ABOS Part I Orthopaedic Exam Review: Shoulder Instability & PVNS MCQs | Part 22215

Key Takeaway
The ABOS Part I Orthopaedic Review module covers high-yield clinical cases for exam preparation. Key topics include recurrent anterior glenohumeral instability, its diagnosis (CT, Pico method), surgical management (Latarjet, Bankart, Remplissage), and rehabilitation. It also delves into Pigmented Villonodular Synovitis (PVNS)/Diffuse TGCT, detailing its clinical presentation, MRI findings, genetic basis, and treatment strategies like synovectomy and Pexidartinib.
ABOS Part I Orthopaedic Exam Review: Shoulder Instability & PVNS MCQs | Part 22215
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 28-year-old male presents with his third episode of anterior glenohumeral dislocation. Initial imaging in the emergency department confirms the dislocation. Given the patient's history and the provided radiograph, which of the following is the most appropriate next step in diagnostic evaluation after successful reduction?

Explanation
Correct Answer: C
Explanation:
The patient's history of recurrent anterior glenohumeral dislocations (third episode in 18 months) and the mechanism of injury (high-energy fall during rugby with arm abducted and externally rotated) strongly suggest significant underlying structural damage, particularly bipolar bone loss (Hill-Sachs lesion and anterior glenoid bone loss). The initial AP radiograph confirms the dislocation but is insufficient for quantifying these osseous defects.
- Option C (Order a non-contrast Computed Tomography (CT) scan with 3D reconstructions) is the correct answer. The case explicitly states that 'non-contrast Computed Tomography (CT) with 3D reconstructions is the gold standard for evaluating osseous architecture' and is essential for 'quantifying bipolar bone loss' and 'accurate preoperative planning.' This advanced imaging is crucial to determine the extent of glenoid bone loss and the Hill-Sachs lesion, which dictates the appropriate surgical strategy (e.g., Bankart, Remplissage, Latarjet).
- Option A (Immediate referral for physical therapy to initiate rotator cuff strengthening) is premature and potentially harmful. While rehabilitation is critical post-operatively, without addressing the underlying structural instability, rotator cuff strengthening alone is unlikely to prevent recurrence in a patient with significant bone loss and recurrent dislocations.
- Option B (Obtain a stress radiograph series to assess for ligamentous laxity) is not the primary diagnostic step for recurrent instability with suspected bone loss. While ligamentous laxity can contribute, the immediate concern in this case is osseous deficiency, which stress radiographs do not adequately evaluate.
- Option D (Proceed directly to arthroscopic Bankart repair planning) is incorrect because the type of surgical repair depends entirely on the quantification of bone loss. An isolated Bankart repair would likely fail if critical glenoid bone loss or an 'off-track' Hill-Sachs lesion is present, as highlighted in the case.
- Option E (Prescribe a sling for 6 weeks with strict immobilization) represents non-operative management, which is explicitly contraindicated for recurrent instability with significant bone loss, especially in a young, competitive contact athlete. The case states, 'Recurrent instability with significant bone loss' is a contraindication for non-operative management.
Question 2
Following successful reduction and initial radiographs, a CT scan with 3D reconstructions is obtained for the 28-year-old rugby player. The CT scan, as depicted, reveals significant anterior glenoid bone loss. Based on the case description and the image, which method is widely employed to measure anterior glenoid bone loss on en face 3D CT views?

Explanation
Correct Answer: C
Explanation:
Accurate quantification of glenoid bone loss is critical for surgical decision-making in recurrent anterior shoulder instability.
- Option C (The Pico method, drawing a best-fit circle over the inferior portion of the intact glenoid) is the correct answer. The case explicitly states, 'The Pico method is widely employed to measure anterior glenoid bone loss on en face 3D CT views. A best-fit circle is drawn over the inferior portion of the intact glenoid (or the contralateral normal glenoid for comparison), and the area or width of the missing anterior bone is calculated as a percentage of the total circle.' This method provides a quantitative assessment of the bone defect.
- Option A (The Sugaya method, measuring the glenoid width on an axial MRI slice) is a method for assessing glenoid bone loss, but it is typically performed on MRI and measures the width, not necessarily the area based on a best-fit circle as described for the Pico method on CT. The case specifically mentions the Pico method for 3D CT.
- Option B (The Hill-Sachs interval measurement on a sagittal CT view) is used to quantify the Hill-Sachs lesion itself and its relationship to the glenoid, not primarily for measuring anterior glenoid bone loss.
- Option D (The glenoid track calculation, assessing the engagement of the Hill-Sachs lesion) is a biomechanical concept that integrates both glenoid bone loss and the Hill-Sachs lesion to determine if the Hill-Sachs lesion is 'on-track' or 'off-track.' While crucial for decision-making, it is not a direct method for measuring the anterior glenoid bone loss percentage itself.
- Option E (The 'inverted pear' sign, qualitatively assessing the glenoid shape) is a qualitative description of significant glenoid bone loss, where the normal pear shape of the glenoid becomes inverted due to erosion of the anterior-inferior aspect. While a relevant concept, it is a qualitative observation rather than a quantitative measurement method like the Pico method.
Question 3
The 28-year-old rugby player is found to have critical glenoid bone loss (>15%) and an 'off-track' Hill-Sachs lesion. An open Latarjet procedure is planned. During the procedure, as depicted in the image, the coracoid graft is being fixed to the anterior glenoid. Which of the following statements regarding the critical technical aspects of graft positioning and fixation is most accurate?

Explanation
Correct Answer: C
Explanation:
The Latarjet procedure requires meticulous technique to achieve stability and prevent complications.
- Option C (The graft should be positioned flush with, or slightly medial (1-2 mm) to, the articular cartilage of the anterior glenoid rim) is the correct answer. The case explicitly states, 'The prepared coracoid graft is passed through the subscapularis split. It is positioned flush with, or slightly medial (1-2 mm) to, the articular cartilage of the anterior glenoid rim.' This precise positioning is crucial to restore the glenoid arc without causing iatrogenic osteoarthritis.
- Option A (The graft should be positioned 5mm lateral to the articular cartilage to maximize the blocking effect) is incorrect. The case warns, 'Positioning the graft lateral to the cartilage risks severe osteoarthritis.' While a blocking effect is desired, it must be achieved without encroaching on the articular surface.
- Option B (The graft should be fixed with a single screw to allow for dynamic compression) is incorrect. The case states, 'Two 3.75 mm or 4.0 mm partially threaded cannulated screws are inserted over the K-wires to achieve rigid bicortical compression.' Two screws provide more stable fixation and prevent rotation of the graft.
- Option D (The subscapularis split should be performed at the junction of the inferior two-thirds and superior one-third to protect the axillary nerve) is incorrect. The case states, 'A longitudinal split is created in the subscapularis tendon, typically at the junction of the superior two-thirds and inferior one-third, to protect the axillary nerve traversing inferiorly.' Reversing the split location would place the axillary nerve at greater risk.
