconstruction.
* Restore key grip (lateral pinch).
Surgical Warning: Many patients are extremely hesitant to undergo any surgical procedure for fear of losing the minimal, precious function they have remaining. The surgeon must observe the patient performing daily activities to determine what specific additional function would best promote independence, rather than operating purely based on a theoretical anatomical deficit.
Prerequisites for Tendon Transfers in Tetraplegia
Despite a slightly different approach to tendon transfers in spinal cord injury patients compared to peripheral nerve injury patients, the fundamental biomechanical prerequisites remain absolute:
- Neurological Stability: Recovery must have ceased (wait at least 12 months).
- Spasticity Control: Uncontrolled spasticity in a donor muscle, despite grade 5 strength, strictly precludes its use in a transfer. Spasticity will overpower the transfer and lead to severe contractures.
- Pain and Paresthesias: Painful paresthesias or complex regional pain syndrome in a hand prohibit that hand from being reconstructed.
- Joint Suppleness: Wrist mobility and the natural tenodesis effect must be maintained. Contractures of the elbow (flexion/supination) or metacarpophalangeal joints (extension) must be resolved via therapy or serial casting prior to surgery.
- Muscle Selection: The donor muscle must possess adequate strength (grade 4 or 5), appropriate tension fraction, sufficient excursion (amplitude), and expendability.
Surgical Restoration of Elbow Extension
Elbow extension is lost in approximately 70% of tetraplegic patients. The inability to extend the elbow against gravity severely limits the patient's spatial reach, prevents independent wheelchair transfers, and makes pressure-relief maneuvers (push-ups) impossible. Therefore, regaining elbow extension is paramount and should be the first function achieved.
Several surgical techniques have been described for triceps substitution in patients with grade 3 or less triceps power.
Biceps-to-Triceps Transfer
Transfer of the biceps tendon posteriorly to the terminal insertion of the triceps can be performed, but only if supinator function is active and strong (Friedenberg, Zancolli). If the supinator is weak, transferring the biceps will result in a devastating loss of forearm supination. Furthermore, Zancolli reported a 24% reduction in elbow flexion strength following this procedure. Today, biceps-to-triceps transfer is generally reserved for patients with significant, recalcitrant elbow flexion contractures where weakening the flexor moment is actually desirable.
Posterior Deltoid-to-Triceps Transfer (Moberg)
The posterior deltoid-to-triceps transfer, originally described by Moberg, is the gold standard procedure for establishing elbow extension. The posterior deltoid is synergistic with elbow extension and provides excellent excursion and power. Because the deltoid lacks sufficient length to reach the olecranon directly, the procedure requires an intercalated graft (fascia lata, toe extensors, or tibialis anterior tendon).
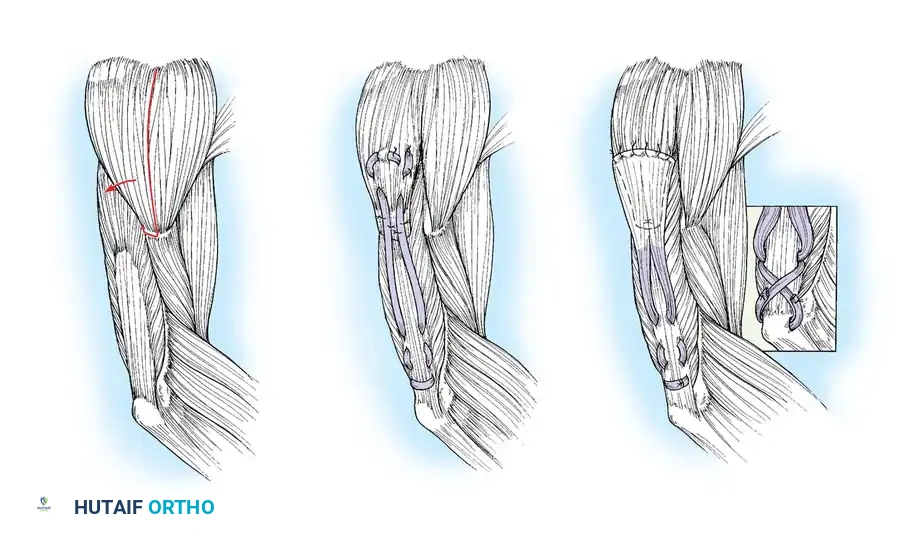
Lacey et al. reported excellent results using anterior tibial tendon grafts, noting that all patients achieved functional elbow extension and high satisfaction rates. Hentz et al. modified the procedure by utilizing fascia lata or directly attaching the deltoid to the mobilized triceps aponeurosis without a free graft, though this requires extensive mobilization.
