Distal Radius Fractures: Comprehensive Classification, Stability Assessment, and Operative Management

Key Takeaway
Distal radius fractures demand meticulous assessment of stability and articular congruity. While stable patterns may be managed with closed reduction and casting, unstable fractures—defined by LaFontaine’s criteria—often necessitate operative intervention. Treatment strategies range from percutaneous pinning to rigid internal fixation, tailored to patient demand, bone quality, and fracture morphology to optimize functional recovery and minimize post-traumatic arthrosis.
INTRODUCTION TO DISTAL RADIUS FRACTURES
Distal radius fractures represent one of the most ubiquitous injuries encountered in orthopedic traumatology, accounting for approximately one-sixth of all fractures treated in emergency departments. The management of these fractures has evolved significantly, transitioning from historical reliance on closed reduction and cast immobilization to a nuanced, evidence-based approach that heavily incorporates operative intervention for unstable patterns.
The primary goal of treatment is the restoration of normal wrist anatomy—specifically radial height, volar tilt, radial inclination, and articular congruity—to maximize functional outcomes and mitigate the risk of post-traumatic osteoarthritis. Achieving this requires a profound understanding of fracture morphology, biomechanical stability, and patient-specific physiological demands.
CLASSIFICATION SYSTEMS
More than 20 classification systems have been proposed for distal radial fractures. As with most fracture classifications, the intraobserver and interobserver agreement rates usually are only moderate at best. However, these classifications are indispensable for understanding fracture pathoanatomy, facilitating academic communication, and conceptualizing the biomechanical challenges inherent in treatment.
Gartland and Werley Classification (1951)
This foundational system emphasizes metaphyseal comminution, intra-articular extension, and fragment displacement. It is primarily descriptive and serves as a historical baseline for understanding fracture severity.
* Group 1: Simple Colles fracture (extra-articular, non-comminuted).
* Group 2: Comminuted Colles fracture, undisplaced intra-articular fragment.
* Group 3: Comminuted Colles fracture, displaced intra-articular fragment.
Frykman Classification (1967)
Frykman advanced the assessment by incorporating the involvement of the radioulnar and radiocarpal joints, as well as the presence of an ulnar styloid fracture. A key mnemonic for this system is that even numbers indicate an associated ulnar styloid fracture.
* Group 1 / 2: Extra-articular (without / with ulnar styloid fracture).
* Group 3 / 4: Intra-articular involving the radiocarpal joint (without / with ulnar styloid fracture).
* Group 5 / 6: Intra-articular involving the distal radioulnar joint (DRUJ) (without / with ulnar styloid fracture).
* Group 7 / 8: Intra-articular involving both radiocarpal and DRUJ (without / with ulnar styloid fracture).
Melone Classification (1986)
Melone evaluated the four major fracture components: the radial shaft, the radial styloid, the dorsal medial fragment, and the volar medial fragment. This system is highly relevant for understanding "die-punch" injuries and the critical importance of the lunate facet.
* Type 1: Undisplaced, minimal comminution, stable.
* Type 2: Unstable, displacement of the medial complex, moderate-to-severe comminution.
* Type 3: Displacement of the medial complex as a unit plus an anterior spike.
* Type 4: Wide separation or rotation of the dorsal fragment and palmar fragment rotation.
Fernandez Classification (1987)
Fernandez revolutionized treatment algorithms by basing his classification system on the mechanism of injury. This system directly guides the choice of surgical fixation.
* Type 1 (Bending): One cortex of the metaphysis fails due to tensile stress; opposite cortex with some comminution (e.g., classic Colles or Smith fractures).
* Type 2 (Shearing): Fracture of the joint surface (e.g., Barton or reverse Barton fractures). Requires buttress plate fixation.
* Type 3 (Compression): Fracture of the joint surface with impaction of subchondral and metaphyseal bone, intra-articular comminution (die-punch). Requires bone grafting and support.
* Type 4 (Avulsion): Fracture of the ligament attachments of the ulnar and radial styloid process, radiocarpal fracture-dislocation (e.g., Chauffeur's fracture).
* Type 5 (Combination): High-velocity injuries combining multiple mechanisms.
Cooney Universal Classification (1990)
- Type 1: Extra-articular, undisplaced.
- Type 2: Extra-articular, displaced.
- Type 3: Intra-articular, undisplaced.
- Type 4: Intra-articular, displaced.
Modified AO/OTA Classification
The AO system remains the gold standard for academic research, categorizing fractures based on articular involvement.
* Type A: Extra-articular.
* Type B: Partial articular (B1: radial styloid, B2: dorsal rim, B3: volar rim, B4: die-punch).
* Type C: Complete articular (metaphyseal dissociation from the diaphysis).
