Metacarpal Lengthening: The Tajima Technique Masterclass
Key Takeaway
Metacarpal lengthening utilizing the Tajima technique is a specialized surgical procedure designed to address congenital hypoplasia or post-traumatic shortening of the hand. By employing a precise chevron osteotomy, interosseous muscle release, and structural iliac crest bone grafting secured with axial Kirschner wire fixation, surgeons can restore functional length and biomechanical balance. This guide details the operative steps, soft tissue management, and postoperative rehabilitation protocols essential for optimal outcomes.
INTRODUCTION TO METACARPAL LENGTHENING
Metacarpal lengthening is a highly specialized reconstructive procedure utilized to restore the anatomical length, biomechanical alignment, and aesthetic appearance of a shortened metacarpal. Shortening of the metacarpals can severely disrupt the complex biomechanical cascade of the hand, leading to a loss of grip strength, altered intrinsic muscle tension, and a cosmetically displeasing "sunken knuckle" appearance.
The Tajima technique remains a cornerstone in operative orthopaedics for addressing metacarpal hypoplasia. Unlike gradual distraction osteogenesis (callotasis), which requires prolonged external fixation and carries a high risk of pin-tract infections, the Tajima method employs an acute lengthening strategy. This is achieved through a meticulously planned chevron osteotomy, extensive soft tissue release, and the interposition of a structural autologous bone graft (typically from the iliac crest), stabilized by axial Kirschner wire (K-wire) fixation.
This comprehensive guide delineates the indications, preoperative planning, step-by-step surgical execution, and postoperative rehabilitation protocols required to master the Tajima technique for metacarpal lengthening.
CLINICAL INDICATIONS AND CONTRAINDICATIONS
Indications
The decision to proceed with metacarpal lengthening must be rooted in both functional deficits and patient-specific goals. Primary indications include:
* Congenital Hypoplasia: Conditions such as brachymetacarpia (most commonly affecting the fourth and fifth metacarpals), symbrachydactyly, or other congenital hand differences where the shortened metacarpal compromises the transverse metacarpal arch.
* Post-Traumatic Shortening: Malunion of metacarpal shaft fractures, bone loss secondary to severe crush injuries, or ballistic trauma resulting in segmental defects.
* Post-Infectious Growth Arrest: Premature closure of the metacarpal physis secondary to pediatric osteomyelitis or septic arthritis.
* Iatrogenic Shortening: Previous surgical resections for benign bone tumors (e.g., enchondroma) resulting in structural collapse.
Contraindications
- Inadequate Soft Tissue Envelope: Severe scarring, radiation dermatitis, or compromised vascularity that cannot accommodate acute skeletal expansion.
- Active Infection: Any ongoing osteomyelitis or soft tissue infection must be eradicated prior to structural grafting.
- Severe Joint Arthrosis: Advanced degenerative changes in the metacarpophalangeal (MCP) or carpometacarpal (CMC) joints may necessitate arthrodesis rather than isolated lengthening.
- Lack of Motor Function: Lengthening a metacarpal in a functionally paralyzed digit will not improve grip mechanics and is generally contraindicated.
Clinical Pearl: Acute lengthening of a metacarpal is generally limited to 1.0 to 1.5 centimeters. Attempting to acutely lengthen beyond this threshold dramatically increases the risk of neurovascular compromise, excessive skin tension, and subsequent digital ischemia. If greater length is required, gradual distraction osteogenesis should be considered.
BIOMECHANICS AND ANATOMIC CONSIDERATIONS
To successfully execute the Tajima technique, the surgeon must possess a profound understanding of hand biomechanics. The metacarpals are not isolated struts; they are dynamically tethered by a complex network of ligaments and muscles.
The Deep Transverse Metacarpal Ligament (DTML)
The DTML connects the volar plates of adjacent MCP joints, effectively tethering the metacarpal heads together to maintain the transverse metacarpal arch. In the setting of a shortened metacarpal, the DTML acts as a primary restrictive force against longitudinal distraction. Surgical release of this ligament is an absolute prerequisite for achieving adequate length.
The Interosseous Muscles
The dorsal and volar interosseous muscles originate from the metacarpal shafts. When a metacarpal is congenitally short or chronically retracted, these muscles adapt to the shortened resting length. During acute lengthening, the interossei act as a deforming force, resisting distraction and potentially causing secondary MCP joint contractures. The Tajima technique addresses this by sharply detaching the interosseous muscles from the metacarpal shaft, allowing for unrestricted skeletal distraction, followed by meticulous reattachment to restore intrinsic function.
PREOPERATIVE PLANNING
Meticulous preoperative planning is the bedrock of a successful outcome.
* Radiographic Evaluation: Standard posteroanterior (PA), lateral, and oblique radiographs of the affected hand are mandatory. Contralateral hand radiographs should be obtained for templating and to determine the exact millimeter discrepancy in length.
* Templating: Calculate the exact length of the bone graft required. The graft must not only fill the defect but also account for the interlocking V-shaped (chevron) osteotomy cuts.