Operative Technique: Posterior Deltoid-to-Triceps Transfer (Modified Moberg)
Patient Positioning and Preparation:
1. Place the patient in the lateral decubitus position with the operative arm draped free, allowing full, unrestricted flexion and extension of the elbow.
2. Ensure all pressure points are meticulously padded, as tetraplegic patients are at extreme risk for intraoperative decubitus ulceration.
Surgical Approach:
1. Make a 10- to 13-cm longitudinal incision along the posterior border of the deltoid muscle, extending distally toward the humeral insertion.
2. Raise thick fasciocutaneous flaps over the fascia of the deltoid to prevent skin necrosis. Identify the deltoid's humeral insertion.
3. Using a periosteal elevator and sharp dissection, elevate the posterior third to half of the deltoid tendon along with a robust strip of its periosteal insertion.
Surgical Pitfall: When splitting the deltoid muscle fibers in a distal-to-proximal direction, you must carefully palpate and visually inspect the deep surface of the muscle. The axillary nerve and posterior circumflex humeral vessels enter the muscle on its deep surface. Injury to the axillary nerve will denervate the transfer, resulting in catastrophic failure.
Graft Harvesting and Preparation:
1. Depending on surgeon preference, harvest an appropriate intercalated graft. Moberg originally utilized great toe extensors; however, the anterior tibial tendon or a robust strip of fascia lata is currently preferred due to superior tensile strength.
2. If using fascia lata, harvest a strip approximately 4 cm wide and 15 cm long. Tubularize the graft using a running locking non-absorbable suture.
Tendon Weaving and Fixation:
1. Weave the proximal end of the graft into the mobilized posterior deltoid muscle belly using a Pulvertaft weave technique. Secure it with multiple interrupted horizontal mattress sutures (e.g., 2-0 Ethibond or FiberWire).
2. Expose the distal triceps tendon and olecranon via a separate posterior longitudinal incision.
3. Create a longitudinal split in the triceps aponeurosis.
4. Pass the distal end of the graft subcutaneously from the proximal incision to the distal incision. Ensure the subcutaneous tunnel is wide enough to allow unhindered gliding of the graft.
Setting the Tension (The Critical Step):
1. The tension of the transfer dictates the functional outcome. The goal is to provide maximum extension power without permanently eliminating passive elbow flexion.
2. Adduct the arm and fully extend the elbow. Place the deltoid under maximal physiological tension.
3. Preliminarily suture the graft to the triceps aponeurosis or directly into an olecranon bone tunnel.
4. Test the passive range of motion. You must be able to passively flex the elbow to at least 90 degrees (some authors advocate for full passive flexion, though this risks a lax transfer). If the transfer is too tight, the patient will lose the ability to bring the hand to the mouth.
5. Once optimal tension is confirmed, permanently secure the graft. Place stainless steel surgical markers (clips) at measured distances proximal and distal to the repair site. This allows for radiographic verification of repair integrity postoperatively (Ejeskär technique).
Restoration of Key Pinch and Grasp
For most authors, the ultimate goal of distal upper extremity reconstruction in tetraplegia is to obtain a reliable key grip (lateral pinch). Key pinch posture provides a stronger, broader gripping surface, is cosmetically preferable, and is biomechanically easier to achieve than a "chuck-jaw" (three-jaw chuck) pinch.
Grasping with all fingers is highly desirable but cannot be accomplished without the availability of multiple expendable motor units, which are rarely present in high-level tetraplegia. The surgical objective is not to provide complex, independent digital function, but rather a simple, robust, and reliable mechanism for grasping objects like utensils, catheters, and pens.