- Option E (The coracoacromial ligament should be completely excised to prevent impingement) is incorrect. The case states, 'The coracoacromial ligament is sharply released from the lateral aspect of the coracoid, leaving a 1 cm stump for later capsular repair.' This stump is used to repair the native capsule, contributing to the stability.
Question 4
A 28-year-old rugby player with recurrent anterior shoulder instability and an 'off-track' Hill-Sachs lesion, but subcritical glenoid bone loss (<13.5%), undergoes an arthroscopic Bankart repair combined with a remplissage procedure. During the diagnostic arthroscopy, the anterior labrum and capsule are mobilized from the anterior glenoid neck, as shown in the image. Which of the following steps is most critical to ensure adequate superior shift during the anterior Bankart repair?
Explanation
Correct Answer: C
Explanation:
The arthroscopic Bankart repair aims to reattach the avulsed labrum and tighten the anterior capsule to restore stability.
- Option C (Releasing the tissue inferiorly to the 6 o'clock position) is the correct answer. The case states, 'The anterior labrum and capsule are meticulously mobilized from the anterior glenoid neck using an elevator and electrocautery. It is critical to release the tissue inferiorly to the 6 o'clock position to allow for adequate superior shift during repair.' This extensive release is essential to achieve sufficient capsular shift and tension, which is key to preventing recurrent instability.
- Option A (Decorticating the anterior glenoid neck with a motorized burr) is an important step to create a bleeding bone bed for biological healing, but it does not directly facilitate the superior capsular shift.
- Option B (Placing suture anchors superiorly at the 1 o'clock position) is generally not the starting point for Bankart repair. Anchors are typically placed from inferiorly (5:30 position) and progressed superiorly to the 3:00 position to restore the anterior bumper and achieve the desired capsular shift.
- Option D (Passing sutures through only the labrum, avoiding the capsule) is incorrect. The sutures should pass through the 'capsulolabral complex,' ensuring a healthy bite of the inferior glenohumeral ligament to achieve the superior and lateral capsular shift, as described in the case.
- Option E (Performing the remplissage procedure after tying the anterior Bankart anchors) is incorrect. The case states, 'Before tying the anterior Bankart anchors, the remplissage is addressed... These sutures are left untied until the anterior repair is complete.' The remplissage sutures are tied after the anterior repair is complete, but the anchors are placed before tying the Bankart anchors.
Question 5
A 28-year-old rugby player undergoes an open Latarjet procedure for recurrent anterior shoulder instability with critical glenoid bone loss. Postoperatively, the patient reports numbness and weakness in the biceps and brachialis muscles. Which of the following nerves is most likely injured during the procedure?
Explanation
Correct Answer: D
Explanation:
Understanding the neurovascular anatomy around the shoulder is crucial for preventing and identifying complications during Latarjet surgery.
- Option D (Musculocutaneous nerve) is the correct answer. The case explicitly states under 'Intraoperative Complications' that 'The musculocutaneous nerve enters the conjoint tendon as proximally as 3 to 5 cm distal to the coracoid tip and is at risk during graft harvest and retraction.' The musculocutaneous nerve innervates the biceps brachii and brachialis muscles, and its injury would lead to the described symptoms of numbness and weakness in these muscles.
- Option A (Axillary nerve) is also at risk during the Latarjet procedure, particularly during inferior capsular release and subscapularis split. Injury to the axillary nerve would primarily affect deltoid function (shoulder abduction) and sensation over the regimental badge area, which is different from the symptoms described.
- Option B (Radial nerve) injury would typically manifest as wrist drop and weakness in forearm extensors, which is not consistent with the patient's symptoms.
- Option C (Ulnar nerve) injury would affect intrinsic hand muscles and sensation along the medial forearm and hand, which is not consistent with the patient's symptoms.
- Option E (Suprascapular nerve) injury would primarily affect the supraspinatus and infraspinatus muscles, leading to weakness in shoulder abduction and external rotation, not biceps/brachialis weakness.
Question 6
The biomechanical concept of the 'glenoid track' is central to understanding recurrent anterior shoulder instability with bipolar bone loss. For the 28-year-old rugby player, if his intact inferior glenoid width is measured at 25 mm, what is the calculated width of his glenoid track?
Explanation
Correct Answer: B
Explanation:
The glenoid track concept is a critical biomechanical principle for surgical decision-making in shoulder instability.
- Option B (Approximately 20.75 mm) is the correct answer. The case states, 'The glenoid track is the zone of contact between the humeral head and the glenoid during maximum abduction and external rotation. Its width is calculated as 83 percent of the intact inferior glenoid width.' Therefore, for an intact inferior glenoid width of 25 mm, the glenoid track width would be 0.83 * 25 mm = 20.75 mm.
- Option A (Approximately 15 mm) is incorrect. This value is not derived from the 83% calculation.
- Option C (Approximately 25 mm) is incorrect. This represents the full intact glenoid width, not the glenoid track width.
- Option D (Approximately 13.5 mm) is incorrect. This value is mentioned in the case as a threshold for glenoid bone loss (13.5-15%), not the glenoid track calculation.
- Option E (Approximately 8.3 mm) is incorrect. This value is not derived from the 83% calculation.
Question 7
The 28-year-old rugby player has a history of three anterior glenohumeral dislocations. The case highlights that 'failure to address bipolar bone loss is the leading cause of surgical failure following isolated arthroscopic soft-tissue stabilization.' Which of the following patient characteristics or findings would most strongly indicate a need for an osseous augmentation procedure (e.g., Latarjet) rather than an isolated arthroscopic Bankart repair?
Explanation
Correct Answer: D
Explanation:
The decision between soft-tissue repair and osseous augmentation is primarily driven by the extent of bone loss and the engagement of the Hill-Sachs lesion.
- Option D (Critical glenoid bone loss (>15%) and an 'off-track' Hill-Sachs lesion) is the correct answer. The case explicitly states under 'Indications and Contraindications' that 'Open Latarjet Procedure' is indicated for 'Critical glenoid bone loss (> 15%)' and 'Off-track Hill-Sachs lesions.' This combination represents the highest risk for recurrence with soft-tissue repair alone and necessitates bone augmentation.
- Option A (First-time dislocation in a high-demand contact athlete) might warrant an arthroscopic Bankart repair, but without recurrent instability or quantified bone loss, it does not automatically indicate an osseous augmentation procedure. The case lists 'First-time dislocators in high-demand sports' as an indication for 'Arthroscopic Bankart Repair.'
- Option B (An 'on-track' Hill-Sachs lesion with minimal glenoid bone loss (<13.5%)) would typically be managed with an arthroscopic Bankart repair, possibly with a remplissage if the Hill-Sachs is 'off-track' but glenoid bone loss is subcritical. This scenario does not necessitate a Latarjet.
- Option C (A positive sulcus sign indicating generalized ligamentous laxity) is a risk factor for instability but does not, by itself, mandate osseous augmentation. It might influence the choice of soft-tissue repair technique (e.g., more aggressive capsular plication) but is not the primary driver for bone grafting.
