Open Hip Dislocation: How Fascia Lata Autograft Restores Stability

Key Takeaway
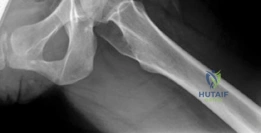
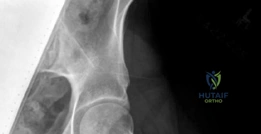
We review everything you need to understand about Open Hip Dislocation: How Fascia Lata Autograft Restores Stability. A 25-year-old female with left hip posterior femoroacetabular impingement received treatment via surgical hip dislocation. The procedure involved posterior wall rim trimming and labral reconstruction using a fascia lata autograft. This intervention successfully addressed chronic posterior hip pain and associated labral pathology stemming from a prominent posterior acetabular wall.
A 32-year-old active female presents with a six-month history of painful, recurrent "clicking" and a sensation of the right hip "giving way." She underwent hip arthroscopy for femoroacetabular impingement 18 months ago. Examination reveals a positive apprehension test in extension and external rotation. An MRA is provided below.
How do you approach this patient, and what is the likely diagnosis?
Candidate: The patient has post-arthroscopic iatrogenic hip instability. I would confirm this with clinical exam and MRA. I'd start with physical therapy focusing on dynamic stabilizers. If that fails, I would consider an open capsular reconstruction using a fascia lata graft.
Focusing only on the "hole" in the capsule. Failing to mention a mandatory assessment of bony morphology (e.g., version, dysplasia) and assuming the patient is immediately a candidate for surgery without a trial of specialized physiotherapy.
A structured approach: 1) Clinical history confirming mechanical symptoms and failed previous intervention. 2) Systematic imaging evaluation: MRI to quantify the capsular defect and CT for osseous morphology (version/dysplasia) to rule out bony causes of instability. 3) Initial management: Dedicated hip-stabilization physiotherapy. 4) Surgical indication: If conservative management fails, I would propose an open surgical hip dislocation and capsular reconstruction using an iliotibial band autograft, ensuring that any underlying bony mal-orientation is corrected simultaneously.
Describe the "Ganz Principle" in the context of the surgical approach for this patient. Why is this technique considered safe for the femoral head?
Candidate: The Ganz technique involves a trochanteric flip osteotomy. It protects the medial circumflex femoral artery (MCFA) by keeping it within the vascular sleeve of the short external rotators, allowing 360-degree joint access without AVN risk.
Vague explanations of "not cutting the blood vessels" without specifying the anatomy. Failing to mention the specific role of the digastric osteotomy in preserving the superior retinacular vessels derived from the MCFA.
The core of the Ganz approach is the preservation of the deep branch of the medial circumflex femoral artery (MCFA). By performing a digastric trochanteric flip osteotomy—maintaining the attachment of the external rotators and the posterior soft tissue envelope—the blood supply to the femoral head remains tethered via the superior retinaculum. This allows for safe anterior dislocation and full exposure of the acetabulum and femoral neck without risking avascular necrosis.
You have harvested the fascia lata. Describe the biomechanical rationale for using this tissue and the critical intraoperative steps for tensioning the graft.

Candidate: The ITB is strong and mimics the native iliofemoral ligament. I fix it to the acetabulum with anchors and the femur with screws. I tension it with the hip in neutral extension.
Ignoring the "Goldilocks" principle of tensioning. Not mentioning the exact hip position (extension/neutral rotation) or the clinical consequence of over-tensioning (stiffness) vs. under-tensioning (persistent instability).
Biomechanically, the fascia lata autograft serves as a robust static restraint, with tensile properties approximating the native iliofemoral ligament. Intraoperatively, the graft is fixed to the acetabulum (anchors) and the intertrochanteric line (interference screws or anchors). Tensioning is critical: the hip must be placed in 10-15 degrees of extension and neutral rotation. Over-tensioning leads to iatrogenic stiffness and adhesive capsulitis, while under-tensioning fails to provide the necessary checkrein against anterior translation, leading to reconstruction failure.
