Operative Management of Gout and Scleroderma in the Hand

Key Takeaway
Gout and scleroderma present complex reconstructive challenges in hand surgery. While acute gout mimics infection, chronic tophaceous gout causes severe tendon and joint destruction requiring meticulous debridement. Scleroderma leads to profound contractures and ischemia, necessitating joint arthrodesis, resection arthroplasty, and digital sympathectomy. This guide details the evidence-based surgical indications, operative techniques, and postoperative protocols for managing these debilitating systemic arthropathies.
INTRODUCTION TO SYSTEMIC ARTHROPATHIES OF THE HAND
The surgical management of systemic arthropathies and connective tissue diseases—specifically gout, calcium pyrophosphate deposition disease (pseudogout), and scleroderma—requires a profound understanding of both the underlying medical pathophysiology and the complex biomechanical alterations they inflict upon the hand and wrist. Unlike primary osteoarthritis, these conditions are characterized by aggressive soft tissue infiltration, profound inflammatory cascades, and severe microvascular compromise. The orthopedic surgeon must navigate a delicate balance between aggressive debridement or reconstruction and the preservation of tenuous vascular supplies.
GOUTY ARTHROPATHY
Gout is a crystal-induced arthropathy caused by the deposition of monosodium urate (MSU) crystals within joints, periarticular soft tissues, and tendon sheaths. While typically presenting as an acute, intensely painful, erythematous monoarthropathy in men, its chronic tophaceous form frequently involves the hand and wrist, particularly in postmenopausal women.
Clinical Presentation and Diagnostic Pitfalls
The acute gouty attack is characterized by sudden, severe pain, swelling, and profound erythema. The joint is exquisitely tender and hot, frequently mimicking a severe cellulitis or septic arthritis.
🚨 SURGICAL WARNING: The "Unsuspecting Surgeon" Pitfall
Acute gouty arthritis of the hand or wrist can perfectly mimic a closed space infection, abscess, or septic tenosynovitis. An unsuspecting surgeon may hastily perform an incision and drainage (I&D). Inappropriate surgical intervention during an acute gout flare can lead to delayed wound healing, secondary bacterial infection, and chronic sinus tract formation. Always rule out crystal arthropathy via aspiration before proceeding with I&D in atypical presentations.
In chronic tophaceous gout, massive deposits of MSU crystals accumulate around joints and within tendon sheaths. These tophi can cause:
* Nerve Compression: Median nerve compression (carpal tunnel syndrome) is a frequent complication of gouty flexor tenosynovitis.
* Tendon Rupture: Intratendinous crystal deposition mechanically weakens the tendon architecture, leading to spontaneous rupture, most commonly of the extensor pollicis longus (EPL) or digital extensors.
* Skin Ulceration: Expanding tophi exert immense pressure on the overlying dermis, leading to ischemia, ulceration, and chalky white exudate.
* Bony Destruction: Extreme osteolysis and joint destruction can occur, sometimes necessitating digital amputation.
The diagnosis of gout is definitively established only by joint or tendon sheath aspiration. Polarized light microscopy will reveal negatively birefringent, needle-shaped monosodium urate crystals.
CLINICAL PEARL: Serum Uric Acid Reliability
The presence of hyperuricemia alone does not establish the diagnosis of gout, as many hyperuricemic patients never experience an attack. Conversely, during an acute gout flare, serum uric acid levels may be entirely normal due to the acute phase response increasing renal urate excretion. Rely on synovial fluid analysis, not serum labs, for definitive diagnosis.
Surgical Indications and Operative Techniques
Surgery for gout is rarely indicated for acute flares. Medical management (NSAIDs, colchicine, corticosteroids, and subsequent urate-lowering therapy) remains the gold standard. However, surgical intervention becomes necessary under the following conditions:
1. Compression of critical neurovascular structures (e.g., acute or refractory carpal tunnel syndrome).
2. Impending or actual tendon rupture.
3. Severe mechanical block to joint motion caused by massive tophi.
4. Skin necrosis, ulceration, or secondary infection.
5. Intractable pain in a destroyed joint.
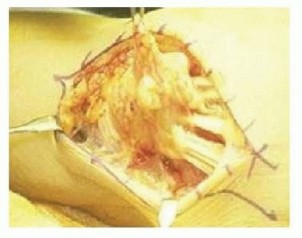
Tophus Excision and Tenosynovectomy
- Positioning and Anesthesia: The patient is positioned supine with the arm on a hand table. Regional anesthesia (axillary or supraclavicular block) is preferred. A well-padded pneumatic tourniquet is applied.
