Restoration of Intrinsic Finger Function: Surgical Techniques
Key Takeaway
The restoration of intrinsic finger function is critical for correcting claw hand deformities caused by ulnar and median nerve palsy. Surgical reconstruction relies on the principle that long finger extensors can extend the interphalangeal joints if metacarpophalangeal hyperextension is prevented. Techniques include capsulodesis, tenodesis, and active tendon transfers such as the modified Bunnell, Fowler, Riordan, and Brand procedures, which rebalance the hand to restore functional grasp and pinch.
RESTORATION OF INTRINSIC FUNCTION OF THE FINGERS
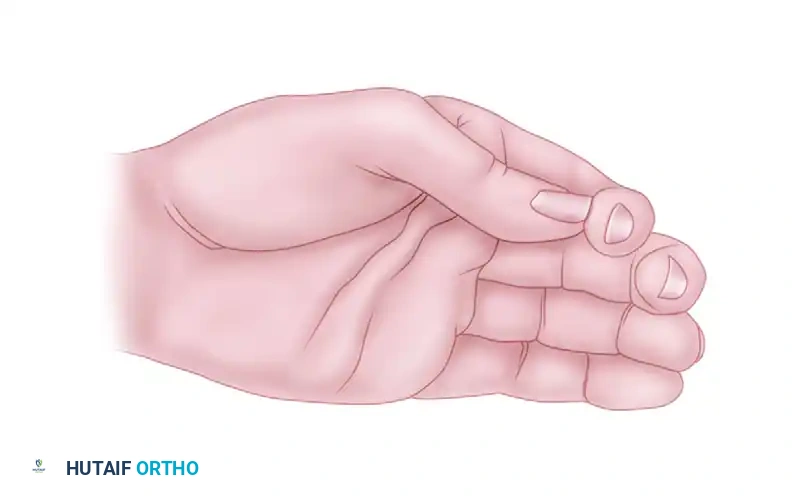
The loss of intrinsic muscle function in the fingers is a profoundly disabling condition, most commonly resulting from paralytic diseases (such as leprosy or poliomyelitis) or low lesions of the median and ulnar nerves. Low lesions of these nerves cause selective paralysis of the intrinsic muscles while sparing the long extrinsic muscles. This muscular imbalance allows the extrinsics to act unopposed, predictably producing the classic "claw hand" (intrinsic-minus) deformity.
Pathomechanics of the Intrinsic-Minus Hand
Loss of intrinsic muscle power primarily causes hyperextension of the metacarpophalangeal (MCP) joints in a mobile hand. However, this resting deformity is not the most disabling aspect of the paralysis. Clinical and biomechanical studies demonstrate that with intrinsic paralysis, overall grip strength is diminished by 50% or more. This profound weakness occurs because the hand lacks the primary power of flexion at the MCP joints.
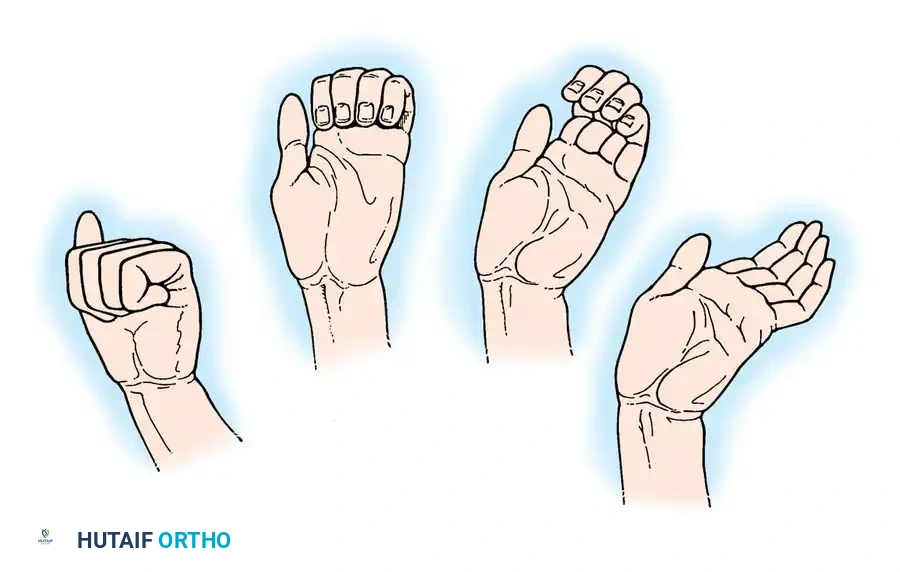
Furthermore, the normal synchronous motion of the fingers is lost. In a healthy hand, finger flexion is a coordinated, sweeping motion. In the intrinsically paralyzed hand, an asynchronous "roll-up" maneuver occurs: the interphalangeal (IP) joints must flex first, driven by the unopposed flexor digitorum profundus (FDP) and superficialis (FDS), followed only later by the MCP joints. Because of this out-of-phase flexion, the hand is unable to grasp large objects effectively; the fingertips roll into the palm before the proximal phalanges can close around the object.