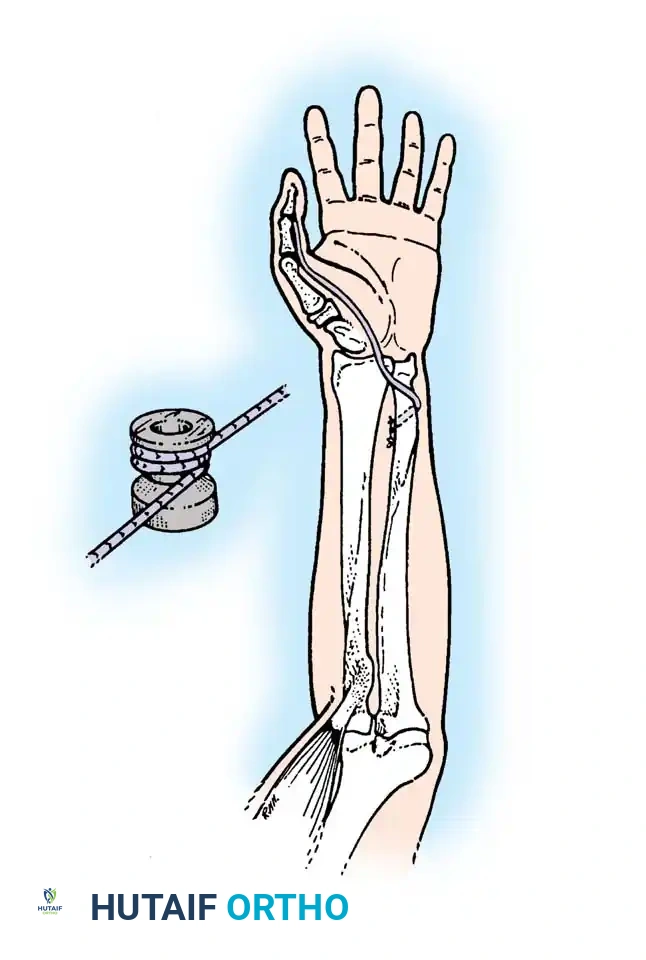
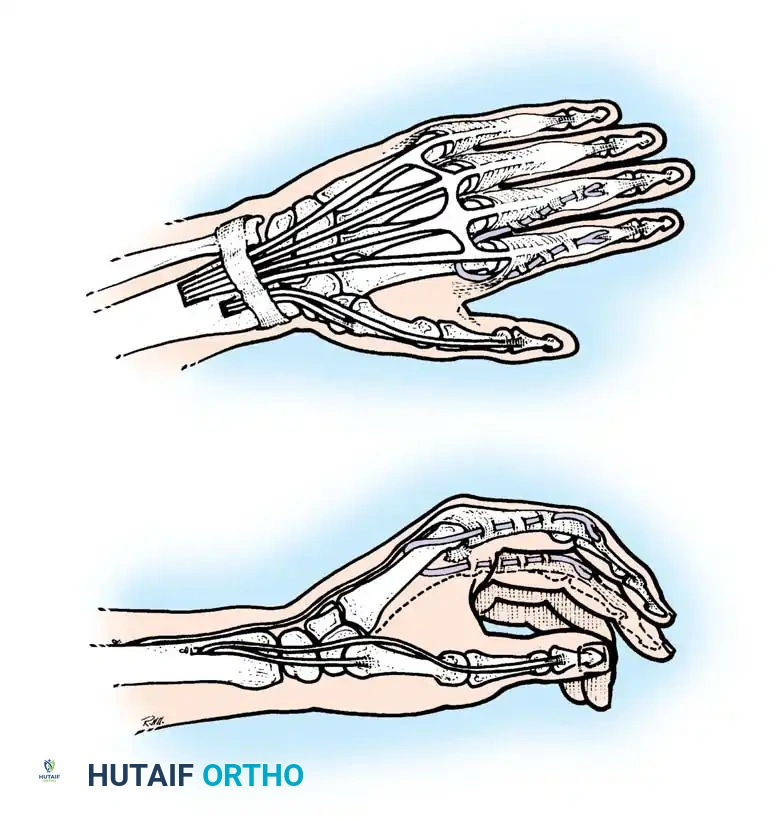
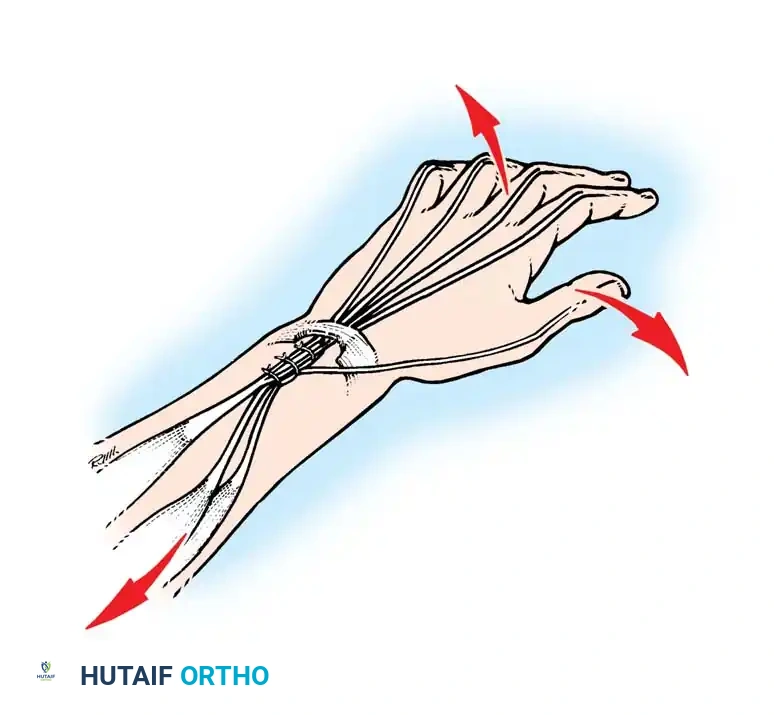
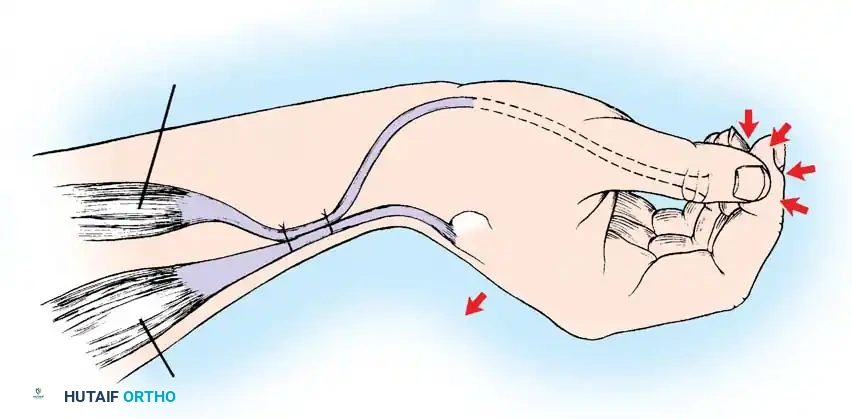
The Tenodesis Effect
In patients lacking active finger flexion, the natural tenodesis effect of the wrist must be harnessed. When the wrist is actively extended (via ECRL/ECRB), the extrinsic finger flexors (FDP, FDS) and the flexor pollicis longus (FPL) passively tighten, causing the fingers and thumb to flex and pinch against each other.