ASSESSMENT OF STABILITY
Most distal radial fractures are initially treated with immobilization after closed reduction. Unfortunately, many of these fractures lose reduction, or the initial reduction is deemed unacceptable upon critical radiographic review, leading to poor functional outcomes. Identifying fractures at high risk for displacement is paramount.
The LaFontaine Criteria
LaFontaine et al. identified five critical factors indicative of inherent fracture instability. The presence of three or more of these factors strongly predicts the failure of conservative management:
1. Initial dorsal angulation of more than 20 degrees (severe loss of volar tilt).
2. Dorsal metaphyseal comminution.
3. Intra-articular involvement.
4. An associated ulnar fracture (ulnar styloid or neck).
5. Patient age older than 60 years (a surrogate for osteopenia/osteoporosis).
Clinical Pearl: Other suggested indicators of instability include initial radial shortening of greater than 5 mm and significant volar comminution. A fracture that requires excessive molding or extreme wrist flexion (Cotton-Loder position) to maintain reduction is inherently unstable and should be considered for operative fixation.
There are no definitive, universally agreed-upon criteria to dictate treatment decision-making in borderline cases. A multitude of factors must be considered when developing a treatment plan, including:
* Initial injury characteristics and energy of trauma.
* Anatomical alignment achieved after closed reduction.
* Patient age and systemic bone quality.
* Patient functional demand and occupation.
* Expected functional outcome versus surgical risk.
If closed treatment is chosen for a fracture with questionable stability, meticulous and close monitoring is advised. It is imperative to note any change in the reduction over a series of weekly radiographs. Fractures considered potentially unstable must be evaluated with serial radiographs (typically at 1, 2, and 3 weeks post-injury) until early fracture callus provides mechanical stability.
ASSOCIATED ULNAR INJURIES: GALEAZZI AND ULNAR STYLOID FRACTURES
Distal radius fractures rarely occur in isolation. The distal radioulnar joint (DRUJ) and the ulnar styloid are frequently compromised, significantly altering the stability of the forearm axis.
Galeazzi Fracture-Dislocations
A Galeazzi injury involves a fracture of the distal third of the radial shaft coupled with a dislocation or subluxation of the DRUJ. These are highly unstable injuries that mandate operative intervention in adults.

The radius must be anatomically reduced and rigidly fixed, typically utilizing a dynamic compression plate (DCP) or a locking compression plate (LCP). Following radial fixation, the DRUJ must be assessed for stability throughout the forearm arc of motion. If the DRUJ remains unstable, it is often pinned in supination using parallel Kirschner wires.


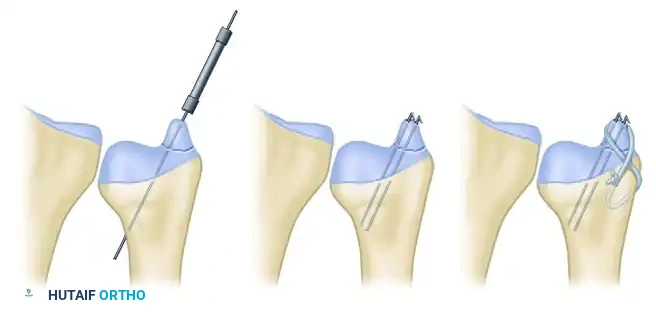
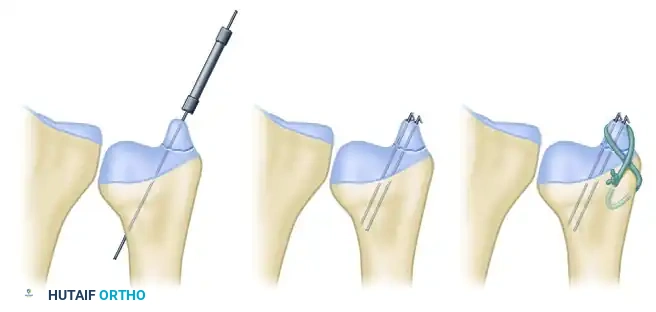
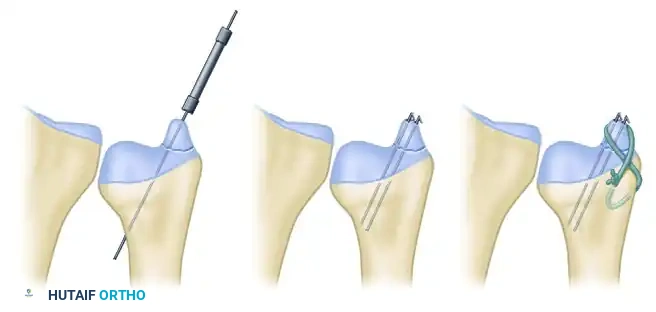
Ulnar Styloid Fractures
Ulnar styloid fractures occur in up to 60% of distal radius fractures. Base of styloid fractures are particularly concerning as they often represent an avulsion of the primary stabilizing components of the Triangular Fibrocartilage Complex (TFCC).