Power of pinch is also severely diminished. Beyond the obvious effects of thenar muscle paralysis, the collateral ligaments of the MCP joints are lax in extension. Without the stabilizing force of the intrinsic musculature, the fingers lose lateral stability. Divergence of the fingers occurs automatically with extension produced by the long extensor tendons, and convergence of the tips during grasping is dictated solely by the alignment of the long flexors. To stabilize the fingers in extension at the MCP joint—especially to provide resistance for the index finger against the pinch pressure of the thumb—functioning intrinsic muscles are absolute prerequisites.
Clinical Pearl: The fundamental principle of intrinsic reconstruction is based on Bouvier’s maneuver: the long finger extensors (extensor digitorum communis) are fully capable of extending the IP joints, provided that hyperextension of the MCP joints is prevented.
Principles of Surgical Reconstruction
Many procedures have been devised to block hyperextension of the MCP joints. However, stabilizing these joints at a selected position while permitting controlled side-to-side deviation requires functioning, dynamic intrinsic muscles. The restoration of grasping power should always be the primary goal if suitable donor muscles are available.
The MCP joints can be stabilized by:
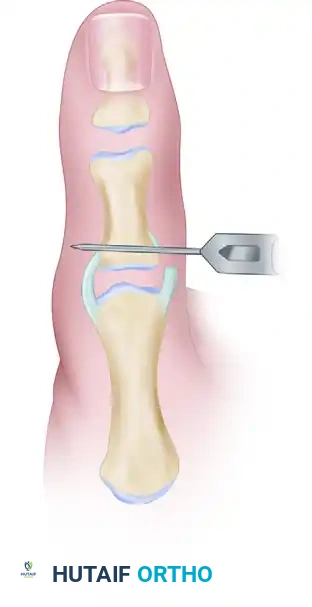
* Capsuloplasty: e.g., Zancolli volar capsulodesis.
* Tenodesis: e.g., Riordan or Fowler techniques.
* Bone Block: e.g., Mikhail technique.
* Arthrodesis: Reserved for severe, rigid deformities or salvage.
* Active Tendon Transfers: Procedures that actively flex the MCP joints and extend the IP joints.
Transfers to replace intrinsic function of the fingers are among the most variable, complicated, and surgically demanding procedures in hand surgery. No single procedure predictably compensates for all deformities that follow intrinsic paralysis; the choice depends on the availability of donor muscles, the degree of passive joint mobility, the presence of habitual wrist flexion, and the surgeon's expertise.
