Surgical Management of Psoriatic Arthritis and Reiter Syndrome in the Hand

Key Takeaway
Psoriatic arthritis of the hand presents unique biomechanical and surgical challenges, characterized by asymmetrical peripheral joint involvement, dactylitis, and severe interphalangeal joint destruction. Surgical intervention, primarily proximal interphalangeal joint arthrodesis, is indicated for fixed flexion contractures and instability. This guide details the clinical evaluation, radiographic hallmarks like the pencil-in-cup deformity, and step-by-step operative techniques to optimize functional outcomes while mitigating the heightened infection risks associated with psoriatic skin lesions.
PSORIATIC ARTHRITIS OF THE HAND
Psoriatic arthritis (PsA) is a complex, chronic inflammatory arthropathy associated with psoriasis. In the realm of operative orthopedics and hand surgery, PsA presents a unique set of biomechanical, soft-tissue, and reconstructive challenges that distinguish it significantly from rheumatoid arthritis (RA) and osteoarthritis (OA).
An estimated 25% of patients with psoriatic arthritis exhibit a polyarticular presentation that clinically mimics rheumatoid arthritis. However, 5% to 10% of patients present with exclusive or predominant distal interphalangeal (DIP) joint involvement—a hallmark of the disease. The temporal relationship between cutaneous and articular manifestations is variable; approximately 15% to 20% of patients develop the classic psoriatic skin rash only after the onset of arthritis, complicating early diagnosis.
Almost 95% of patients with psoriatic arthritis demonstrate asymmetrical peripheral joint involvement, a critical differentiating factor from the typically symmetrical presentation of RA.
Clinical Presentation and Pathoanatomy
The clinical presentation of PsA in the hand is driven by a combination of synovitis, enthesitis, and tenosynovitis.
- Dactylitis (The "Sausage Digit"): Fusiform swelling of the entire digit is a classic manifestation. This occurs due to severe, concurrent inflammation of the flexor tendon sheath (tenosynovitis) and the adjacent interphalangeal joints.
- Nail Bed Changes: Uniquely, the nails may separate from the nail bed (onycholysis) and exhibit a white, flaking discoloration near their distal borders. Ridging and hyperkeratosis are also common. Nalebuff observed that fingernail changes—the most common of which is pitting—are present in approximately 15% of patients with joint involvement. The anatomical proximity of the nail matrix to the extensor tendon insertion at the DIP joint explains the frequent coexistence of nail dystrophy and DIP joint arthritis, driven by a contiguous enthesitis.
Clinical Pearl: When evaluating a patient with asymmetrical DIP joint pain and swelling, meticulously examine the nails for pitting or onycholysis. The presence of these nail changes strongly correlates with underlying psoriatic enthesopathy and can guide the diagnosis even in the absence of widespread cutaneous plaques.
Classification of Psoriatic Arthritis
Kapasi, Ruby, and Calney established a highly pragmatic classification system that categorizes patients into three distinct groups based on the temporal onset of arthritis relative to skin lesions. This classification has direct prognostic implications for the severity of joint destruction:
- Type 1: Characterized by the early onset of joint involvement with the late development of skin lesions. In these patients, the arthritic involvement tends to be relatively mild.
- Type 2: Characterized by late joint involvement following early, established skin changes. This cohort typically experiences a much more severe, rapidly progressive, and destructive form of arthritis.
- Type 3: Characterized by the almost simultaneous onset of joint and skin involvement. The severity of arthritic destruction in this group is highly unpredictable.
Radiographic Hallmarks and Biomechanics
The radiographic progression of psoriatic arthritis in the hand is characterized by a combination of aggressive bone resorption and paradoxical bone proliferation.
Key radiographic findings include:
* Acro-osteolysis: Erosion and resorption of the terminal phalangeal tufts.
* Tapering and Cupping: Tapering of the distal ends of the phalanges and metacarpals, combined with the cupping of the proximal ends of the adjacent phalanges. This creates the classic "pencil-in-cup" deformity, which leads to profound multidirectional joint instability.
* Ankylosis: Severe destruction often culminates in the spontaneous bony ankylosis of isolated small joints.
* Joint Predilection: There is a strong predilection for the interphalangeal (DIP and PIP) joints, with a notable sparing of the metacarpophalangeal (MCP) joints.
Differential Diagnosis: Osteoarthritis and Systemic Lupus Erythematosus
Differentiating PsA from other arthropathies is critical for surgical planning.