* Donor Site Selection: The anterior iliac crest is the gold standard for harvesting corticocancellous bone. It provides the necessary structural rigidity (cortical strut) to withstand axial loads, combined with osteoinductive cancellous bone to promote rapid incorporation.
SURGICAL TECHNIQUE: THE TAJIMA METHOD
1. Patient Positioning and Anesthesia
- The patient is placed in the supine position with the operative arm extended on a radiolucent hand table.
- General anesthesia or a regional brachial plexus block is administered.
- A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mmHg (or 100 mmHg above systolic blood pressure) following exsanguination with an Esmarch bandage.
- The ipsilateral anterior iliac crest is prepped and draped simultaneously for bone graft harvest.
2. Incision and Exposure
- Make a dorsal longitudinal incision directly over the shortened metacarpal. The incision should extend from the CMC joint to just distal to the MCP joint to ensure adequate exposure.
- Carefully dissect through the subcutaneous tissues, meticulously identifying and retracting the dorsal sensory branches of the radial or ulnar nerves.
- Identify the extensor tendon apparatus. Retract the extensor tendon laterally (usually to the ulnar side) to expose the underlying dorsal periosteum of the metacarpal shaft.
- Incise the periosteum longitudinally and perform a subperiosteal dissection.
Surgical Warning: Maintain a strict subperiosteal plane during exposure. This preserves the delicate periosteal blood supply, which is critical for the incorporation of the avascular bone graft and the healing of the osteotomy sites.
3. Soft Tissue Release and Osteotomy
- Interosseous Muscle Detachment: Sharply detach the interosseous muscle origins from both the radial and ulnar aspects of the metacarpal shaft. This release must be thorough to prevent resistance during distraction.
- DTML Release: Dissect distally to expose the deep transverse metacarpal ligament on both sides of the affected metacarpal head. Incise the ligament to free the metacarpal head from its adjacent tethers.
- The Chevron Osteotomy: Utilize an oscillating microsaw to create two V-shaped (chevron) osteotomies at the junction of the proximal and middle thirds of the metacarpal diaphysis. The apex of the "V" should point distally or proximally depending on the surgeon's preference, though a distally pointing apex often provides superior resistance to dorsal angulation forces.
FIGURE 79-78 A: Tajima technique for metacarpal lengthening. The Chevron osteotomy is made in the shortened metacarpal; the interosseous muscles are detached from the shaft, and the deep transverse metacarpal ligaments are released to allow for unrestricted longitudinal distraction.
4. Distraction and Graft Preparation
- Once the osteotomy is complete and the soft tissues are released, apply manual longitudinal traction to the distal metacarpal segment.
- Assess the adequacy of the release. The gap should open easily without excessive tension on the neurovascular bundles. Measure the exact dimension of the distraction gap using a sterile caliper.
- Bone Graft Harvest: Transition to the iliac crest. Harvest a tricortical or bicortical block of corticocancellous bone matching the measured defect plus an additional 2-3 millimeters to allow for the interlocking chevron cuts.
- Graft Fashioning: Using a rongeur or a fine burr, fashion the ends of the bone graft into reciprocal V-shapes so that it perfectly interlocks with the proximal and distal metacarpal osteotomy sites. This interlocking geometry maximizes surface area for healing and provides inherent rotational stability.
5. Graft Insertion and Fixation
- Insert the fashioned corticocancellous graft into the distraction gap. Ensure that the cortical portion of the graft is positioned dorsally to resist the bending moments exerted by the flexor tendons.
- Axial Fixation: Drive a longitudinal Kirschner wire (typically 0.045 or 0.062 inch) to secure the construct. The K-wire can be introduced retrograde through the metacarpal head (with the MCP joint flexed to 90 degrees to avoid pinning the central articular surface), passed through the distal segment, through the center of the bone graft, and driven securely into the proximal metacarpal base and CMC joint for maximum stability.
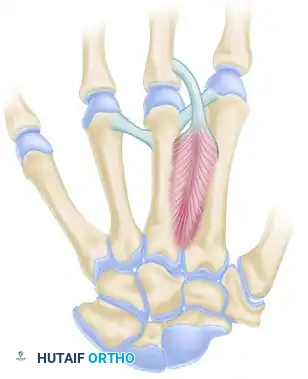
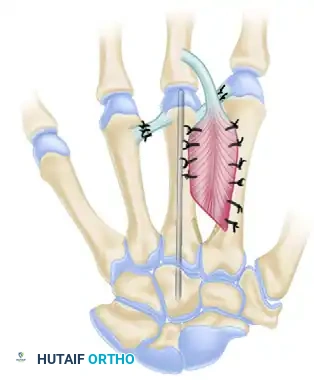
FIGURE 79-78 B: The corticocancellous bone graft is interposed into the defect and secured with a robust axial Kirschner wire. The interosseous muscles are reattached, and the transverse metacarpal ligaments are repaired to restore the transverse arch.