SURGICAL TECHNIQUES FOR INTRINSIC RESTORATION
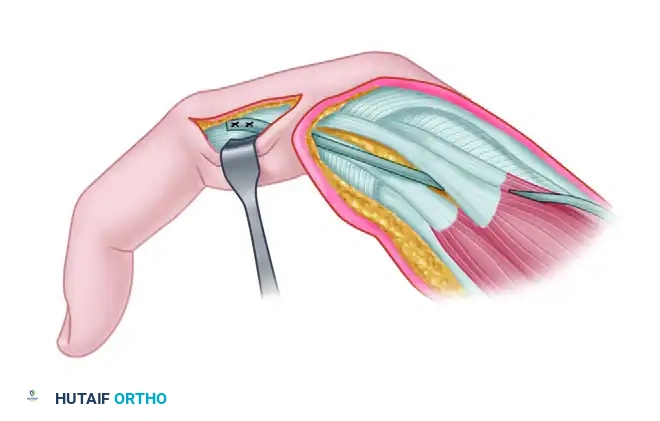
Transfer of a Slip of the Abductor Pollicis Longus Tendon (Neviaser, Wilson, and Gardner)
Neviaser, Wilson, and Gardner described the transfer of an accessory slip of the abductor pollicis longus (APL) tendon to replace the function of the first dorsal interosseous muscle. Anatomical studies reveal that in over 80% of patients, the APL tendon consists of two or more slips. The normal insertions include the base of the first metacarpal, the trapezium, and the thenar fascia. One of these supernumerary slips can be safely harvested for transfer.
Surgical Steps:
1. Incision and Identification: Make a transverse incision near the insertion of the APL. Identify the slips of the abductor tendon at the level of the radial styloid.
> Surgical Warning: Meticulously identify and protect the branches of the superficial radial nerve (SRN) during this exposure. Neuroma formation in this area is highly debilitating.
2. Slip Selection: Apply traction to each slip to determine its exact insertion. Select a slip that does not insert on the first metacarpal base. Divide it at its distal insertion.
3. Distal Exposure: Make a second incision over the radial aspect of the MCP joint of the index finger. Identify the tendon of the first dorsal interosseous muscle.