- Option E (Age over 30 years with a sedentary lifestyle) generally correlates with a lower risk of recurrence compared to younger, active individuals. This demographic might even be considered for non-operative management if it were a first-time dislocation, but it does not indicate a need for osseous augmentation.
Question 8
During the postoperative rehabilitation for an arthroscopic Bankart repair, the patient is in the early protective phase (Weeks 0 to 4). Which of the following is the most appropriate instruction regarding external rotation?
Explanation
Correct Answer: C
Explanation:
The early protective phase of rehabilitation is crucial for protecting the surgical repair and preventing re-injury.
- Option C (External rotation is strictly limited to 0 degrees) is the correct answer. The case states under 'Early Protective Phase' (Weeks 0 to 4) for arthroscopic Bankart repairs, 'external rotation is strictly limited to 0 degrees to protect the anterior capsular repair and the subscapularis split.' This restriction is vital to prevent undue stress on the reattached labrum and tightened capsule, which are most vulnerable in external rotation.
- Option A (Passive external rotation to 45 degrees is permitted) is incorrect. This level of external rotation is typically introduced later, in the intermediate mobilization phase (Weeks 4 to 8), and even then, it is gradually increased.
- Option B (Active external rotation to 30 degrees is encouraged) is incorrect. Active motion, especially against resistance, is generally avoided in the early protective phase to prevent stress on the repair.
- Option D (Active-assisted external rotation to tolerance is allowed) is incorrect for the early protective phase. Any significant external rotation, even active-assisted, can jeopardize the repair.
- Option E (No restrictions on external rotation, as long as it is pain-free) is incorrect and dangerous. Pain is not the sole indicator of safety in the early postoperative period; strict adherence to protocol is necessary to protect the healing tissues.
Question 9
The case describes the Latarjet procedure's 'triple-blocking effect.' Which of the following components contributes to this effect?
Explanation
Correct Answer: C
Explanation:
The Latarjet procedure provides stability through a combination of mechanisms, known as the triple-blocking effect.
- Option C (The dynamic sling effect of the conjoint tendon traversing the subscapularis) is the correct answer. The case explicitly states, 'The Latarjet procedure is the workhorse for recurrent instability associated with critical glenoid bone loss (> 15%) or in high-demand contact athletes. It relies on a triple-blocking effect: the osseous augmentation of the glenoid, the dynamic sling effect of the conjoint tendon traversing the subscapularis, and the capsular repair to the coracoacromial ligament stump.' The conjoint tendon (biceps short head and coracobrachialis) acts as a dynamic restraint, particularly with the arm in abduction and external rotation.
- Option A (The tenodesis of the infraspinatus into the Hill-Sachs lesion) describes the remplissage procedure, which is a different technique used for off-track Hill-Sachs lesions, not a component of the Latarjet's triple-blocking effect.
- Option B (The restoration of the glenoid track width by the coracoid graft) is partially correct in that the osseous augmentation restores the glenoid's articular arc, but the 'glenoid track' is a concept for Hill-Sachs engagement, not a direct component of the Latarjet's triple-blocking effect as described. The osseous augmentation is one of the three effects, but this option describes it in terms of glenoid track width restoration, which is not the primary description of the triple-blocking effect.
- Option D (The increased concavity compression provided by the rotator cuff) refers to the general dynamic stability provided by the rotator cuff, which is not specific to the Latarjet procedure's unique blocking mechanisms.
- Option E (The repair of the posterior capsule to the coracoacromial ligament stump) is incorrect. The repair is of the native capsule to the stump of the coracoacromial ligament, and it is the anterior capsule, not posterior, that is repaired to the stump. This capsular repair is indeed one of the three blocking effects, but the option incorrectly states 'posterior capsule.'
Question 10
A 28-year-old right-hand dominant male presents with his third episode of anterior glenohumeral dislocation. The mechanism of injury involved direct impact to the posterior aspect of the shoulder while the arm was abducted and externally rotated. The patient is an active participant in competitive contact sports. Based on the epidemiological data and clinical presentation in the case, which of the following statements regarding his risk of recurrence is most accurate?
Explanation
Correct Answer: B
Explanation:
The case provides specific epidemiological data and patient characteristics that influence the risk of recurrence.
- Option B (Non-operative management would likely result in a recurrence rate approaching 90%) is the correct answer. The case states, 'Studies have demonstrated that patients under the age of 20 face a recurrence rate approaching 90 percent with non-operative management.' While this patient is 28, he is a young, competitive contact athlete with a history of recurrent dislocations. The case also lists 'Recurrent instability with significant bone loss; Young, competitive contact athletes' as contraindications for non-operative management, implying a very high risk of failure if non-operative management were pursued. Given his history of three dislocations and participation in contact sports, his risk with non-operative management would be extremely high, likely similar to or exceeding the 90% for those under 20.
- Option A (His risk of recurrence is low due to his age being over 25) is incorrect. While the risk decreases with age, a 28-year-old competitive contact athlete with recurrent dislocations still has a very high risk, especially if bone loss is present. The case highlights that 'males in their second and third decades of life engaged in contact sports' have a significant predilection for primary dislocations and high recurrence rates.
- Option C (His risk of recurrence is primarily due to generalized ligamentous laxity) is not explicitly stated as the primary cause in the case. While hyperlaxity can contribute, the case emphasizes 'progressive structural damage, most notably bipolar bone loss' as a consequence of recurrent instability.
- Option D (The high-energy mechanism of injury suggests a lower risk of recurrence compared to atraumatic dislocations) is incorrect. High-energy trauma, especially in contact sports, is associated with significant structural damage (like bone loss) that increases the risk of recurrence, not lowers it. Atraumatic dislocations often have different underlying etiologies (e.g., multidirectional instability).
- Option E (The risk of recurrence is negligible after the third dislocation, as the joint has 'stretched out') is incorrect. This is a dangerous misconception. Each subsequent dislocation exacerbates structural damage, making recurrence more likely and leading to progressive joint degeneration. The case states, 'Recurrent instability inevitably leads to progressive structural damage.'
Question 11
A 38-year-old male presents with a 2-year history of insidious left knee pain, intermittent swelling, and mechanical symptoms. Over the past 6 months, symptoms progressed to constant pain and persistent, boggy effusion. Prior aspirations yielded dark, serosanguinous fluid, negative for crystals and infection. Physical examination reveals a doughy effusion, significant synovial thickening, and a 5° flexion contracture with maximal flexion to 100°. Plain radiographs show a moderate effusion, preserved joint space, and subtle marginal subchondral erosions. Given this clinical picture, which of the following is the most likely diagnosis?
Explanation
Correct Answer: C - Pigmented Villonodular Synovitis (PVNS)
The patient's presentation is classic for Pigmented Villonodular Synovitis (PVNS), now classified as diffuse Tenosynovial Giant Cell Tumor (TGCT). Key features include the insidious onset of chronic knee pain, persistent boggy (doughy) joint effusion, mechanical symptoms, and recurrent aspirations yielding dark, serosanguinous fluid. The preserved joint space on radiographs despite chronic symptoms, coupled with subtle marginal erosions, further supports PVNS. The synovial thickening palpable on examination is also characteristic of the proliferative nature of PVNS.