6. Soft Tissue Reconstruction and Closure
- Interosseous Reattachment: The interosseous muscles must be reattached to restore intrinsic digital balance. Depending on the amount of lengthening achieved, the muscles may fall into a new anatomical position. Suture the muscle bellies to the periosteum, or pass non-absorbable sutures through small drill holes made directly into the bone graft or the lengthened metacarpal shaft.
- DTML Repair: If the soft tissue tension allows, repair the deep transverse metacarpal ligaments using a 4-0 non-absorbable suture. This step is crucial for stabilizing the metacarpal head and preventing splaying of the digits. If direct repair is impossible due to the new length, a local fascial slip or tendon graft may be utilized, though often the surrounding scar tissue will stabilize the arch over time.
- Deflate the tourniquet and achieve meticulous hemostasis using bipolar electrocautery.
- Close the extensor retinaculum (if opened) and the skin in a routine, tension-free manner using interrupted sutures.
- Apply a sterile, non-adherent dressing followed by a well-padded volar intrinsic-plus splint (MCP joints flexed to 70-90 degrees, interphalangeal joints fully extended).
POSTOPERATIVE CARE AND REHABILITATION
The success of the Tajima technique relies heavily on a disciplined, phased postoperative rehabilitation protocol. The primary goal is to protect the osteotomy and graft site until radiographic union occurs, while simultaneously preventing stiffness in the adjacent joints.
Phase I: Protection and Immobilization (Weeks 0 to 3)
- The hand is strictly immobilized in the intrinsic-plus splint.
- Elevation of the extremity is paramount to minimize postoperative edema, which can compromise the already stretched skin envelope.
- Active range of motion (ROM) of the uninvolved digits, elbow, and shoulder is encouraged immediately to prevent proximal stiffness and promote venous return.
- Skin sutures are typically removed at 10 to 14 days postoperatively.
Phase II: Early Controlled Motion (Weeks 3 to 6)
- At 3 weeks, the rigid splint is transitioned to a custom-molded thermoplastic splint.
- Initiation of Motion: Gentle, supervised active range of motion of the affected finger is initiated. The K-wire provides sufficient axial stability to allow for tendon gliding, preventing extensor tendon adhesions over the dorsal surgical site.
- Passive motion and forceful gripping are strictly prohibited during this phase, as the bone graft is still undergoing early incorporation and is vulnerable to shear forces.
Phase III: Hardware Removal and Strengthening (Weeks 6 and Beyond)
- At 6 weeks postoperatively, clinical and radiographic evaluations are performed. If radiographs demonstrate bridging callus and early incorporation of the graft at both osteotomy interfaces, the longitudinal Kirschner wire is removed in the clinic.
- Following K-wire removal, the patient is cleared for progressive passive range of motion and dynamic splinting if any joint contractures are present.
- Progressive strengthening exercises (e.g., putty squeezing, grip strengthening) are introduced.
- Full unrestricted activity and return to heavy manual labor or sports are generally permitted between 10 to 12 weeks, contingent upon complete radiographic consolidation of the graft.
COMPLICATIONS AND PITFALLS
While highly effective, metacarpal lengthening is a technically demanding procedure with several potential complications that the orthopaedic surgeon must anticipate and mitigate.
- Neurovascular Compromise: The most devastating acute complication. Over-distraction can stretch the digital arteries, leading to vasospasm and digital ischemia. Prevention: Limit acute lengthening to 1.5 cm. Always assess capillary refill after distraction and before leaving the operating room.
- Nonunion or Delayed Union: Failure of the bone graft to incorporate, often due to inadequate rigid fixation, poor soft tissue coverage, or thermal necrosis during the osteotomy. Prevention: Use sharp saw blades with continuous saline irrigation, ensure a tight interlocking fit of the chevron cuts, and maintain strict subperiosteal dissection.
- Extensor Tendon Adhesions: The dorsal approach places the extensor tendon in direct contact with the healing bone graft, predisposing it to adhesions and subsequent loss of digital flexion. Prevention: Meticulous closure of the periosteal layer over the graft if possible, and strict adherence to the early active motion protocol at 3 weeks.
- Malunion and Rotational Deformity: Inadequate fixation can lead to dorsal apex angulation or rotational malalignment of the digit, causing the fingers to overlap during flexion. Prevention: The chevron osteotomy inherently resists rotation, but precise placement of a robust, centrally located axial K-wire is mandatory. Always check the digital cascade in flexion before final fixation.
- Graft Resorption: The use of purely cancellous bone or allograft increases the risk of structural collapse. Prevention: Always utilize structural corticocancellous autograft (iliac crest) to provide a rigid scaffold capable of withstanding the compressive forces of the hand.
By adhering to the precise biomechanical principles and meticulous surgical steps outlined in the Tajima technique, orthopaedic surgeons can reliably restore metacarpal length, optimize hand function, and achieve excellent long-term clinical outcomes for their patients.
You Might Also Like