4. Tunneling: Create a generous subcutaneous tunnel from the radial styloid to the base of the index finger.
5. Grafting: Obtain a free tendon graft (commonly the palmaris longus). Weave the graft into the first dorsal interosseous tendon distal to the MCP joint.
6. Routing and Tensioning: Pass the graft subcutaneously into the area of the radial styloid, ensuring the first dorsal compartment is not disturbed. With the index finger and wrist in a neutral position, weave and suture the graft to the selected APL slip.
> Pitfall: Do not tension the graft too tightly; excessive tension will result in an over-abducted resting posture of the index finger.
Postoperative Care: The wrist and thumb are immobilized in a thumb spica splint for 3 to 4 weeks, after which active, progressive range-of-motion exercises are initiated.
The Modified Bunnell Transfer
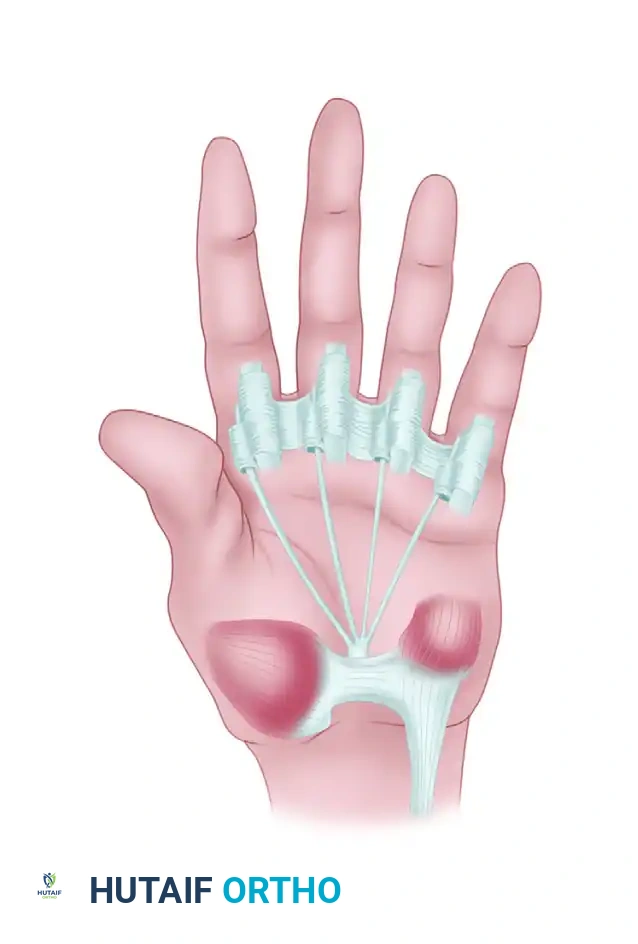
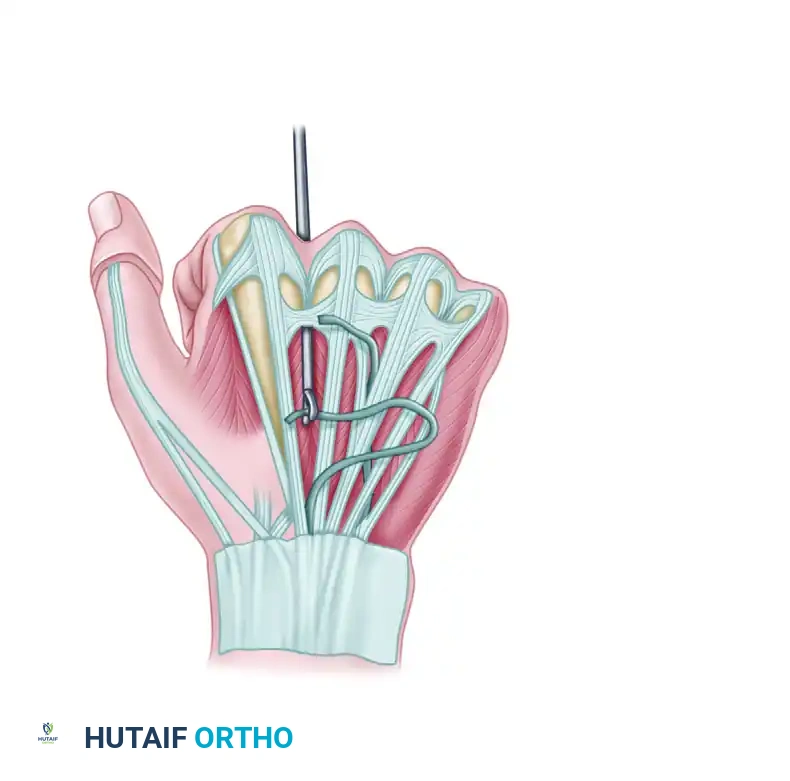
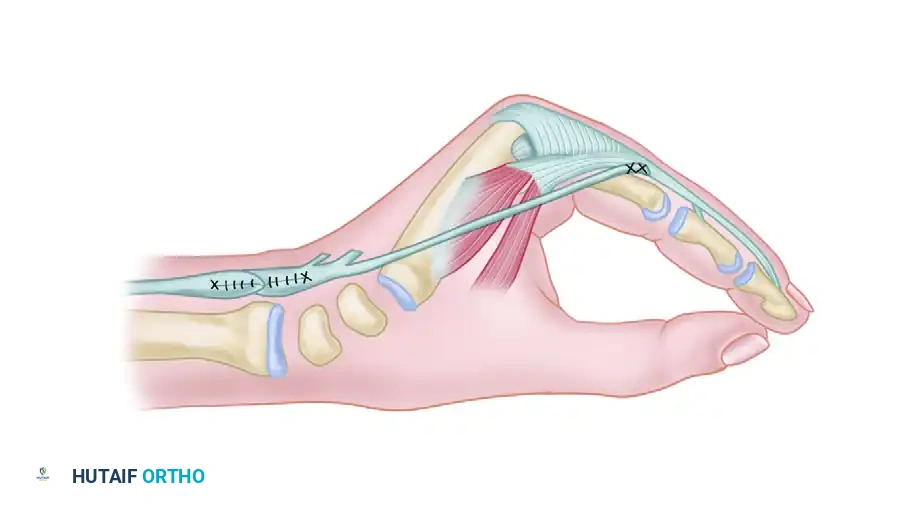
Sterling Bunnell originally devised a technique utilizing the flexor digitorum superficialis (FDS) tendons. In the modified approach, the FDS tendon is detached from the finger, split into slips, and passed through the lumbrical canals to the extensor aponeurosis of each finger. This removes a powerful flexor of the proximal interphalangeal (PIP) joint and converts it into an extensor of that same joint and a flexor of the MCP joint.