- A. Septic Arthritis: This is unlikely. While the patient has a chronic effusion and pain, prior synovial fluid analyses were negative for infection (Gram stain and cultures), and there are no systemic signs of infection (fever, chills, warmth, erythema).
- B. Rheumatoid Arthritis: While RA can cause synovial hypertrophy and erosions, the presentation is typically polyarticular, and synovial fluid is inflammatory with a high WBC count (often >2,000 cells/mm3) and a neutrophil predominance. The patient's normal ESR/CRP and mononuclear fluid analysis make RA less likely, especially in a monoarticular presentation without other systemic features.
- D. Synovial Chondromatosis: This condition is characterized by the formation of cartilaginous or osteocartilaginous loose bodies within the joint. While it can cause mechanical symptoms and chronic pain, the synovial fluid is typically clear to yellow, and radiographs or MRI would show calcified loose bodies, which were not described as the primary finding in this case.
- E. Hemophilic Arthropathy: This is ruled out by the patient's negative history of bleeding diatheses or coagulopathies, and normal coagulation panel results. While hemophilic arthropathy also causes recurrent hemarthroses and hemosiderin deposition, it occurs in patients with known clotting factor deficiencies.
Question 12
The patient's plain radiographs demonstrated a moderate to large joint effusion and relatively preserved tibiofemoral and patellofemoral joint spaces. However, close inspection revealed subtle, well-marginated radiolucent lesions at the margins of the medial femoral condyle and the posterior aspect of the tibial plateau. Which of the following terms best describes these specific radiographic findings in the context of this patient's likely diagnosis?
Explanation
Correct Answer: C - Marginal subchondral erosions
The case explicitly states that plain radiographs revealed "subtle, well-marginated radiolucent lesions—subchondral erosions—at the margins of the medial femoral condyle and the posterior aspect of the tibial plateau." These erosions, occurring at the capsular reflections (often referred to as 'bare areas' where cartilage ends and synovium begins), are a highly characteristic, albeit subtle, radiographic finding in Pigmented Villonodular Synovitis (PVNS). They represent direct invasion of the subchondral bone by the aggressive, proliferative synovial tissue.
- A. Subchondral cysts: While cysts can occur in various arthropathies, the description of lesions at the 'margins' and 'capsular reflections' specifically points to erosions rather than typical subchondral cysts, which are usually centrally located within the bone beneath the cartilage.
- B. Osteophytes: These are bony outgrowths indicative of osteoarthritis. The case explicitly states there were "no obvious osteophytes" and "no gross joint space narrowing that would characterize advanced osteoarthritis," making this incorrect.
- D. Periosteal reactions: These indicate new bone formation along the periosteum, often seen in infection, trauma, or tumors. While PVNS is a tumor-like condition, the described lesions are intra-articular and subchondral, not periosteal.
- E. Geodes: This is another term for subchondral cysts, which, as explained above, does not precisely fit the description of marginal lesions at capsular reflections.
Question 13
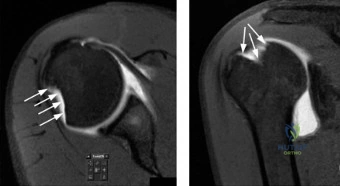
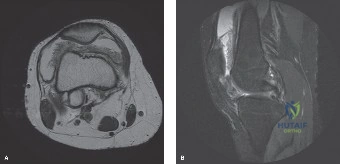
Following plain radiographs, an MRI of the left knee was performed. The image below is a representative sequence from this MRI study.
Which of the following MRI findings, clearly depicted in the case description and often visible on sequences like the one shown, is considered pathognomonic for Pigmented Villonodular Synovitis (PVNS)?
Explanation
Correct Answer: C - Diffuse synovial thickening with low signal intensity on T1- and T2-weighted sequences and prominent blooming on GRE
The case explicitly states that the "most critical and pathognomonic finding was the presence of extensive areas of low signal intensity on both T1- and T2-weighted sequences within the hypertrophic synovial masses. On the Gradient-Recalled Echo (GRE) sequences, these areas demonstrated a prominent 'blooming artifact.' This magnetic susceptibility artifact is caused by the paramagnetic properties of extensive hemosiderin deposition within the synovial tissue, a hallmark of Pigmented Villonodular Synovitis (PVNS)." The provided image, while not explicitly labeled as GRE, shows diffuse, dark (low signal) synovial tissue, consistent with hemosiderin deposition.
- A. Extensive bone marrow edema adjacent to erosions: The case specifically notes, "there was no significant surrounding bone marrow edema adjacent to these erosions," which helps differentiate chronic PVNS erosions from acute inflammatory or infectious erosions.
- B. Multiple intra-articular calcified loose bodies: This is characteristic of synovial chondromatosis, not PVNS. The MRI description for PVNS focuses on synovial proliferation and hemosiderin, not calcified bodies.
- D. Complete absence of joint effusion: The patient presented with a persistent, palpable joint effusion, and the MRI confirmed a "moderate to large joint effusion." An absence of effusion would contradict the clinical and imaging findings.
- E. High signal intensity on T1-weighted images within the synovium: While some hemorrhagic conditions can show high signal on T1 due to methemoglobin, the classic and pathognomonic finding for PVNS is low signal on both T1 and T2 due to chronic hemosiderin deposition, which has a paramagnetic effect.
Question 14
During a repeat diagnostic arthrocentesis, 45 cc of dark, opaque, reddish-brown fluid was aspirated from the patient's knee. The fluid was negative for crystals, and cultures were negative. Which classic description is often used to characterize the appearance of synovial fluid in Pigmented Villonodular Synovitis (PVNS)?
Explanation
Correct Answer: C - Resembling 'crankcase oil' or liquid chocolate
The case explicitly states that the aspirated fluid was "dark, opaque, reddish-brown fluid, often classically described as resembling 'crankcase oil' or liquid chocolate." This distinctive appearance is due to the chronic presence of blood and hemosiderin within the joint, a hallmark of PVNS.
- A. Clear, straw-colored: This describes normal synovial fluid or a non-inflammatory effusion, which is not consistent with the patient's presentation.
- B. Turbid, purulent: This is characteristic of septic arthritis, which was ruled out by negative cultures and Gram stain.
- D. Highly viscous, mucinous: This can be seen in conditions like synovial chondromatosis or early osteoarthritis, but not the dark, bloody fluid of PVNS.
- E. Cloudy, yellow with urate crystals: This is characteristic of gout, which was ruled out by crystal analysis.
Question 15
Histopathological evaluation is crucial for definitive diagnosis of Tenosynovial Giant Cell Tumor (TGCT), diffuse type (PVNS). Microscopically, PVNS is characterized by a hypercellular proliferation of mononuclear cells, multinucleated osteoclast-like giant cells, foamy lipid-laden macrophages, and extensive hemosiderin deposits. Beyond these cellular features, what is the specific genetic abnormality frequently associated with the pathogenesis of PVNS?
