Acromioclavicular Joint Excision & Management: Surgical Guide
Key Takeaway
Symptomatic acromioclavicular (AC) joint disease often responds to conservative measures, including rest, NSAIDs, and intraarticular corticosteroid injections. When conservative management fails, arthroscopic distal clavicle excision is indicated. Diagnostic injections of 1% lidocaine are highly predictive of surgical success. Evidence favors an indirect subacromial arthroscopic approach to preserve the superior capsular ligaments, ensuring joint stability while adequately preventing bony impingement.
ACROMIOCLAVICULAR JOINT PATHOLOGY AND MANAGEMENT
The acromioclavicular (AC) joint is a diarthrodial joint that serves as the sole articulation between the clavicle and the scapula, playing a critical role in the biomechanics of the shoulder girdle. Pathologic conditions affecting the AC joint—most commonly primary osteoarthritis, post-traumatic arthritis, and distal clavicular osteolysis—are frequent sources of anterior and superior shoulder pain.
Because the AC joint undergoes significant contact stresses during overhead activities and horizontal adduction, degenerative changes are ubiquitous in the aging population. However, radiographic degeneration correlates poorly with clinical symptoms. Therefore, the orthopedic surgeon must rely on a meticulous clinical examination and targeted diagnostic modalities to isolate the AC joint as the primary pain generator before considering surgical intervention.
Conservative Management Protocols
Symptomatic disease of the acromioclavicular joint usually responds favorably to a structured regimen of conservative measures. First-line treatment should always be exhausted before surgical resection is contemplated.
- Activity Modification: Avoidance of the offending activities, particularly repetitive overhead lifting, dips, bench presses, and cross-body adduction movements.
- Pharmacotherapy: A scheduled course of oral nonsteroidal anti-inflammatory drugs (NSAIDs) to reduce capsular inflammation.
- Intraarticular Corticosteroid Injections: Image-guided (ultrasound or fluoroscopic) or landmark-guided injections of a corticosteroid mixed with a local anesthetic can provide both diagnostic confirmation and profound therapeutic relief.
- Physical Therapy: Focused on periscapular stabilization and rotator cuff strengthening to optimize glenohumeral kinematics and reduce compensatory stresses on the AC joint.
Clinical Pearl: If no symptoms are referable to the acromioclavicular joint during physical examination, despite the presence of severe radiographic degeneration, the distal clavicle must not be resected. Prophylactic resection in asymptomatic patients is contraindicated and may lead to iatrogenic instability.
Diagnostic Evaluation and Surgical Indications
The decision to proceed with surgical débridement or resection of the acromioclavicular joint is predicated on a triad of clinical findings, radiographic evidence, and a positive response to a diagnostic injection.
Physical Examination:
Distal clavicular excision is indicated if the AC joint is exquisitely tender to direct superior palpation and pain is reliably reproduced at the joint with horizontal adduction of the shoulder (the cross-body adduction test, which dynamically compresses the joint). The O'Brien active compression test and Paxinos sign may also be positive.
Radiographic Evaluation:
Standard shoulder series should be supplemented with a Zanca view (an anteroposterior radiograph with a 10- to 15-degree cephalad tilt) to accurately profile the AC joint without superimposition of the scapular spine. Findings typically include joint space narrowing, subchondral sclerosis, osteophyte formation, and cystic changes in the distal clavicle.
The Diagnostic Injection (The Gold Standard):
Injecting the acromioclavicular joint with 1% lidocaine (without epinephrine) is the most reliable predictor of surgical success.
* Relief of 80% to 100% of the patient's baseline pain following the injection indicates a high likelihood of good to excellent postoperative results.
* Failure to achieve significant pain relief suggests an alternative pathology (e.g., subacromial impingement, rotator cuff tear, or cervical radiculopathy) and contraindicates isolated AC joint resection.
BIOMECHANICS AND EVIDENCE-BASED SURGICAL APPROACHES
When conservative measures fail, surgical intervention involves the excision of the distal clavicle (traditionally known as the Mumford procedure). The evolution of this procedure has transitioned from open resection to arthroscopic techniques, which offer decreased morbidity, preservation of the deltotrapezial fascia, and faster rehabilitation.
Arthroscopic distal clavicle excision can be performed via two primary approaches: the direct (superior) approach and the indirect (subacromial) approach.