Modification of Bunnell transfer to restore intrinsic function of fingers. The FDS is routed through the lumbrical canals.
Complications of the Bunnell Transfer:
Because the FDS is an exceptionally strong muscle, this transfer is often too powerful. Over several months to years, it can pull the PIP joints into rigid extension, producing a severe iatrogenic "intrinsic-plus" deformity (swan-neck deformity). To mitigate this, a modification using only a single FDS tendon (usually from the ring finger) split into four slips for all fingers can be employed. However, setting and maintaining equal tension across all four slips remains technically challenging.
The Fowler Transfer
Fowler addressed intrinsic paralysis by splitting the extensor indicis proprius (EIP) and extensor digiti minimi (EDQ) tendons to form four slips. These slips are attached to the radial side of the extensor aponeuroses of the index and middle fingers, and the ulnar side of the ring and little fingers.
In his later, more biomechanically sound modification, the tendon slips are passed volar to the deep transverse metacarpal ligament (DTML). This volar routing is critical: it changes the vector of pull, allowing the transfer to effectively flex the MCP joint while extending the IP joints.
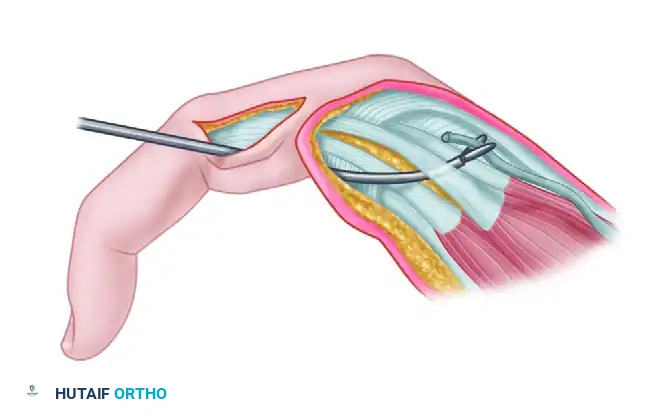
Clamp threading graft through the interosseous space.
Clamp threading graft volar to the transverse metacarpal ligament.
Fowler transfer: Tendon being routed volar to the deep transverse metacarpal ligament.
Addressing Tension Issues in the Fowler Transfer:
To reach their destinations on the extensor aponeuroses, the ends of the tendon slips must be advanced approximately 2.5 cm. This places them under considerable tension, which can precipitate an intrinsic-plus deformity. To avoid excessive tension, the procedure is modified:
1. The detached EIP tendon is split into two slips, passed volar to the DTML, and attached to the radial side of the ring and little fingers.
2. A free tendon graft is attached to the musculotendinous junction of the EIP.
3. The distal end of this graft is split into two slips, passed distally in a similar manner, and attached to the radial side of the middle and index fingers.

Graft tacked to the side of the extensor mechanism.
The Riordan Transfers and Tenodesis
Riordan further refined the Fowler concept. Instead of attaching the free tendon graft to the musculotendinous junction of the EIP, Riordan attached the tendon graft to the freed insertion of the palmaris longus tendon.

Riordan transfer: Palmaris longus and plantaris graft routed to the index and middle fingers, while the EIP is split and rerouted to the ring and little fingers.