Osteoarthritis (OA):
Unlike PsA, OA typically presents with Heberden's nodes at the DIP joints and Bouchard's nodes at the PIP joints, driven by cartilage loss and osteophyte formation rather than aggressive central erosions.
Fig. 70-4 Osteoarthritic hands with Heberden (distal interphalangeal) and Bouchard (proximal interphalangeal) nodes on both index fingers and thumbs. Note angular changes at distal joints as a result of loss of joint cartilage and instability.
Systemic Lupus Erythematosus (SLE) and Vasculitis:
SLE can present with severe hand deformities (Jaccoud's arthropathy) characterized by reducible subluxations and dislocations without the erosive bone destruction seen in PsA. Furthermore, SLE may be complicated by vasculitis, leading to digital ischemia and necrosis, a pathology distinct from the inflammatory enthesitis of PsA.

Fig. 70-5 Vasculitis associated with lupus erythematosus resulted in necrosis of fingertips in a 33-year-old woman.
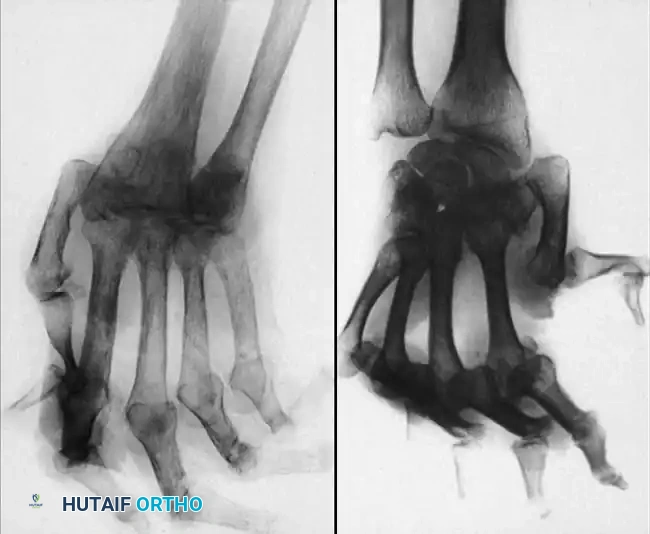
Fig. 70-6 A and B, Typical radiographs of hand and wrist in patients with systemic lupus erythematosus. Note joint dislocations without erosive changes or joint space narrowing. (From Nalebuff EA: Surgery of psoriatic arthritis of the hand, Hand Clin 12:603, 1996.)
SURGICAL MANAGEMENT OF PSORIATIC ARTHRITIS
Contractures of the proximal interphalangeal (PIP) joints are the most common indication for surgical intervention in the psoriatic hand. Due to the severe destruction of the articular surfaces and the attenuation of the collateral ligaments, arthrodesis is overwhelmingly the procedure of choice.
In a landmark report of 25 patients with psoriatic arthritis, Belsky et al. found PIP joint involvement in 22 patients. The natural history of the disease was starkly illustrated: seven patients had spontaneous fusion of all eight PIP joints, and 13 developed fixed flexion contractures exceeding 90 degrees in all PIP joints.
Implant Arthroplasty vs. Arthrodesis
While silicone implant arthroplasty can improve hand function in select patients with RA, its use in PsA is highly controversial. Belsky et al. explicitly warned that the risk of deep periprosthetic infection is significantly higher after implant arthroplasty in PsA patients compared to those with rheumatoid disease. This is attributed to the colonization of psoriatic skin plaques by Staphylococcus aureus and the compromised local soft-tissue envelope. Consequently, PIP and DIP joint arthrodesis remains the gold standard for achieving a stable, painless, and functional digit.
Surgical Warning: Nalebuff strongly recommended scheduling elective surgical procedures for psoriatic arthritis during the summer months. During this season, ultraviolet exposure typically causes psoriatic skin lesions to regress and become smaller, thereby significantly reducing the risk of postoperative surgical site infections. Never incise directly through an active, scaling psoriatic plaque if it can be avoided.
Operative Technique: Proximal Interphalangeal (PIP) Joint Arthrodesis
The goal of PIP arthrodesis is to provide a stable pinch and grasp. The angle of fusion must be tailored to the specific digit to optimize the cascade of the hand: typically 40 degrees of flexion for the index finger, increasing by 5 to 10 degrees for each subsequent ulnar digit (up to 55-60 degrees for the small finger).