Explanation
Correct Answer: C - t(1;2)(p13;q37) translocation leading to CSF1 overexpression
The case explicitly details the pathogenesis: "The mononuclear cells frequently demonstrate a specific genetic translocation, t(1;2)(p13;q37), which results in the fusion of the Colony Stimulating Factor 1 (CSF1) gene with the Collagen Type VI Alpha 3 (COL6A3) promoter. This translocation leads to the localized overproduction of CSF1, which acts as a chemoattractant, recruiting the massive influx of non-neoplastic macrophages and giant cells that form the bulk of the tumor mass." This genetic abnormality and its consequence are central to understanding PVNS.
- A. Trisomy 21: This is associated with Down syndrome and is not related to PVNS.
- B. t(11;22) translocation (Ewing sarcoma): This is the characteristic translocation found in Ewing sarcoma, a malignant bone tumor, not PVNS.
- D. Deletion of the p53 tumor suppressor gene: While p53 mutations are common in many cancers, it is not the primary or specific genetic driver for PVNS.
- E. BRAF V600E mutation: This mutation is notably associated with melanoma, papillary thyroid cancer, and hairy cell leukemia, but not PVNS.
Question 16
Based on the MRI findings demonstrating diffuse, exuberant, hypertrophic synovitis involving all compartments of the knee joint, including the suprapatellar pouch, medial and lateral gutters, intercondylar notch, and posterior joint recesses, how is this patient's condition most accurately classified according to the World Health Organization (WHO) system, and what is its typical recurrence rate after surgical synovectomy?
Explanation
Correct Answer: B - Diffuse TGCT; high recurrence rate (20-50%)
The case clearly states: "Based on the MRI findings demonstrating involvement of the suprapatellar pouch, gutters, intercondylar notch, and posterior recesses, this patient presented with Diffuse TGCT of the knee." It further elaborates on the WHO classification: "Diffuse TGCT (formerly Diffuse PVNS): Involves the entire synovial lining of a joint, bursa, or tendon sheath. It is locally aggressive, infiltrative, and carries a notoriously high recurrence rate (ranging from 20% to 50% in the literature) even after extensive surgical synovectomy."
- A. Localized TGCT; low recurrence rate (<5%): Localized TGCT (formerly Giant Cell Tumor of Tendon Sheath) presents as a discrete nodule, typically in digits, and has a low recurrence rate after excision. This does not match the diffuse involvement described.
- C. Synovial Sarcoma; variable recurrence rate depending on grade: Synovial sarcoma is a rare, aggressive malignancy, distinct from PVNS. While it can occur in joints, its classification and prognosis are different.
- D. Osteochondroma; no recurrence after complete excision: Osteochondroma is a benign bone tumor, not a synovial lesion, and is not relevant to this case.
- E. Reactive Synovitis; recurrence dependent on underlying cause: Reactive synovitis is a general term for inflammation of the synovium. While PVNS involves synovial inflammation, it is a specific tumor-like condition, not merely reactive, and has a distinct recurrence profile.
Question 17
The natural history of untreated diffuse Tenosynovial Giant Cell Tumor (TGCT) is progressive joint destruction. The hyperplastic synovium acts as a space-occupying lesion and degrades articular cartilage. Given this, what is the primary goal of surgical management for diffuse TGCT of the knee?
Explanation
Correct Answer: C - To achieve complete eradication of the abnormal synovial tissue
The case explicitly states: "The primary goal of treatment is the complete eradication of the abnormal synovial tissue to relieve symptoms, halt joint destruction, and prevent recurrence." This is the fundamental principle behind synovectomy for PVNS.
- A. To achieve joint fusion (arthrodesis) to eliminate pain: Arthrodesis is a salvage procedure for end-stage arthritis or severe joint destruction, not the primary goal for PVNS, especially in a young patient with preserved joint space.
- B. To perform a diagnostic biopsy and then observe for spontaneous regression: PVNS does not spontaneously regress. While a biopsy may be performed for diagnostic ambiguity, observation is not a viable definitive strategy for diffuse TGCT due to its progressive nature.
- D. To replace the affected joint with a prosthetic implant: Total joint arthroplasty may be necessary in cases of severe, end-stage joint destruction secondary to PVNS, but it is not the primary goal of initial surgical management, which aims to preserve the native joint.
- E. To decompress the joint capsule to relieve effusion: While effusion relief is a temporary benefit, simply decompressing the capsule does not address the underlying proliferative synovial tissue, which is the source of the problem and will lead to recurrence of effusion and continued joint destruction.
Question 18
During the all-arthroscopic extensive anterior and posterior synovectomy for this patient's diffuse TGCT of the knee, a critical technical challenge is ensuring thorough clearance of the posterior compartments. Which of the following best describes the arthroscopic approach to address the posterior compartments while minimizing neurovascular risk?
Explanation
Correct Answer: C - Establish posteromedial and posterolateral portals under direct intra-articular visualization, carefully avoiding neurovascular structures.
The case emphasizes: "Thorough clearance of the posterior compartments is the most critical step in preventing recurrence in diffuse TGCT. Trans-notch visualization is insufficient for a complete posterior synovectomy." It then describes the technique: "An 18-gauge spinal needle was used to localize a posteromedial portal under direct intra-articular visualization, ensuring it was superior to the joint line and posterior to the medial collateral ligament to avoid the saphenous nerve and vein. ... Similarly, a posterolateral portal was established under direct visualization, taking extreme care to stay anterior to the biceps femoris tendon and fibular head to protect the common peroneal nerve." This highlights the importance of direct visualization and careful portal placement.
- A. Rely solely on trans-notch visualization from anterior portals for posterior clearance: The case explicitly states this is "insufficient for a complete posterior synovectomy," leading to higher recurrence rates.
- B. Perform an open posterior approach as the primary method for all posterior disease: While an open posterior approach is an option, the case states that an all-arthroscopic approach was chosen because "there was no extra-articular extension... that would mandate an open posterior approach." Modern arthroscopic techniques allow for thorough posterior clearance without the morbidity of an open approach in many cases.
- D. Utilize a posterior midline portal to access both posteromedial and posterolateral compartments simultaneously: A posterior midline portal is not a standard or safe approach for comprehensive posterior knee arthroscopy due to the risk to the popliteal neurovascular bundle. Separate posteromedial and posterolateral portals are used.
- E. Perform a complete posterior capsulectomy through a single large posterior incision: This describes an open posterior approach, which was not the chosen method for this patient and is associated with higher morbidity and arthrofibrosis compared to arthroscopy.
Question 19
Despite meticulous surgical synovectomy, the recurrence rate for diffuse TGCT remains high. For patients with symptomatic TGCT associated with severe morbidity or functional limitations, and not amenable to improvement with surgery, a targeted systemic therapy has emerged. Which of the following agents is FDA-approved for this indication, and what is its primary mechanism of action?