Management of the Flexed Wrist Habit:
Patients with intrinsic paralysis often develop a habit of flexing the wrist to create a tenodesing effect on the long extensor tendons, attempting to passively extend the IP joints. If this wrist flexion is habitual and a wrist flexor can be spared, Riordan recommended transferring the flexor carpi radialis (FCR).
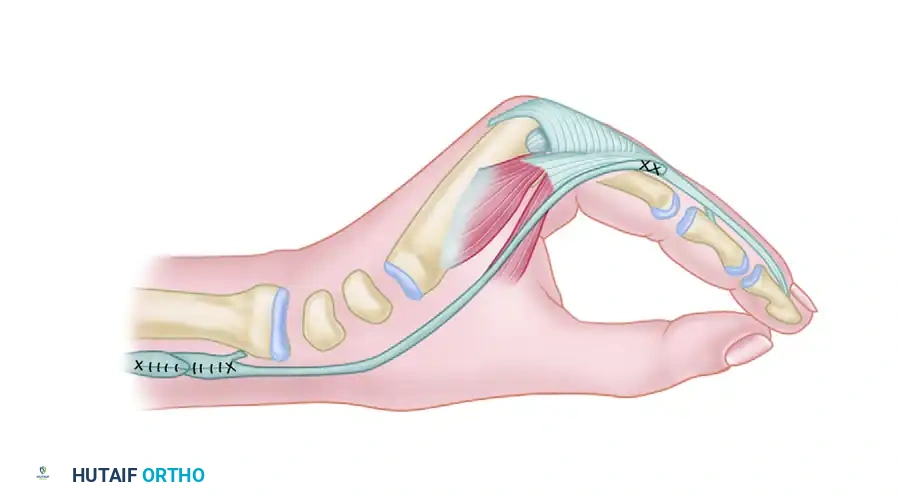
Riordan transfer utilizing the Flexor Carpi Radialis (FCR) transferred to the dorsum of the wrist to restore intrinsic function.
The FCR is freed at its insertion, transferred to the dorsum of the wrist, and prolonged with a four-tailed tendon graft. Each tail is passed volar to the DTML and attached to the radial sides of the extensor aponeuroses. This provides a powerful, active correction of the claw deformity.
Riordan Tenodesis:
If no suitable donor muscles are available for active transfer, a tenodesing procedure is indicated to stabilize the MCP joints. Riordan devised a tenodesis using the extensor carpi radialis brevis (ECRB) and extensor carpi ulnaris (ECU).
* The tendons are cut halfway through at the junction of the middle and distal thirds of the forearm.
* One half of each tendon is stripped distally, leaving the insertion on the metacarpal base intact.
* Each strand is split into two strips (forming four slips total).
* These slips are passed through the interosseous spaces, volar to the DTML, and attached to the radial side of the extensor aponeuroses.
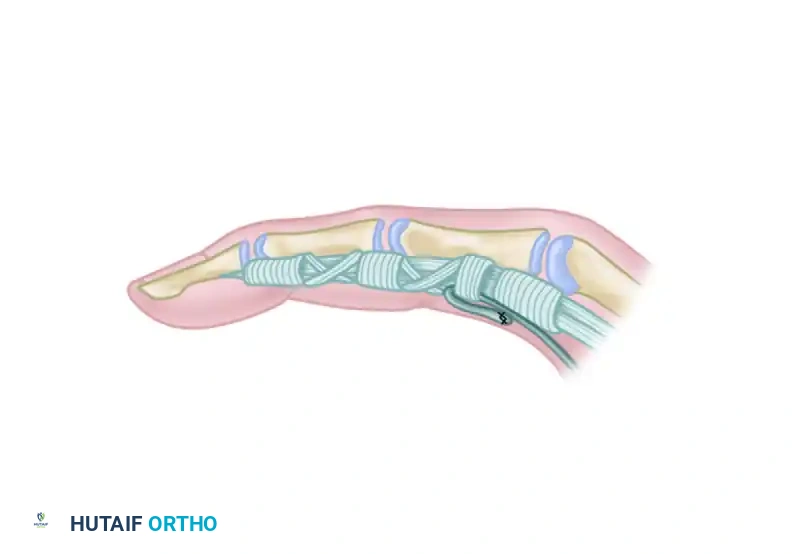
Detail of the tenodesis slip attachment to the lateral band of the extensor mechanism.
