Surgical Management of Biceps Brachii Tendon Displacement: A Comprehensive Operative Guide
Key Takeaway
Biceps brachii tendon displacement frequently presents alongside rotator cuff pathology. Surgical management depends on the integrity of the subscapularis and the transverse humeral ligament. While isolated transverse humeral ligament repair is historically described, modern evidence strongly favors biceps tenodesis. This guide details the anterosuperior and deltopectoral approaches, arthroscopic-assisted subpectoral tenodesis, and postoperative rehabilitation protocols to optimize functional outcomes in patients with long head of the biceps tendon instability.
Introduction to Biceps Brachii Tendon Displacement
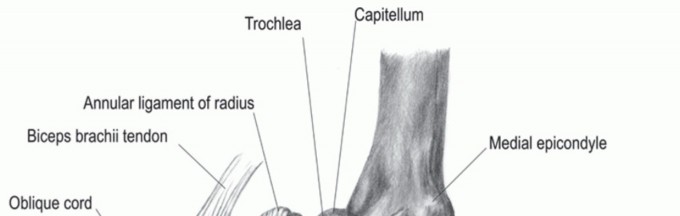
Displacement, subluxation, or dislocation of the long head of the biceps (LHB) tendon is a complex pathological entity that rarely occurs in isolation. The stability of the LHB within the bicipital groove is maintained by a complex capsuloligamentous sling—often referred to as the "biceps pulley"—composed of the superior glenohumeral ligament (SGHL), the coracohumeral ligament (CHL), and the superior fibers of the subscapularis tendon. The transverse humeral ligament (THL) acts as a secondary restraint over the intertubercular groove.
When the biceps pulley is disrupted, the LHB tendon typically subluxates or dislocates medially over the lesser tuberosity. This displacement is intimately associated with subscapularis tendon tears and broader rotator cuff pathology. The surgical management of LHB displacement requires a meticulous understanding of shoulder biomechanics, precise surgical approaches, and evidence-based decision-making regarding tendon repair versus tenodesis.
Clinical Pearl: True isolated displacement of the biceps tendon without concomitant rotator cuff or pulley pathology is exceedingly rare. Always maintain a high index of suspicion for an occult subscapularis tear when medial biceps subluxation is identified on preoperative magnetic resonance imaging (MRI) or during diagnostic arthroscopy.
Biomechanics and Pathoanatomy
The long head of the biceps tendon originates from the supraglenoid tubercle and the superior labrum, traversing the glenohumeral joint before exiting through the bicipital groove. It functions as a dynamic depressor of the humeral head and a weak flexor of the shoulder and elbow.
Displacement of the LHB tendon alters the biomechanical vectors of the shoulder. A medially dislocated biceps tendon acts as a bowstring across the anterior joint, leading to persistent anterior shoulder pain, mechanical clicking, and progressive tearing of the subscapularis tendon due to chronic friction.
Historically, surgical treatment involved relocating the tendon and repairing the transverse humeral ligament. However, modern orthopedic consensus recognizes that the THL is merely a continuation of the subscapularis and supraspinatus fascia. Primary repair of the THL without addressing the underlying pulley lesion or performing a tenodesis yields unacceptably high failure rates. Consequently, biceps tenodesis has become the gold standard for managing LHB displacement.
Surgical Indications and Decision Making
Surgical intervention is indicated for patients with symptomatic biceps tendon displacement who have failed conservative management (e.g., physical therapy, nonsteroidal anti-inflammatory drugs, corticosteroid injections) or those with concomitant rotator cuff tears requiring repair.
Key Surgical Options:
* Transverse Humeral Ligament Repair: Historically described for rare, isolated THL ruptures with an intact pulley. Currently, this is almost universally abandoned in favor of tenodesis due to high recurrence rates.
* Biceps Tenotomy: An acceptable option for low-demand, elderly patients. It provides excellent pain relief but may result in a cosmetic "Popeye" deformity and subjective cramping.
* Biceps Tenodesis: The procedure of choice for active patients, laborers, and athletes. It restores the resting length of the muscle, prevents cosmetic deformity, and maintains elbow flexion and supination strength.
Surgical Technique 1: Isolated Biceps Displacement (Deltopectoral Approach)
In the rare instance where no pathological condition exists in the rotator cuff, or when addressing the biceps pathology in isolation via an open technique, an anterior approach through the deltopectoral interval is utilized.