- Approach: Incisions should be planned to allow extensile exposure while preserving vascularity to the skin flaps. Tophi often adhere intimately to the dermis; meticulous dissection is required to prevent full-thickness skin necrosis.
- Debridement: The chalky, toothpaste-like MSU deposits are curetted and irrigated. Complete excision is often impossible without sacrificing vital structures. The goal is debulking to relieve pressure, not oncologic-level clearance.
- Tendon Management: If the flexor or extensor tendons are heavily infiltrated, a meticulous tenosynovectomy is performed. If a tendon is ruptured (e.g., EPL), primary repair is rarely possible due to substance loss and tissue friability. Tendon transfers (e.g., Extensor Indicis Proprius to EPL) are the preferred reconstructive option.
Joint Reconstruction
In cases of extreme bony disruption, arthrodesis or, in severe cases with unmanageable soft tissue compromise, amputation may be necessary to restore a functional, pain-free hand.
DIFFERENTIAL DIAGNOSIS: PSORIATIC ARTHRITIS AND PSEUDOGOUT
When evaluating destructive arthropathies of the hand, the surgeon must differentiate gout from other inflammatory conditions, notably psoriatic arthritis and pseudogout.
Psoriatic Arthritis
Psoriatic arthritis frequently involves the distal interphalangeal (DIP) joints and is characterized by "pencil-in-cup" radiographic deformities, dactylitis (sausage digits), and characteristic dermatologic findings.

Recognizing the cutaneous manifestations—such as erythematous plaques on the extensor surfaces and severe nail pitting or onycholysis—is critical for differentiating this autoimmune condition from crystal arthropathies.
Pseudogout (Calcium Pyrophosphate Deposition Disease)
Pseudogout, caused by calcium pyrophosphate dihydrate (CPPD) crystal deposition, is more common in the knee but frequently involves the wrist and hand.
* Clinical Presentation: It mimics acute gout or septic arthritis with intermittent, acute inflammatory attacks. It can cause severe flexor tenosynovitis leading to acute median nerve compression.
* Radiographic Findings: Routine radiographs often reveal chondrocalcinosis—opaque calcifications within the articular cartilage or the fibrocartilaginous triangular fibrocartilage complex (TFCC) of the distal radioulnar joint.
* Diagnosis and Treatment: Aspiration reveals weakly positively birefringent, rhomboid-shaped crystals. Treatment is primarily medical, though surgical decompression is required if acute carpal tunnel syndrome develops.
SCLERODERMA (PROGRESSIVE SYSTEMIC SCLEROSIS)
Scleroderma is a complex autoimmune connective tissue disease characterized by microvascular endothelial dysfunction, immune dysregulation, and excessive collagen deposition in the skin and internal organs.
Classifications
- Diffuse Scleroderma (Progressive Systemic Sclerosis): A severe form affecting the proximal extremities, trunk, and internal organs (gastrointestinal tract, heart, lungs, kidneys).
- Limited Cutaneous Scleroderma (CREST Syndrome): An acronym for Calcinosis, Raynaud phenomenon, Esophageal dysmotility, Sclerodactyly, and Telangiectasia.
Hand surgeons are most frequently consulted for patients with CREST syndrome or limited scleroderma due to debilitating digital contractures, fingertip ulcerations, and severe Raynaud phenomenon. The age of onset is typically over 40 years.
Pathomechanics and Clinical Findings
Unlike rheumatoid arthritis, synovial thickening in scleroderma is minimal. The primary pathology lies in the fibrotic transformation of the skin, subcutaneous tissues, and tendon sheaths.
* Leathery Crepitus: Involvement of the tendon sheaths causes a palpable friction rub or a distinct "leathery crepitus" during active range of motion. This must be distinguished from the coarse, gritty crepitus typical of osteoarthritis.
* Tendon Rupture: Extensor tendons frequently attenuate and rupture at the interphalangeal joints due to chronic friction and ischemia. The overlying atrophic skin may break down, exposing the joint.
* Sclerodactyly: The skin becomes taut, shiny, and bound down, leading to profound, rigid flexion contractures of the digits.
Surgical Management of Scleroderma Contractures
Because the severe contracture of all soft tissue structures limits the potential for functional movement, surgical intervention must be carefully planned, prioritizing stable, functional positions over the restoration of full mobility.
Distal Interphalangeal (DIP) Joint
Changes at the DIP joint include severe skin ulceration, fixed flexion contractures, dry gangrene, and secondary osteomyelitis.
* Surgical Options: Amputation or arthrodesis. Due to the severe vascular compromise, healing of an arthrodesis can be unpredictable. Terminal amputation is often the most reliable method to eliminate pain and infection.