If the DRUJ is unstable following fixation of the radius, the ulnar styloid should be addressed. Open reduction and internal fixation (ORIF) can be achieved via several techniques depending on fragment size:
* Lag Screw Fixation: Ideal for large, non-comminuted base fragments.
* Kirschner Wire Pinning: Useful for smaller fragments.
* Tension Band Wiring: Provides excellent biomechanical compression for transverse avulsion fractures.
TREATMENT OPTIONS
Closed Treatment and Immobilization
Stable fractures can be successfully treated with closed reduction and immobilization. The standard protocol involves initial stabilization with a well-padded sugar-tong splint to accommodate acute swelling, followed by conversion to a short-arm or long-arm cast once edema subsides.
Monitoring Protocol:
Weekly radiographic evaluation is mandatory for the first 3 weeks. Significant changes in radial length (shortening >3mm), palmar tilt (dorsal angulation >10 degrees from neutral), or loss of radial inclination should prompt immediate consideration of operative treatment.
The Elderly and Low-Demand Patient:
In infirm and low-demand patients, closed treatment is often appropriate even in the presence of factors that would constitute absolute indications for operative treatment in younger, more active cohorts.
Evidence-Based Rationale: In a prospective randomized trial comparing nonoperative treatment with volar locking plate fixation in 73 patients aged 65 years or older, Arora et al. found no significant differences in range of motion or level of pain at the 1-year follow-up. Although grip strength was objectively better in the operatively treated group, anatomical reconstruction did not improve the patients’ subjective ability to perform activities of daily living (ADLs).
Similarly, Egol et al. demonstrated that minor limitations in wrist range of motion and diminished grip strength following nonoperative treatment did not limit functional recovery in a cohort of 90 patients older than 65 years. These findings are strongly corroborated by Diaz-Garcia et al., whose systematic review suggested that despite worse radiographic outcomes (malunion) after cast treatment in the elderly, functional outcomes (DASH scores) are statistically indistinguishable from those of operatively treated patients 60 years and older.
Percutaneous Pinning
Percutaneous pinning after closed reduction is a highly effective, minimally invasive technique useful for distal radial fractures exhibiting metaphyseal instability or simpler intra-articular displacement (e.g., 2-part sagittal splits).
Biomechanical Principles:
An anatomical reduction must be obtained first via closed manipulation (traction, palmar translation, and ulnar deviation). Kirschner wires (K-wires) do not reduce the fracture; they merely maintain the reduction by acting as internal splints.
Surgical Technique:
1. Positioning: The patient is positioned supine with the arm extended on a radiolucent hand table. Fluoroscopy is positioned parallel to the table.
2. Reduction: Longitudinal traction is applied, often utilizing finger traps. The fracture is disimpacted and reduced.
3. Styloid Pinning: The first pins (usually 1.6 mm / 0.062-inch K-wires) are placed percutaneously from the tip of the radial styloid, directed proximally and ulnarly across the fracture site into the intact medial radial metaphysis and diaphysis.
* Surgical Warning: The superficial branch of the radial nerve (SBRN) is highly vulnerable during radial styloid pin insertion. A mini-open technique—utilizing a small incision and blunt dissection down to the bone with a hemostat—is strongly recommended to protect the nerve and extensor tendons.
4. Lunate Facet Pinning: If the lunate facet is displaced, a separate pin can be driven from the dorso-ulnar aspect of the distal radius fragment into the proximal radial shaft.
5. Kapandji (Intrafocal) Technique: Intrafocal pins can be added to provide a direct dorsal buttress. A K-wire is introduced directly into the fracture hematoma dorsally, levered to reduce dorsal tilt, and driven into the intact volar cortex.
Postoperative Protocol:
We generally use at least two to three pins and confirm adequate reduction on true anteroposterior and lateral fluoroscopic views. Splint or cast immobilization is strictly necessary after percutaneous pinning, as the pins alone cannot withstand physiological loads. Pins are typically removed in the clinic at 4 to 6 weeks postoperatively once clinical and radiographic union is evident.
Outcomes and Complications:
A number of studies have reported excellent success with this technique. Glickel et al. reported good long-term outcomes with closed reduction and percutaneous pinning of all but the most complex, highly comminuted injuries. Percutaneous pinning tends to work best when pins are anchored in dense subchondral bone, making it less ideal for severely osteoporotic patients.
Complications related to the technique of percutaneous pinning include:
* Tendon Tethering or Rupture: Particularly the Extensor Pollicis Longus (EPL) if dorsal pins are left prominent.
* Pin Migration: Backing out of pins leading to loss of reduction.
* Nerve Injury: Iatrogenic damage to the SBRN.
* Infection: Superficial pin tract infections occur in up to 10% of cases, usually resolving with oral antibiotics and pin removal. Deep infections are rare but require immediate surgical debridement.
You Might Also Like