Positioning and Preparation
- Position the patient in a modified beach-chair position with the head secured and the operative arm draped free.
- Ensure the arm can be freely manipulated into flexion, extension, internal, and external rotation.
Approach and Dissection
- Incision: Make a standard anterior incision following the deltopectoral groove, beginning just distal to the coracoid process and extending distally toward the deltoid insertion.
- Interval Development: Identify the cephalic vein. Retract the vein laterally with the deltoid to protect it, or medially with the pectoralis major depending on surgeon preference and venous anatomy.
- Deep Dissection: Retract the conjoined tendon medially. Identify the long head of the biceps tendon as it exits the joint.
- Ligamentous Release: Make an incision through the transverse humeral ligament, extending down through the proximal third of the pectoralis major tendon to fully expose the bicipital groove.
Management of the Tendon
- Historical Repair: Rarely, if the tendon is pristine and the pulley intact, the biceps tendon can be placed back into the groove, and the transverse humeral ligament can be repaired using heavy, non-absorbable interrupted sutures.
- Tenodesis (Preferred): More commonly, the intra-articular portion of the tendon is excised, and a subpectoral or suprapectoral tenodesis is performed using an interference screw or cortical button.
Surgical Warning: When dissecting distally along the pectoralis major tendon, remain vigilant of the ascending branch of the anterior circumflex humeral artery. Inadvertent injury can cause significant, difficult-to-control hemorrhage.
Surgical Technique 2: Biceps Displacement with Rotator Cuff Tear (Anterosuperior Approach)
If a pathological process of the rotator cuff is present alongside the subluxing biceps tendon, an anterosuperior approach is highly effective. This approach allows for simultaneous management of the biceps tendon, acromioplasty, and rotator cuff repair.
Positioning and Incision
- Position the patient in the beach-chair position.
- Incision: Begin the incision just lateral to the acromioclavicular (AC) joint and extend it distally in line with the deltoid fibers for approximately 4 to 5 cm.
Deltoid Splitting and Protection
- Subcutaneous Dissection: Perform wide subcutaneous dissection to expose the deltoid fascia and its insertion.
- Deltoid Split: Split the deltoid muscle longitudinally, beginning just lateral to the AC joint and continuing exactly 5 cm distally in the deltoid raphe.
Pitfall: Do not extend the deltoid split beyond 5 cm from the lateral edge of the acromion. Extending the split further distally places the axillary nerve at imminent risk of transection, which would result in catastrophic loss of deltoid function. Place a stay suture at the distal apex of the split to prevent inadvertent propagation.
- Vascular Preservation: During the proximal dissection, meticulously identify and preserve the acromial branch of the thoracoacromial artery. Do not excise this vessel, as it provides critical vascularity to the anterior deltoid.
Acromioplasty and Exposure
- Carefully dissect the deltoid from the anterior acromion using electrocautery.
- Perform an anterior acromioplasty to decompress the subacromial space.
- Excise the coracoacromial ligament to further enhance exposure and prevent secondary impingement.
Tenodesis and Cuff Repair
- Tendon Identification: Flex the shoulder to relax the anterior structures. Identify the long head of the biceps tendon.
- Tenodesis: Tenodese the LHB to the proximal humerus. This can be achieved using an interference screw (which provides superior initial biomechanical pull-out strength) or double-loaded suture anchors placed in the bicipital groove.
- Intra-articular Excision: Excise the redundant intra-articular portion of the LHB tendon to eliminate the source of pain.
- Rotator Cuff Repair: Proceed with the repair of the rotator cuff (supraspinatus and/or subscapularis) using standard suture anchor techniques.
- Closure: Close the deltoid meticulously with non-absorbable sutures, followed by standard layered closure of the subcutaneous tissue and skin.
Surgical Technique 3: Arthroscopic Release and Subpectoral Tenodesis
Modern advancements have popularized a hybrid approach: arthroscopic intra-articular release followed by an open subpectoral tenodesis. This technique removes the tendon from the bicipital groove entirely, eliminating groove-related pain.
Arthroscopic Phase
- Establish standard posterior and anterior arthroscopic portals.
- Evaluate the biceps pulley, subscapularis, and LHB tendon.