1. Patient Positioning and Preparation
- The patient is placed supine with the operative arm extended on a radiolucent hand table.
- Regional anesthesia (brachial plexus block) or general anesthesia is administered.
- A well-padded pneumatic tourniquet is applied to the upper arm and inflated to 250 mm Hg after exsanguination.
- Meticulous skin preparation is paramount. Chlorhexidine-alcohol solutions are preferred, taking care to gently prep over any dormant psoriatic plaques without causing abrasion.
2. Surgical Approach
- A dorsal longitudinal or dorsal lazy-S incision is made over the PIP joint.
- Full-thickness skin flaps are elevated to protect the delicate dorsal vascular network.
- The extensor mechanism is exposed. A longitudinal tenotomy is performed through the central slip, splitting it to expose the underlying joint capsule.
- The collateral ligaments are sharply excised from their proximal attachments to allow for complete joint exposure and mobilization.
3. Joint Preparation
- In cases of severe "pencil-in-cup" deformity, the remaining sclerotic bone must be aggressively debrided to expose healthy, bleeding cancellous bone.
- Using a microsaw or manual rongeurs, the articular surfaces of the proximal and middle phalanges are resected.
- A "cup and cone" reaming technique or flat opposing cuts can be utilized. The cup and cone method provides superior bony apposition and allows for fine-tuning of the flexion angle prior to definitive fixation.
4. Fixation Techniques
Rigid internal fixation is critical due to the poor bone stock often encountered in PsA.
* Tension Band Wiring: Two parallel 0.035-inch Kirschner wires (K-wires) are driven antegrade through the middle phalanx and retrograde into the proximal phalanx at the desired angle. A 24-gauge stainless steel wire is passed through a transverse drill hole in the proximal phalanx and looped in a figure-of-eight fashion over the K-wires to provide dynamic compression.
* Headless Compression Screws: If bone stock permits, a single axial headless compression screw provides excellent rigid fixation and eliminates the issue of prominent hardware beneath the thin dorsal skin.
5. Closure and Postoperative Protocol
- The extensor mechanism is reapproximated using 4-0 absorbable sutures.
- The skin is closed with non-absorbable monofilament sutures.
- A bulky, non-adherent soft dressing is applied, followed by a volar plaster splint immobilizing the digit in the fused position.
- Postoperative Care: The splint is maintained for 4 to 6 weeks. Pin tract care (if K-wires are left exposed) must be meticulous due to the heightened infection risk. Radiographic union is typically observed between 6 and 8 weeks, at which point hardware may be removed if symptomatic, and progressive strengthening is initiated.
REITER SYNDROME (REACTIVE ARTHRITIS)
Reiter syndrome, now more commonly referred to within the spectrum of reactive arthritis, is a seronegative spondyloarthropathy classically described by the clinical triad of:
1. Conjunctivitis
2. Urethritis
3. Synovitis
Clinical Presentation and Differentiation
The synovitis in Reiter syndrome is typically acute, asymmetrical, and oligoarticular, usually involving four or fewer joints. While it predominantly affects the large joints of the lower extremity (knees, ankles), upper extremity involvement can occur.
Patients frequently present with enthesitis, manifesting as severe heel pain (Achilles tendinitis or plantar fasciitis), back pain (sacroiliitis), and nail deformities. These nail changes and the presence of dactylitis can sometimes make it clinically difficult to distinguish Reiter syndrome from psoriatic arthritis in the acute setting.
However, several key factors differentiate the two:
* Demographics: Reiter syndrome is typically found in young men (often following a genitourinary or gastrointestinal infection), whereas PsA has a more equal gender distribution and a wider age of onset.
* Disease Course: The natural history of Reiter syndrome is generally favorable. Approximately 90% of patients experience a complete remission of symptoms after several weeks to months of conservative management with nonsteroidal anti-inflammatory drugs (NSAIDs) and targeted physical therapy.
* Chronicity: In only about 10% of cases does the disease become chronic and destructive.
Surgical Indications
Because of the high rate of spontaneous remission and the primarily inflammatory (rather than structurally destructive) nature of the early disease, surgery is rarely indicated in Reiter syndrome. Operative intervention is reserved strictly for the small minority of chronic patients who develop fixed, debilitating contractures or severe secondary osteoarthritis after years of persistent inflammation, at which point the surgical principles mirror those applied to psoriatic arthritis.
You Might Also Like