The Brand Transfers
Paul Brand contributed significantly to the treatment of the intrinsic-minus hand, particularly in patients with Hansen's disease (leprosy). Brand devised a technique utilizing the ECRB tendon, lengthened by a free graft from the plantaris tendon.
Brand transfer of the ECRB tendon prolonged with a free graft to restore intrinsic function.
Surgical Biomechanics of the Brand Transfer:
The distal end of the plantaris graft is split into four tails. Each tail is passed volar to the DTML. For the middle, ring, and little fingers, the slips are attached to the radial side of the proximal phalanx or extensor aponeurosis.
Surgical Pearl (Index Finger Routing): For the index finger, Brand specifically recommended attaching the slip to the ulnar side of the extensor mechanism. This biomechanical adjustment ensures that during pinch, the index finger is pulled into adduction rather than abduction, providing a much firmer and more stable key pinch against the thumb.

Routing of the four-tailed plantaris tendon graft.
Volar Routing Modification:
In cases where dorsal routing is suboptimal, Brand also described transferring the ECRL or ECRB to the volar side of the forearm. The muscle is extended by a four-tailed graft passed through the carpal tunnel, through the lumbrical canals, and finally to the extensor aponeuroses.
Brand transfer of the ECRL or ECRB to the volar side of the forearm, prolonged with a free graft through the carpal tunnel.

Detailed view of the volar routing and graft attachment.
Warning: This volar transfer crowds the carpal tunnel. If the median nerve is still functioning, this added volume can precipitate acute carpal tunnel syndrome. It is generally reserved for patients with established median nerve palsy where compression is no longer a clinical concern.
POSTOPERATIVE REHABILITATION AND OUTCOMES
The success of intrinsic restoration relies as much on meticulous postoperative therapy as it does on surgical execution.
Immobilization Phase (Weeks 0-4):
Postoperatively, the hand is immobilized in a dorsal blocking splint. The wrist is positioned in neutral to 30 degrees of extension (depending on the specific transfer and tension). The MCP joints are immobilized in 70 to 90 degrees of flexion to remove tension from the newly transferred slips, while the IP joints are left free to extend fully.
Mobilization Phase (Weeks 4-8):
At 3 to 4 weeks, the splint is modified to allow active flexion and extension within safe limits. The patient is taught to activate the transferred muscle. For example, if a wrist extensor (ECRB) was used, the patient is instructed to extend the wrist to initiate MCP flexion and IP extension.
Strengthening Phase (Weeks 8+):
Progressive resistance exercises are introduced. The focus is on restoring synchronous finger flexion, eliminating the "roll-up" phenomenon, and maximizing grip and pinch strength.
Complications and Pitfalls
- Intrinsic-Plus Deformity: The most common long-term complication, particularly with the Bunnell FDS transfer. Excessive tension causes rigid MCP flexion and PIP hyperextension (swan-neck). Treatment may require surgical release or lengthening of the lateral bands.
- Graft Rupture or Attenuation: Usually occurs due to premature mobilization or inadequate suturing technique (a Pulvertaft weave is mandatory for all tendon junctions).
- Failure to Correct the Claw: Often results from failing to route the tendon slips volar to the deep transverse metacarpal ligament. If routed dorsally, the transfer will only exacerbate MCP hyperextension.
- Adhesions: Extensive subcutaneous tunneling and free grafts are prone to scarring. Meticulous hemostasis and early, controlled IP joint motion are critical to prevent tethering.
By adhering to strict biomechanical principles, carefully selecting the appropriate donor tendons, and ensuring precise routing and tensioning, the orthopedic surgeon can successfully restore functional grasp, pinch, and synchronous motion to the intrinsically paralyzed hand.
You Might Also Like