The Direct vs. Indirect Arthroscopic Approach
Extensive biomechanical and clinical studies have evaluated the optimal approach and the required extent of resection to prevent impingement while maintaining joint stability.
1. Subacromial (Indirect) Approach Efficacy:
Snyder et al. reported good-to-excellent long-term results in 47 (94%) of 50 arthroscopic distal clavicular resections utilizing a subacromial approach and a claviculizer (Smith & Nephew, Memphis, TN). This approach allows for simultaneous evaluation and treatment of subacromial pathology.
2. Biomechanical Stability (Miller et al. & Matthews et al.):
Miller et al. performed arthroscopic AC joint resections using both direct and indirect approaches in a cadaveric model. Biomechanical testing post-resection revealed no significant difference in AC joint instability between the two techniques.
Likewise, in a cadaveric study comparing open with arthroscopic AC joint resections, Matthews et al. found no significant differences in the stability of the two joints, though both were significantly more unstable than the nonoperative native joint. Crucially, Matthews et al. demonstrated that a conservative 5-mm arthroscopic resection is sufficient to prevent bony impingement at the AC joint during maximal physiologic motion.
3. Coplaning vs. Resection (Barber Study):
In a comprehensive 6-year follow-up study, Barber compared three distinct groups of patients treated with:
* Subacromial decompression and associated coplaning of the clavicle (removing only the inferior osteophytes).
* 50% resection of the undersurface of the clavicle.
* Complete arthroscopic acromioclavicular joint resection.
All groups were evaluated using validated functional and symptomatic metrics, including the American Shoulder and Elbow Surgeons (ASES) score, Rowe score, and Constant-Murley score. Barber found that all three groups achieved comparable scores and comparable relief of symptoms. He concluded that AC joint coplaning, partial clavicle resection, or full AC joint resection did not negatively alter the results of the acromioplasty. Furthermore, complications related to AC joint decompression were primarily attributed to inadequate decompression rather than the specific technique utilized.
4. Long-Term Clinical Outcomes (Levine et al.):
In a landmark long-term follow-up study of 66 shoulders in 60 patients, Levine et al. compared arthroscopic direct and indirect AC joint resections.
* Forty-two patients underwent a direct approach. Of these, four required reoperation (two to stabilize an iatrogenically unstable AC joint, and two for revision AC joint resection at 5 years).
* Levine et al. suggested that the direct approach inherently risks injury to the superior capsular ligaments, which are the primary restraints to anteroposterior translation, thereby leading to distal clavicular instability.
Surgical Warning: Based on long-term follow-up data and cadaveric studies showing no added benefit to the direct AC joint resection, the indirect (subacromial) approach is generally preferred. It is quicker, allows for easier evaluation of concomitant subacromial pathology, preserves the critical superior AC capsular ligaments, and is reliably associated with adequate subacromial decompression.
SURGICAL TECHNIQUE: ARTHROSCOPIC INDIRECT DISTAL CLAVICLE EXCISION
Patient Positioning and Setup
- Anesthesia: General anesthesia is typically employed, often supplemented with an interscalene regional nerve block for postoperative pain control.
- Positioning: The patient is placed in either the beach-chair or lateral decubitus position, depending on surgeon preference.
- Preparation: The operative arm is prepped and draped in a standard sterile fashion. If in the lateral decubitus position, 10 to 15 pounds of balanced suspension traction is applied.
Portal Placement and Diagnostic Arthroscopy
- A standard posterior viewing portal is established. A thorough diagnostic arthroscopy of the glenohumeral joint is performed to rule out intra-articular pathology (e.g., SLAP tears, chondral defects).
- The arthroscope is redirected into the subacromial space.
- A lateral working portal is established under direct visualization, typically 2 to 3 cm lateral to the acromion.
- An anterior portal may be established just lateral to the coracoid process to assist with instrumentation and fluid management.
Subacromial Decompression and AC Joint Identification
- A motorized shaver and radiofrequency ablation wand are introduced through the lateral portal to perform a thorough subacromial bursectomy. This step is critical for visualizing the coracoacromial (CA) ligament and the undersurface of the acromion.
- The CA ligament is traced medially to its insertion on the acromion. Just medial to this insertion lies the AC joint.