Proximal Interphalangeal (PIP) Joint
Scleroderma invariably leads to rigid PIP joint flexion contractures. Soft tissue releases are universally unsuccessful due to the diffuse fibrotic nature of the disease.
* Surgical Option: Arthrodesis is the procedure of choice. The joint is fused in a functional position (typically 30 to 40 degrees of flexion, increasing from the index to the small finger). Tension-band wiring or buried K-wires are preferred over bulky plates, which the atrophic skin cannot accommodate.
Metacarpophalangeal (MCP) Joint
The MCP joint may present with either a severe flexion deformity or a paradoxical hyperextension deformity. Resection arthroplasty has proven to be a highly effective method for preserving motion and correcting alignment at this joint, as championed by Nalebuff, Melone, McLoughlin, and Beldner.
- Flexion Deformity Approach: If the primary deformity is MCP flexion, the joint is approached through a standard dorsal longitudinal incision. The metacarpal head is resected to decompress the joint and allow extension.
- Hyperextension Deformity Approach: If the MCP joint is hyperextended (often accompanied by severe PIP flexion), Nalebuff recommends a palmar approach.
- A transverse or zigzag palmar incision is made.
- The flexor tendons are retracted.
- The metacarpal head is resected from the volar aspect.
- This is typically combined with a concurrent dorsal fusion of the PIP joint to correct the complex multi-joint collapse pattern.
Thumb Web Space Contracture
Adduction contracture of the first web space is a profoundly disabling complication, eliminating the patient's ability to grasp large objects.
* Surgical Technique: Release of the adductor pollicis aponeurosis is performed. If the contracture is severe and involves the carpometacarpal joint, Nalebuff advocates for concomitant trapezial excision to thoroughly decompress the first ray.
* Adjuncts: Thumb MCP and IP joint fusions may be added to provide a stable post for pinch. Full-thickness skin grafting or local Z-plasties of the web space are frequently required to close the soft tissue defect.
Management of Ischemia and Calcinosis
Fingertip Ulcerations and Raynaud Phenomenon
Vascular impairment in scleroderma leads to exquisitely painful fingertip ulcerations.
* Conservative Management: The best initial approach is extremely conservative. Allowing ischemic tips to auto-amputate spontaneously is often preferred, as this maximizes the retention of digital length and avoids surgical incisions in profoundly ischemic tissue that will fail to heal.
* Digital Sympathectomy: For refractory ulcers and severe pain, surgical sympathectomy is indicated. As described by Flatt, Wilgis, and Jones, this involves microsurgical stripping of the adventitia (which contains the sympathetic nerve fibers) from the common and proper digital arteries.
* Pharmacologic Adjuncts: Intra-arterial injection of vasodilating drugs (e.g., papaverine, botulinum toxin A, or calcium channel blockers) during surgery helps dilate the spastic vessels. While ischemic changes may eventually recur, the short-term vasodilation is highly beneficial for achieving wound healing and providing immediate pain relief.
> SURGICAL WARNING: Smoking Cessation
Absolute cessation of smoking is a non-negotiable prerequisite for any vascular or reconstructive surgery in the scleroderma patient. Nicotine-induced vasoconstriction will universally doom local flaps, skin grafts, and sympathectomy outcomes.
Calcinosis Cutis
Subcutaneous calcium deposits (calcinosis) frequently erupt through the eroded pulps of the fingers, causing pain and secondary infection.
* Surgical Technique: These deposits can be excised through a mid-lateral incision to avoid the tactile volar pulp. Alternatively, they may be carefully curetted. The surgeon must warn the patient that due to the underlying microvascular disease, wound healing will be significantly delayed, and meticulous postoperative wound care is mandatory.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative management of systemic arthropathies requires a multidisciplinary approach involving the orthopedic surgeon, rheumatologist, and specialized hand therapist.
- Immobilization: Following arthrodesis or resection arthroplasty, rigid immobilization in a bulky, non-compressive dressing is maintained for 10-14 days to allow for initial soft tissue healing.
- Wound Care: In scleroderma patients, sutures should be left in place longer than usual (often 3-4 weeks) due to delayed collagen synthesis and poor vascularity.
- Therapy: For gout patients undergoing tenosynovectomy or tendon transfer, early protected active range of motion is initiated to prevent peritendinous adhesions. For scleroderma patients, therapy focuses on maintaining the functional gains achieved in the operating room, utilizing custom orthoses to prevent the recurrence of contractures.
- Medical Optimization: Postoperative flares of gout are common due to surgical stress. Prophylactic colchicine or NSAIDs should be administered perioperatively. Scleroderma patients must be maintained on systemic vasodilators and strictly avoid cold exposure.
You Might Also Like