Explanation
Correct Answer: B - Pexidartinib; selective Tyrosine Kinase Inhibitor (TKI) targeting the CSF1 receptor
The case specifically mentions: "Targeted Systemic Therapy (Pexidartinib): A relatively recent breakthrough. Pexidartinib is a selective Tyrosine Kinase Inhibitor (TKI) that targets the CSF1 receptor. By blocking the CSF1 receptor on the recruited macrophages, it effectively starves the tumor of its cellular bulk. It is FDA-approved for adults with symptomatic TGCT associated with severe morbidity or functional limitations, and not amenable to improvement with surgery."
- A. Methotrexate; inhibits dihydrofolate reductase: Methotrexate is a disease-modifying antirheumatic drug (DMARD) used in inflammatory arthritides like RA, not specifically for PVNS.
- C. Adalimumab; TNF-alpha inhibitor: Adalimumab is a biologic DMARD used for inflammatory conditions like RA, psoriatic arthritis, and ankylosing spondylitis, not PVNS.
- D. Rituximab; CD20 monoclonal antibody: Rituximab targets B cells and is used in lymphomas and certain autoimmune diseases, not PVNS.
- E. Ibuprofen; non-selective COX inhibitor: Ibuprofen is an NSAID, providing symptomatic relief but not addressing the underlying pathology or recurrence of PVNS.
Question 20
A 38-year-old male with diffuse Tenosynovial Giant Cell Tumor (TGCT) of the knee, as described in the case, opts against surgical intervention due to personal reasons. If left untreated, what is the most likely long-term outcome for this patient's knee joint?
Explanation
Correct Answer: C - Progressive joint destruction leading to severe secondary osteoarthritis, often requiring total joint arthroplasty.
The case explicitly states the natural history of untreated diffuse TGCT: "The natural history of untreated diffuse TGCT is progressive joint destruction. The hyperplastic synovium acts as a space-occupying lesion, causing mechanical damage, while the biochemical environment (metalloproteinases and inflammatory cytokines) degrades articular cartilage. The subchondral erosions eventually lead to structural collapse and severe secondary osteoarthritis, often necessitating premature total joint arthroplasty in young patients."
- A. Spontaneous regression of the synovial proliferation and resolution of symptoms: PVNS is a locally aggressive, tumor-like condition that does not spontaneously regress.
- B. Development of a malignant transformation into synovial sarcoma: While PVNS is a tumor-like condition, malignant transformation into synovial sarcoma is exceedingly rare and not considered the typical natural history.
- D. Chronic, stable effusion with minimal impact on joint function: The disease is progressive, leading to increasing pain, mechanical symptoms, and functional limitations, not a stable state.
- E. Resolution of mechanical symptoms but persistence of pain and swelling: Mechanical symptoms (catching, giving way, mechanical block) are a prominent feature of PVNS due to the space-occupying nature of the synovium and would worsen, not resolve, without treatment.
Question 21
A 25-year-old male undergoes an open Latarjet procedure for recurrent anterior shoulder instability with 25% glenoid bone loss. Postoperatively, he complains of numbness over the lateral aspect of his forearm, but motor function of the biceps is intact. Which nerve is most likely injured, and what is its typical distance from the coracoid tip where it enters the conjoint tendon?
Explanation
Question 22
A 35-year-old female presents with recurrent, spontaneous hemorrhagic effusions of her right knee. MRI reveals nodular synovial thickening with low signal intensity on both T1- and T2-weighted images, along with significant "blooming" artifact on gradient-echo sequences. What is the most likely diagnosis?
Explanation
Question 23
During preoperative planning for an anterior shoulder stabilization, the concept of the "glenoid track" is utilized to evaluate bipolar bone loss. A Hill-Sachs lesion is considered "off-track" if its medial margin extends medial to what specific landmark or measurement?
Explanation
Question 24
A biopsy of hypertrophic synovium from a knee with recurrent atraumatic effusions reveals mononuclear stromal cells, multinucleated giant cells, and hemosiderin-laden macrophages. Which of the following genetic translocations is established in the pathogenesis of this condition?
Explanation
Question 25
A 40-year-old male sustains a seizure and is found to have a locked posterior shoulder dislocation. CT imaging reveals a reverse Hill-Sachs lesion (anteromedial humeral head defect) involving 35% of the articular surface. The glenoid is intact. What is the most appropriate surgical management?
Explanation
Question 26
A 30-year-old male is diagnosed with diffuse, severe pigmented villonodular synovitis (PVNS) of the knee that has recurred after multiple open synovectomies. He is deemed a candidate for targeted systemic therapy. Which FDA-approved medication, acting as a CSF1R inhibitor, is indicated for this condition?
Explanation
Question 27
During arthroscopic stabilization for recurrent anterior shoulder instability, the surgeon identifies an ALPSA lesion. Which of the following best describes the anatomic pathomorphology of this specific lesion?
Explanation
Question 28
Tenosynovial Giant Cell Tumor (diffuse type, historically known as PVNS) most frequently affects which of the following anatomic locations?
Explanation
Question 29
A surgeon plans an arthroscopic Bankart repair with Remplissage for a patient with 10% anterior glenoid bone loss and an "off-track" Hill-Sachs lesion. Which structure is tenodesed into the humeral head defect during the Remplissage portion of the procedure?
Explanation
Question 30
A 28-year-old female presents with a chronic, mildly painful, swollen knee without any history of preceding trauma. Aspiration of the joint yields a thick, dark brown, "chocolate-like" fluid that does not clear with sequential aspiration. Which of the following is the most likely diagnosis?
Explanation
Question 31
A 19-year-old gymnast complains of bilateral shoulder pain and a sensation that her shoulders are "slipping out of place." Physical examination demonstrates generalized ligamentous laxity, a positive sulcus sign of 2.5 cm bilaterally, and apprehension with anterior and posterior translation. What is the most appropriate initial management?
Explanation
Question 32
When comparing the localized and diffuse forms of Pigmented Villonodular Synovitis (PVNS) regarding surgical outcomes, which of the following statements is most accurate?
Explanation
Question 33
A patient with a history of recurrent anterior shoulder instability undergoes an MR arthrogram. The radiologist notes a "U-shaped" dependent pouch of the axillary recess and extravasation of contrast into the soft tissues inferior to the glenohumeral joint. Which lesion does this specific finding describe?
Explanation
Question 34
A 24-year-old athlete with recurrent anterior shoulder instability undergoes an arthroscopic Bankart repair. Preoperative imaging demonstrated 10% glenoid bone loss and an 'off-track' Hill-Sachs lesion. Which of the following is the most appropriate concurrent procedure?
Explanation
Question 35
A 35-year-old female presents with chronic knee swelling and pain. MRI reveals a nodular synovial mass with low signal intensity on T1 and T2-weighted sequences, displaying blooming artifact on gradient-echo images. Biopsy is performed. Which of the following histologic findings is characteristic of this condition?