- The inferior capsule of the AC joint is ablated to expose the distal clavicle and the medial facet of the acromion. Bleeding from the distal clavicle is controlled with electrocautery.
Resection of the Distal Clavicle
- A 4.0-mm or 5.5-mm arthroscopic burr (claviculizer) is introduced through the lateral or anterior portal.
- Resection begins at the anterior aspect of the distal clavicle and proceeds posteriorly.
- Resection Depth: The goal is to resect approximately 5 to 8 mm of the distal clavicle. As demonstrated by Matthews et al., a 5-mm resection is generally sufficient to prevent impingement.
- Preservation of Superior Capsule: Extreme care must be taken to angle the burr appropriately to avoid violating the superior AC capsular ligaments. The superior capsule must remain intact to prevent postoperative anteroposterior instability of the clavicle.
- Verification: Once the resection is complete, the arthroscope is advanced into the resected space. The surgeon should be able to pass the 5.5-mm burr freely between the distal clavicle and the acromion. Dynamic testing is performed by internally rotating and cross-body adducting the patient's arm while visualizing the joint to ensure no residual bony contact occurs.
CONCOMITANT PATHOLOGY: ROTATOR CUFF AND SUBSCAPULARIS REPAIR
Isolated acromioclavicular joint arthritis is relatively uncommon; it is frequently accompanied by subacromial impingement syndrome, supraspinatus tears, or anterior shoulder pathology such as subscapularis tendon tears. During the diagnostic glenohumeral arthroscopy phase, the subscapularis must be meticulously evaluated using a 30-degree or 70-degree arthroscope.
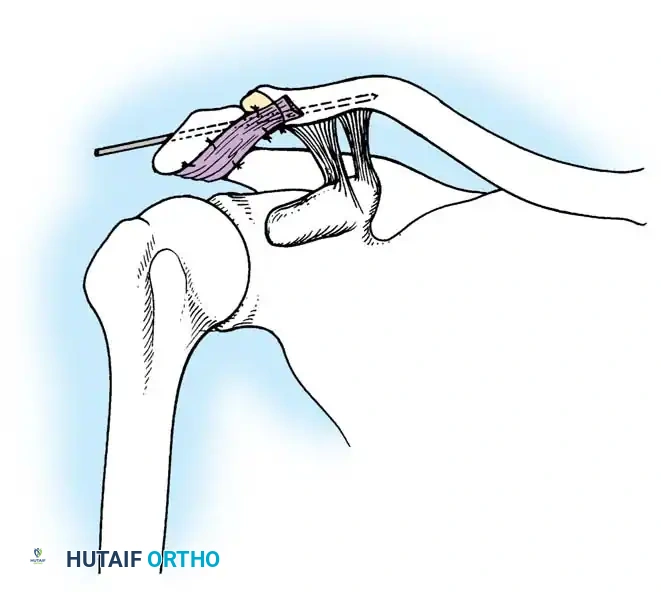
If a subscapularis tear is identified, it should be addressed prior to transitioning to the subacromial space for the AC joint resection. Advanced techniques, such as the Burkhart and Tehrany subscapularis repair, utilize traction sutures to mobilize the retracted tendon back to its anatomic footprint on the lesser tuberosity.
FIGURE 52-50 Burkhart and Tehrany subscapularis tendon repair. Superior view of suture passage through subscapularis tendon as traction is maintained on tendon.