- Perform an arthroscopic tenotomy at the superior labral insertion using an electrothermal device or arthroscopic scissors.
- Address any concomitant intra-articular pathology (e.g., labral debridement, rotator cuff repair).
Open Subpectoral Phase
- Make a 2 to 3 cm longitudinal incision centered over the inferior border of the pectoralis major tendon in the axillary fold.
- Dissect through the subcutaneous tissue to identify the inferior border of the pectoralis major.
- Retract the pectoralis major superiorly and the conjoint tendon medially.
- Identify the LHB tendon within the bicipital sheath. Deliver the tendon into the wound.
- Whipstitch the distal 2 cm of the tendon using a high-strength, non-absorbable suture.
- Prepare a bone socket in the humeral shaft, approximately 1 cm distal to the bicipital groove, using a reamer matched to the tendon's diameter.
- Secure the tendon into the socket using a bio-composite interference screw or a cortical button.
Surgical Warning: During deep retraction for the subpectoral approach, avoid aggressive medial retraction of the conjoint tendon. The musculocutaneous nerve enters the coracobrachialis as close as 3 to 5 cm distal to the coracoid process and is highly susceptible to neuropraxia from heavy retraction.
Postoperative Care and Rehabilitation
The postoperative rehabilitation protocol must be carefully tailored, particularly if a concomitant rotator cuff repair was performed. The healing of the rotator cuff dictates the speed of the rehabilitation program.
Phase I: Protection Phase (Weeks 0–4)
- Immobilization: A shoulder immobilizer is worn strictly for the first 2 weeks. Following this, a standard sling is used for an additional 2 weeks.
- Range of Motion (ROM): Passive range of motion (PROM) of the shoulder is initiated early to prevent adhesive capsulitis.
- Elbow Restrictions: Active elbow flexion and active forearm supination are strictly prohibited to protect the tenodesis site. Passive elbow ROM is permitted.
Phase II: Active Motion Phase (Weeks 4–8)
- Sling Weaning: The sling is discontinued at 4 weeks.
- Active ROM: Active use and exercises for the shoulder are begun. Active-assisted range of motion (AAROM) progresses to active range of motion (AROM).
- Biceps Activation: Gentle, unresisted active elbow flexion and supination are introduced at 4 to 6 weeks.
Phase III: Strengthening Phase (Weeks 8–12)
- Resistance Training: Isotonic strengthening of the rotator cuff and periscapular stabilizers begins.
- Biceps Strengthening: Progressive resisted exercises for the biceps brachii are initiated at 8 weeks, starting with light weights and high repetitions.
Phase IV: Return to Activity (Months 3–6)
- Advanced Strengthening: Plyometric exercises and sport-specific training are introduced.
- Clearance: Return to heavy manual labor or overhead sports is typically permitted between 4 and 6 months, provided the patient has achieved full, painless ROM and symmetric strength.
Complications and Management
While biceps tenodesis is highly successful, surgeons must be prepared to manage potential complications:
- Cosmetic Deformity ("Popeye" Muscle): Occurs if the tenodesis fails or if the tendon is tensioned inadequately. Prevention relies on robust fixation (e.g., interference screw) and maintaining the physiological length-tension relationship during fixation.
- Persistent Bicipital Groove Pain: Can occur if a suprapectoral tenodesis is performed and the tendon remains within a stenotic or inflamed groove. Subpectoral tenodesis mitigates this risk.
- Nerve Injury: The axillary nerve (in the anterosuperior approach) and the musculocutaneous nerve (in the subpectoral approach) are at risk. Meticulous adherence to anatomic landmarks and gentle retraction are mandatory.
- Stiffness: Adhesive capsulitis is a risk with any shoulder surgery. Early, controlled passive motion is essential, balancing the protection of the repair with the prevention of capsular contracture.
Conclusion
The treatment of biceps brachii tendon displacement requires a nuanced understanding of shoulder pathoanatomy. While historical techniques advocated for transverse humeral ligament repair, contemporary evidence overwhelmingly supports biceps tenodesis, particularly in the presence of rotator cuff pathology. Whether utilizing an anterosuperior approach for simultaneous cuff repair, a deltopectoral approach, or an arthroscopic-assisted subpectoral technique, meticulous surgical execution and structured postoperative rehabilitation are paramount to restoring shoulder function and eliminating pain.
You Might Also Like