Explanation
Question 36
A 45-year-old male presents to the emergency department after a seizure. He complains of right shoulder pain and an inability to rotate the arm externally. Radiographs show a 'lightbulb' sign on the AP view. What is the most likely associated osseous defect?
Explanation
Question 37
A 29-year-old male has recurrent, diffuse Pigmented Villonodular Synovitis (PVNS) of the knee despite multiple arthroscopic synovectomies. His oncologist recommends targeted systemic therapy. Which of the following pathways is the primary target of this pharmacologic treatment?
Explanation
Question 38
A 22-year-old rugby player undergoes an open Latarjet procedure for recurrent anterior instability with 25% glenoid bone loss. Postoperatively, he exhibits weakness in elbow flexion and decreased sensation over the lateral aspect of his forearm. Which nerve was most likely injured during the procedure?
Explanation
Question 39
The pathogenesis of localized and diffuse tenosynovial giant cell tumor (formerly PVNS) is most strongly associated with which of the following cytogenetic abnormalities?
Explanation
Question 40
A 38-year-old male suffers a posterior shoulder dislocation. Imaging reveals an anteromedial humeral head defect comprising 30% of the articular surface. Which of the following surgical interventions is most appropriate?
Explanation
Question 41
An 18-year-old male sustains a shoulder dislocation and subsequent recurrent instability. An MR arthrogram demonstrates extravasation of contrast into the axilla with a normal-appearing anterior labrum. What is the most likely diagnosis?
Explanation
Question 42
While Pigmented Villonodular Synovitis (PVNS) most commonly affects the knee, when it presents in the shoulder, it can often be mistaken for which of the following conditions due to its characteristic erosive nature on radiographs?
Explanation
Question 43
A 16-year-old female swimmer presents with bilateral shoulder pain and a sensation of her shoulders 'slipping out' during her stroke. Physical exam shows a positive sulcus sign and generalized ligamentous laxity. After a 6-month trial of directed physical therapy, she remains highly symptomatic. Which surgical procedure is most indicated?
Explanation
Question 44
Following an arthroscopic synovectomy for diffuse Pigmented Villonodular Synovitis (PVNS) of the knee, a 40-year-old patient asks about the likelihood of disease recurrence. What is the approximate expected recurrence rate for the diffuse form of PVNS treated with synovectomy alone?
Explanation
Question 45
During an arthroscopic stabilization for anterior shoulder instability, the surgeon notes that the anterior labroligamentous complex is avulsed from the glenoid and has healed medially on the anterior neck of the scapula with an intact periosteal sleeve. This finding is best described as which of the following?
Explanation
Question 46
A 31-year-old male is treated for an acute, first-time posterior shoulder dislocation. Following closed reduction, which immobilization position is most biomechanically favorable to promote healing of the posterior capsulolabral structures?
Explanation
Question 47
A 44-year-old man presents with chronic unilateral hip pain and decreased range of motion. Radiographs show periarticular erosions on both sides of the joint. MRI shows a joint effusion with nodular synovial masses. Which MRI sequence is most sensitive for confirming the diagnosis of PVNS?
Explanation
Question 48
A 19-year-old male recreational basketball player undergoes an arthroscopic Bankart repair for recurrent anterior shoulder instability. Which of the following factors is associated with the highest risk of recurrent instability following this procedure?
Explanation
Question 49
A 50-year-old female undergoes knee arthroscopy for catching and mechanical symptoms. A 2 cm pedunculated yellowish-brown mass is found attached to the infrapatellar fat pad and is completely excised. The rest of the synovium is normal. What is the most likely diagnosis and appropriate follow-up?
Explanation
Question 50
The 'glenoid track' is a critical concept in evaluating shoulder instability. How is the width of the normal glenoid track calculated relative to the uninjured glenoid width (D)?
Explanation
Question 51
A 22-year-old overhead athlete presents with recurrent anterior shoulder instability. A 3D CT scan is ordered to evaluate for glenoid bone loss. The concept of the 'glenoid track' is utilized to determine if a Hill-Sachs lesion will engage the anterior glenoid rim. Which of the following formulas correctly calculates the width of the glenoid track?
Explanation
Question 52
A 26-year-old male is scheduled for a Latarjet procedure due to a 20% anterior glenoid bone defect. During the procedure, the coracoid is osteotomized and transferred to the anterior glenoid. The 'sling effect' contributes significantly to the stability provided by this procedure. This dynamic effect is primarily created by the conjoint tendon compressing against which structure?
Explanation
Question 53
A 35-year-old female presents with a spontaneous, recurrent, painless hemarthrosis of the right knee. Magnetic resonance imaging (MRI) reveals a large, lobulated intra-articular mass. Which MRI sequence is most sensitive for identifying the characteristic 'blooming artifact' associated with this condition?
Explanation
Question 54
Which of the following genetic alterations is considered the primary molecular driver in the pathogenesis of tenosynovial giant cell tumor (TGCT/PVNS)?
Explanation
Question 55
A 40-year-old male sustains a seizure and subsequently complains of severe left shoulder pain with restricted external rotation. An AP radiograph of the shoulder shows a symmetric appearance of the humeral head with a loss of the normal half-moon overlap of the humeral head and glenoid. What is the classic radiologic descriptor for this finding?
Explanation
Question 56
During arthroscopic evaluation of a patient with recurrent anterior shoulder instability, an anterior labroligamentous periosteal sleeve avulsion (ALPSA) lesion is identified. How does this primarily differ pathoanatomically from a classic Bankart lesion?
Explanation
Question 57
A 19-year-old collegiate wrestler suffers a first-time traumatic anterior shoulder dislocation. After successful closed reduction, what single factor places this patient at the highest statistical risk for recurrent instability if managed non-operatively?
Explanation
Question 58
A patient is undergoing an open Latarjet procedure. To safely dissect and mobilize the coracoid process, the surgeon must be mindful of the musculocutaneous nerve. On average, how far distal to the tip of the coracoid process does the musculocutaneous nerve enter the conjoint tendon?
Explanation
Question 59
In cases of critical glenoid bone loss with an off-track Hill-Sachs lesion, a remplissage procedure is often performed concurrently with a Bankart repair. What does the arthroscopic remplissage technique specifically involve?
Explanation
Question 60
A 28-year-old athlete undergoes a Latarjet procedure for recurrent anterior instability. Postoperatively, radiographs reveal that the coracoid graft was positioned too laterally, overhanging the articular surface of the glenoid. What is the most likely long-term complication of this technical error?
Explanation
Question 61
A 45-year-old patient with recalcitrant diffuse tenosynovial giant cell tumor (TGCT/PVNS) of the knee is deemed unresectable and is started on pexidartinib. Which of the following represents the FDA black box warning associated with this medication?
Explanation
Question 62
During physical examination of a 20-year-old female gymnast with multidirectional shoulder instability (MDI), a 'sulcus sign' is elicited in neutral rotation and adduction. Which primary capsuloligamentous structures are being evaluated with this specific test?