Subscapularis Repair Principles
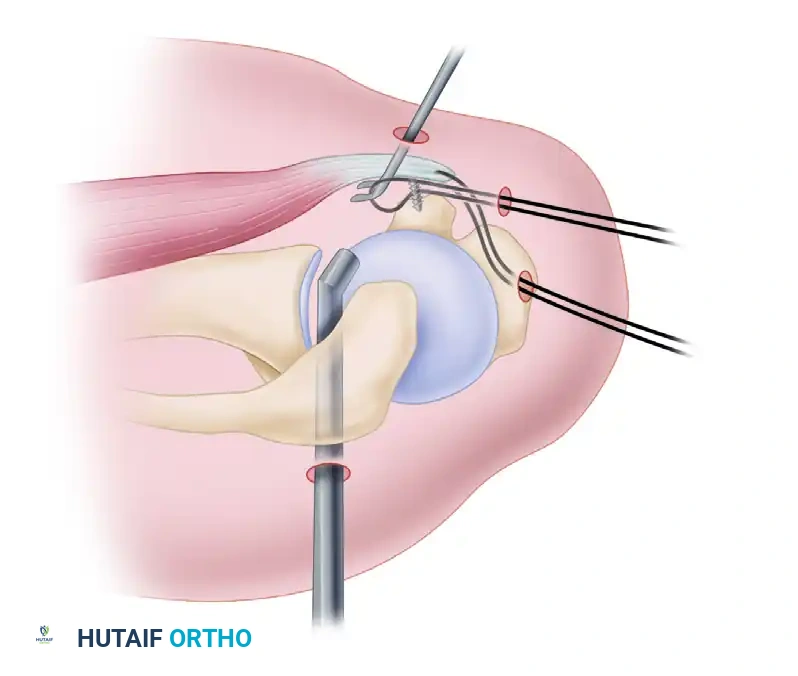
As illustrated in the Burkhart and Tehrany technique, managing a retracted subscapularis tendon requires precise suture management:
1. Traction Suture: A traction suture is passed through the superior border of the subscapularis tendon. This allows the surgeon to apply lateral and superior tension, mobilizing the tendon and assessing its excursion toward the lesser tuberosity footprint.
2. Footprint Preparation: The lesser tuberosity is decorticated using a burr to create a bleeding bone bed, optimizing biological healing.
3. Anchor Placement: Suture anchors are placed at the articular margin of the lesser tuberosity.
4. Suture Passage: Using a specialized suture passer (e.g., a penetrator or birdbeak device), the anchor sutures are shuttled through the tendon while traction is maintained.
5. Knot Tying/Fixation: The sutures are tied or secured with knotless technology, compressing the tendon securely against the prepared footprint.
Addressing concomitant subscapularis pathology ensures that the anterior force couples of the shoulder are restored, which is vital for optimal postoperative kinematics following an AC joint resection.
POSTOPERATIVE REHABILITATION PROTOCOL
The rehabilitation protocol following an isolated arthroscopic distal clavicle excision is generally accelerated, though it must be modified if concomitant procedures (such as a subscapularis or supraspinatus repair) are performed.
Phase I: Immediate Postoperative (Weeks 0-2)
* The patient is placed in a standard clinical sling for comfort.
* Cryotherapy is utilized to minimize hemarthrosis and swelling.
* Active range of motion (AROM) of the elbow, wrist, and hand is encouraged immediately.
* Passive range of motion (PROM) and active-assisted range of motion (AAROM) of the shoulder are initiated as tolerated. Cross-body adduction is avoided to prevent stress on the healing AC joint capsule.
Phase II: Intermediate Phase (Weeks 2-6)
* The sling is discontinued.
* Full AROM is progressively achieved in all planes.
* Isometrics for the rotator cuff and periscapular musculature are initiated.
* Closed kinetic chain exercises are introduced to promote scapulothoracic rhythm.
Phase III: Strengthening Phase (Weeks 6-12)
* Progressive resistive exercises (PREs) are initiated for the deltoid, rotator cuff, and scapular stabilizers.
* Patients may gradually return to light overhead activities and weightlifting, avoiding heavy bench presses or dips until 10 to 12 weeks postoperatively.
COMPLICATIONS AND PITFALLS
While arthroscopic distal clavicle excision is highly successful, complications can arise, primarily due to technical errors during the resection phase.
- Inadequate Resection: The most common cause of persistent postoperative pain. Failure to resect the posterior-superior corner of the distal clavicle can lead to residual impingement. The surgeon must ensure a uniform 5 to 8 mm gap across the entire AP dimension of the joint.
- Iatrogenic Instability: Over-resection (greater than 10-12 mm) or violation of the superior AC capsular ligaments via a direct approach can destabilize the clavicle, leading to painful anteroposterior translation.
- Heterotopic Ossification: Bone formation within the resected gap can occur, bridging the space and causing recurrent symptoms. Thorough irrigation of the subacromial space and meticulous hemostasis reduce the risk of bone dust settling and ossifying.
- Infection and Stiffness: As with any arthroscopic procedure, there is a low risk of septic arthritis or postoperative adhesive capsulitis. Early, controlled mobilization is key to preventing stiffness.
You Might Also Like