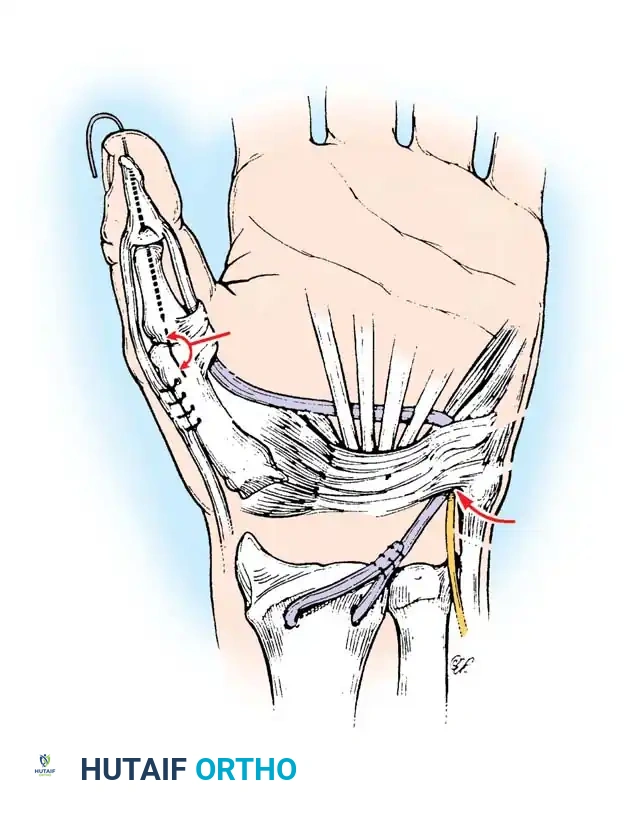
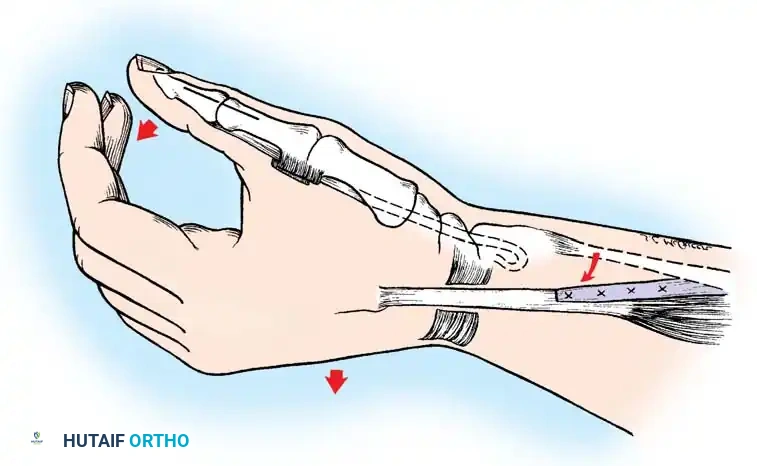
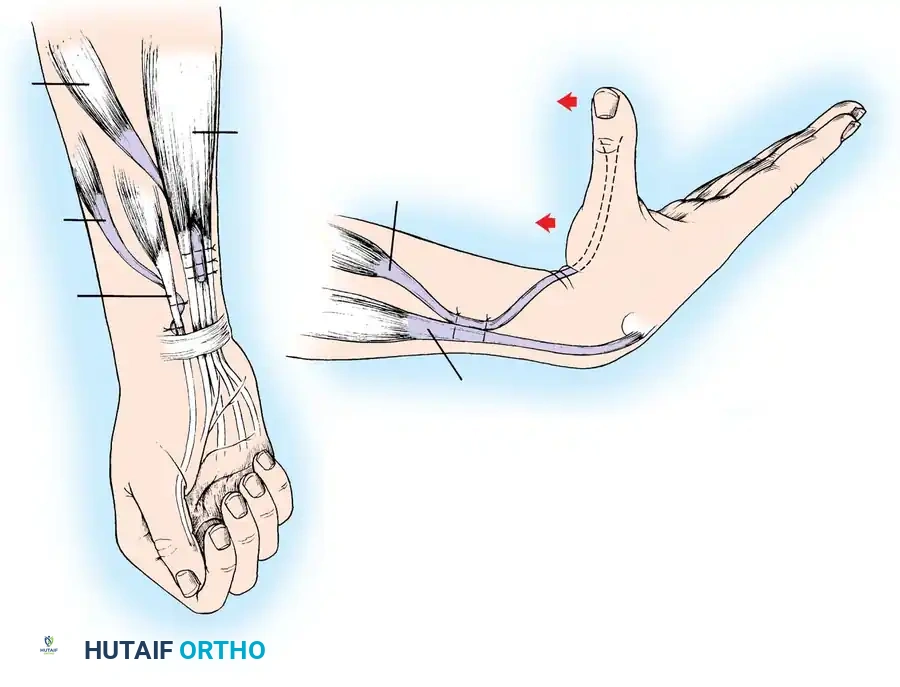
Moberg Key Grip Procedure
For Group 1 or Group 2 tetraplegics, the Moberg key grip procedure is foundational. This involves:
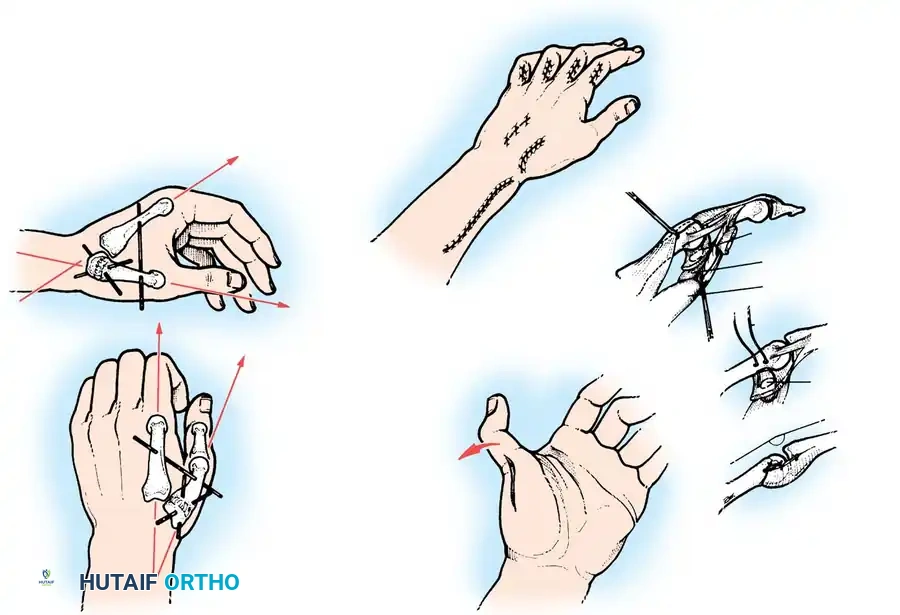
1. FPL Tenodesis: The FPL tendon is divided proximally and anchored to the distal radius. As the patient actively extends the wrist, the anchored FPL passively tightens, driving the thumb into lateral pinch against the index finger.
2. Thumb CMC Arthrodesis or Stabilization: To prevent the thumb from collapsing into retropulsion during pinch, the carpometacarpal (CMC) joint is often arthrodesed, or the metacarpophalangeal (MCP) joint is stabilized via capsulodesis or arthrodesis.
Active Tendon Transfers for Pinch and Grasp
In patients with lower-level tetraplegia (Groups 3-5), active tendon transfers can be employed to provide dynamic pinch and grasp.
- Brachioradialis (BR) to FPL Transfer: The BR is an excellent donor for the FPL. It has immense power and adequate excursion. The BR must be mobilized extensively, proximal to the elbow joint, to maximize its amplitude.
- ECRL to FDP Transfer: If the ECRB is strong enough to maintain wrist extension independently (Group 3), the ECRL can be transferred to the Flexor Digitorum Profundus (FDP) tendons to provide active, powerful finger flexion for a full grasp.