Explanation
Question 63
A 32-year-old male sustains a posterior shoulder dislocation complicated by a reverse Hill-Sachs lesion that involves 30% of the articular surface. Which of the following procedures (McLaughlin procedure) was traditionally described for managing this specific bony defect?
Explanation
Question 64
Histological evaluation of a biopsy specimen taken from an inflamed knee joint reveals a proliferation of mononuclear cells, multi-nucleated giant cells, and numerous foamy macrophages laden with brown pigment. What is the composition of the characteristic brown pigment found in this condition?
Explanation
Question 65
A 23-year-old rugby player has recurrent shoulder instability. Magnetic Resonance Imaging reveals a torn anterior glenohumeral ligament that has avulsed directly from the humeral neck, with an associated loss of the normal U-shaped axillary pouch. What is the proper acronym for this lesion?
Explanation
Question 66
A 29-year-old male with recurrent anterior shoulder dislocations is undergoing a 3D CT scan to evaluate for bipolar bone loss. Based on current literature, a Hill-Sachs lesion is most likely to 'engage' the anterior glenoid rim during which specific arm position?
Explanation
Question 67
Which of the following descriptions best distinguishes localized tenosynovial giant cell tumor (L-TGCT) from diffuse tenosynovial giant cell tumor (D-TGCT/PVNS)?
Explanation
Question 68
During a Latarjet procedure, an osteotomy of the coracoid process is performed. To maximize the bone block size while avoiding detachment of the coracoclavicular ligaments, the osteotomy should be made exactly at what anatomical landmark?
Explanation
Question 69
A 25-year-old athlete undergoes an MRI arthrogram for chronic shoulder pain following a mild subluxation event. The scan reveals a superficial anterior-inferior labral tear associated with adjacent articular cartilage damage on the glenoid, but the anterior band of the IGHL is intact. What is the diagnosis?
Explanation
Question 70
A 45-year-old patient presents with monoarticular knee swelling, stiffness, and brown-colored joint aspirate. Plain radiographs are ordered. What is the most characteristic radiographic finding in the later stages of Pigmented Villonodular Synovitis (PVNS)?
Explanation
Question 71
A 34-year-old male presents with locked posterior shoulder dislocation after a seizure. CT reveals a reverse Hill-Sachs lesion involving 30% of the anterior humeral head articular surface. Which of the following is the most appropriate surgical management?
Explanation
Question 72
A 29-year-old female presents with chronic shoulder pain, swelling, and mechanical catching. MRI demonstrates a lobulated intra-articular mass with a 'blooming' artifact. Which of the following MRI sequences best highlights this specific artifact?
Explanation
Question 73
During diagnostic arthroscopy for recurrent anterior shoulder instability, the surgeon identifies an anterior labral tear. The anterior scapular periosteum is intact, but the labrum and inferior glenohumeral ligament have healed medially on the anterior glenoid neck.
What is the classic eponym for this lesion?
Explanation
Question 74
A patient with refractory diffuse tenosynovial giant cell tumor (PVNS) of the shoulder is prescribed pexidartinib. Which of the following severe adverse effects requires strict monitoring through a Risk Evaluation and Mitigation Strategy (REMS) program?
Explanation
Question 75
A 22-year-old overhead athlete undergoes an arthroscopic Bankart repair with a concurrent remplissage procedure. Which of the following kinematic changes is most likely to result from the addition of the remplissage?
Explanation
Question 76
Which of the following best describes the pathogenesis of tenosynovial giant cell tumor (PVNS)?
Explanation
Question 77
A 24-year-old rugby player has recurrent shoulder instability. 3D CT reconstructions are analyzed to determine the 'Glenoid Track'.
How is the width of the intact glenoid track calculated?
Explanation
Question 78
During an open Latarjet procedure, the coracoid process is osteotomized and transferred to the anterior glenoid. To minimize the risk of injury to the musculocutaneous nerve, the surgeon must be aware of its anatomical relationship. At approximately what distance distal to the tip of the coracoid process does the musculocutaneous nerve typically enter the coracobrachialis muscle?
Explanation
Question 79
A 30-year-old male sustains a severe shoulder dislocation. MRI arthrogram demonstrates extravasation of contrast into the axillary pouch with an intact anterior labrum. A 'J-sign' is noted on the coronal sequences.
What is the most likely diagnosis?
Explanation
Question 80
A 17-year-old male suffers his first anterior shoulder dislocation while playing hockey. Following closed reduction, the patient and his parents ask about the risk of recurrence if treated non-operatively. Which of the following is the single greatest risk factor for recurrent instability in this patient?
Explanation
Question 81
A 45-year-old female is diagnosed with localized tenosynovial giant cell tumor (PVNS) of the shoulder. Plain radiographs are obtained. Which of the following radiographic findings is most characteristic of this disease process?
Explanation
Question 82
A 19-year-old gymnast is diagnosed with multidirectional instability (MDI) of the shoulder. She has failed 6 months of targeted physical therapy.
If surgical intervention is pursued, an arthroscopic capsular shift is performed. Closure of the rotator interval during this procedure primarily limits which motion?
Explanation
Question 83
During a Latarjet procedure, the subscapularis muscle can be managed either by a split in line with its fibers or by a tenotomy. Proponents of the subscapularis split argue it provides which specific anatomical and functional advantage?
Explanation
Question 84
Recent literature regarding anterior shoulder instability highlights the concept of 'subcritical' bone loss, where soft-tissue stabilization alone may result in poorer clinical outcomes in high-demand patients. What percentage of anterior glenoid bone loss is most commonly defined as the threshold for subcritical bone loss?
Explanation
Question 85
A 22-year-old football player presents with a posterior labral tear and posterior instability.
During physical examination, which of the following tests is most specific for diagnosing a symptomatic posterior labral tear or recurrent posterior subluxation?
Explanation
Question 86
A 28-year-old male with recurrent anterior shoulder instability and 30% glenoid bone loss underwent a Latarjet procedure 2 years ago. He now presents with a failed Latarjet, hardware loosening, and recurrent dislocations. A salvage procedure is planned. Which of the following describes an Eden-Hybinette procedure?
Explanation
Question 87
A 40-year-old male undergoes arthroscopic synovectomy for localized PVNS of the shoulder. Histopathological analysis of the resected tissue is performed. Which of the following cellular components is the actual neoplastic cell driving the disease?
Explanation
Question 88
In the evaluation of anterior shoulder instability, a Hill-Sachs lesion is considered 'engaging' if its long axis is parallel to the anterior glenoid rim when the arm is in which of the following positions?
Explanation
Question 89
A patient presents with an atraumatic, swollen, and painful shoulder. Aspiration of the joint is performed to rule out infection. The fluid aspirated is dark brown and opaque ('chocolate fluid'). Cultures are negative. What is the most likely diagnosis?
Explanation
Question 90
A 55-year-old male sustains an acute anterior shoulder dislocation. Following closed reduction, he has profound weakness in external rotation and a positive Hornblower's sign, but imaging shows no rotator cuff tear. Which of the following concomitant injuries most likely explains these specific physical exam findings?
Explanation
None