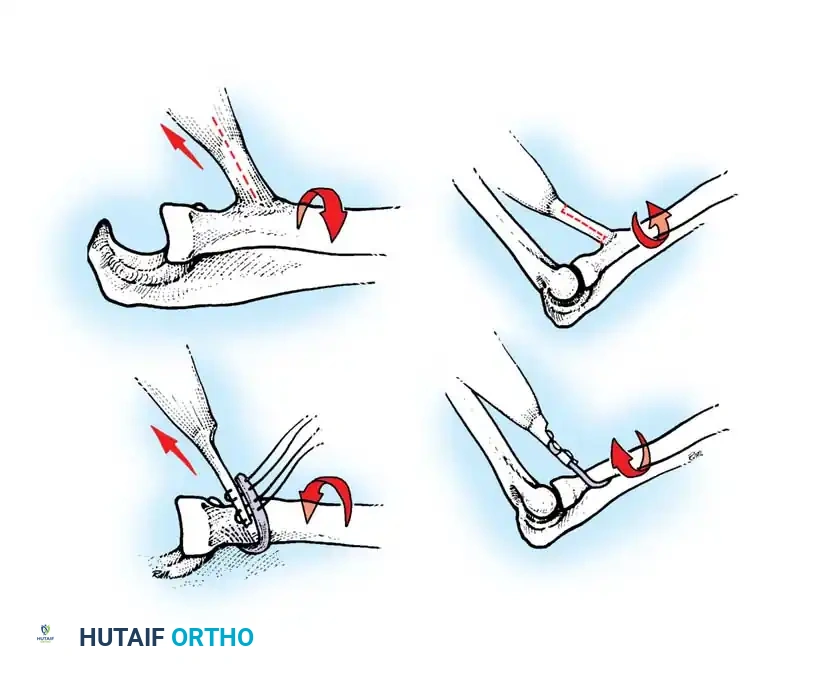
Intrinsic Balancing and the Zancolli Lasso
Tetraplegic hands are inherently "intrinsic-minus," leading to clawing of the fingers (hyperextension of the MCP joints and flexion of the IP joints). This posture defeats the tenodesis effect, as the fingers roll up into the palm rather than sweeping in a wide arc to grasp objects.
To correct this, the Zancolli lasso procedure or similar intrinsic stabilizations are performed. The Flexor Digitorum Superficialis (FDS) tendons are divided distally, looped around the A1 or A2 pulleys, and sutured back onto themselves. This creates a static volar tenodesis that prevents MCP hyperextension, ensuring that proximal pull on the FDP translates into a functional sweeping grasp.
Advanced Modalities: Functional Electrical Stimulation (FES)
High-level tetraplegia (Groups 0 and 1) without available motors for transfer has prompted the development and use of functional electrical stimulation (FES). In these patients, the lower motor neurons to the hand and forearm are often intact, but they lack cortical efferent control.
FES systems utilize implanted or percutaneous electrodes to deliver programmed electrical impulses directly to the intact neuromuscular units. By coordinating combinations of stimuli to different muscles, concerted activities such as grasp, pinch, and release can be synthesized. Freehafer and Keith pioneered implanted neuroprostheses, demonstrating that FES can provide grasp and manipulation capabilities entirely unobtainable by traditional surgical means in high-level tetraplegia.
Postoperative Protocol and Rehabilitation
The success of upper limb reconstruction in tetraplegia is as dependent on meticulous postoperative rehabilitation as it is on surgical execution.
For Deltoid-to-Triceps Transfers:
1. Immobilization: The arm is immobilized in a long-arm cast or rigid orthosis with the elbow at 30 degrees of flexion for exactly 4 weeks. Immobilizing in full extension risks severe joint stiffness, while excessive flexion risks stretching the transfer.
2. Early Mobilization (Weeks 4-8): The cast is removed, and a hinged elbow brace is applied. Active range-of-motion exercises within a protected arc are initiated. Gravity-eliminated exercises are utilized first. Passive stretching of the triceps is strictly prohibited.
3. Strengthening (Week 8+): Progressive resistive exercises are introduced. The patient is trained to integrate the new transfer into daily activities, such as wheelchair propulsion and pressure relief. Maximum hypertrophy and functional integration of the transfer may take up to 12 to 18 months.
For Hand and Wrist Reconstructions:
1. The hand is immobilized in a bulky dressing and volar splint with the wrist in neutral to slight extension, MCP joints flexed to 70 degrees, and IP joints fully extended.
2. At 3 to 4 weeks, active mobilization is commenced. Biofeedback and mirror therapy are highly effective in helping the patient achieve cortical remapping, especially when a muscle (like the BR) is asked to perform a completely novel function (like thumb flexion).
3. Efforts to restore sensation (if applicable) should follow tendon transfers, as cortical interpretation of sensation (localization and stereognosis) is significantly enhanced by active movement of the part.
Through precise patient selection, adherence to biomechanical principles, and rigorous rehabilitation, the orthopedic surgeon can profoundly alter the trajectory of a tetraplegic patient's life, restoring a vital measure of independence and dignity.
You Might Also Like