Closed Reduction Casting: Master Techniques & Principles
Key Takeaway
Discover the latest medical recommendations for Closed Reduction Casting: Master Techniques & Principles. Closed reduction casting is a non-surgical technique to realign displaced fractures, employing axial traction and reversing the injury mechanism under adequate analgesia. After reduction, a cast provides semirigid immobilization, with careful padding around bony prominences and above/below the injury. This process aims to restore proper length, rotation, and angulation while preventing soft tissue complications.
Introduction and Epidemiology
Closed reduction and casting represents a foundational skill set in orthopedic trauma surgery, maintaining its critical relevance despite advancements in operative internal fixation. This technique offers a non-invasive, cost-effective method for stabilizing a myriad of fracture patterns across all age groups. The core objective is to restore an acceptable anatomical alignment of displaced fractures without surgical exposure, thereby minimizing additional soft tissue insult and promoting fracture healing within a meticulously applied external splint or cast. The principles underpinning successful closed reduction are rooted in biomechanics, anatomical understanding, and meticulous technique, aiming to optimize patient comfort, facilitate healing, and prevent complications.
Epidemiologically, fractures amenable to closed reduction and casting are among the most common presentations in orthopedic practice. Distal radius fractures, particularly Colles' and Smith's patterns, frequently undergo closed reduction. Ankle fractures, especially stable bimalleolar or selected trimalleolar injuries, and specific types of tibia and fibula fractures often benefit from this approach. Pediatric fractures, including supracondylar humerus fractures (often with K-wire fixation after reduction), forearm diaphyseal fractures, and buckle or greenstick fractures, are prime candidates due to their higher remodeling potential and thicker periosteal sleeves. Furthermore, closed reduction serves as a crucial temporizing measure for many fractures that will ultimately require operative fixation, providing immediate pain relief and preventing further soft tissue damage or neurovascular compromise prior to definitive surgical intervention. Mastery of these techniques is therefore indispensable for any orthopedic surgeon.
Surgical Anatomy and Biomechanics
A profound understanding of regional surgical anatomy and the biomechanical forces at play is paramount for successful closed reduction and maintenance of alignment. Fracture stability and the efficacy of external immobilization are dictated by bone geometry, surrounding soft tissue envelopes, ligamentous integrity, and the dynamic forces exerted by muscular contractions.
Anatomical Considerations for Reduction
Specific anatomical regions present unique challenges and opportunities for closed reduction. In the distal radius, the relationship of the articular surface to the radial shaft, the integrity of the volar and dorsal cortices, and the distal radioulnar joint are critical. For ankle fractures, the mortise integrity, syndesmotic stability, and the exact displacement of the talus relative to the tibia and fibula guide reduction maneuvers. The thick periosteum in children acts as a natural hinge, often facilitating reduction and contributing to stability. Knowledge of major neurovascular bundles in proximity to common fracture sites (e.g., median nerve in distal radius, common peroneal nerve around the fibular neck, brachial artery in supracondylar humerus fractures) is essential to avoid iatrogenic injury during manipulation and to monitor post-reduction neurovascular status.
Biomechanics of Fracture Stability and Immobilization
Fracture stability is influenced by inherent bone geometry, the pattern of fracture (transverse, oblique, spiral, comminuted), and the integrity of the surrounding soft tissues, including the periosteum and ligaments. Muscle pull can be a significant deforming force, necessitating adequate muscle relaxation for successful reduction.
The principle of three-point contact or fixation is fundamental to maintaining reduction within a cast or splint. This biomechanical concept dictates that stability is achieved by applying pressure at three distinct points: two points on one side of the fracture fragment and one opposing point on the other side. This creates a balanced force system that resists further displacement. For example, in a distal radius fracture, the three points might be distal to the fracture on the volar aspect, proximal to the fracture on the dorsal aspect, and at the fracture apex on the dorsal aspect, correcting volar angulation. The careful molding of the cast material to the contours of the limb is crucial for establishing and maintaining these points of contact.
Ligamentotaxis, the principle of using intact ligaments to reduce articular fragments through continuous traction, is particularly effective in periarticular fractures, such as those of the distal radius or pilon fractures. By applying longitudinal traction, capsular and ligamentous structures pull attached bone fragments into a more anatomical position, aiding indirect reduction.
The soft tissue envelope plays a dual role. While damaged soft tissues contribute to fracture instability and swelling, an intact periosteum can act as a hinge, guiding reduction and providing inherent stability, especially in pediatric fractures. However, excessive swelling post-injury or post-reduction can compromise neurovascular supply and necessitate careful monitoring, often requiring a splint instead of a circumferential cast initially.
Indications and Contraindications
The decision to pursue closed reduction and casting versus surgical fixation is a critical one, requiring careful consideration of fracture characteristics, patient factors, and potential complications.
Indications for Closed Reduction Casting
Closed reduction with external immobilization is indicated for fractures where an acceptable reduction can be achieved and maintained non-operatively, leading to a functional outcome comparable to surgical intervention.
- Minimally Displaced or Stable Fractures: Fractures with little or no displacement, or those inherently stable due to their pattern or location (e.g., non-displaced spiral tibia shaft fracture).
- Pediatric Fractures: Due to a greater remodeling potential, particularly in younger children, and a thicker periosteum aiding stability, many pediatric fractures (e.g., greenstick, buckle, minimally displaced long bone fractures) are excellent candidates.
- Fractures Amenable to Acceptable Reduction: Displaced fractures where anatomical or functional alignment can be restored and maintained using external support (e.g., many distal radius fractures, stable ankle fractures, some diaphyseal forearm fractures).
- Temporary Stabilization: As a provisional measure for highly unstable fractures or open fractures awaiting definitive surgical management, it provides pain relief and prevents further neurovascular compromise.
- Patient Comorbidities: In patients with significant medical comorbidities that preclude safe anesthesia and surgery, closed reduction and casting may be the only viable option, provided acceptable alignment can be achieved.
Contraindications for Closed Reduction Casting
Conversely, certain situations mandate surgical intervention or make closed reduction inadvisable.
- Irreducibility: If an acceptable reduction cannot be achieved due to soft tissue interposition (e.g., muscle, tendon, periosteum) or severe comminution.
- Unstable Reductions: When an initial reduction is achieved but cannot be maintained in external immobilization, leading to a high risk of re-displacement (e.g., highly comminuted, very oblique, or rotationally unstable fractures).
- Open Fractures: While initial closed reduction may be performed as part of emergency management, open fractures typically require surgical debridement and often internal fixation due to contamination and risk of infection. Definitive casting should only occur after thorough debridement.
- Neurovascular Compromise: Fractures causing acute neurovascular compromise (e.g., compartment syndrome, major vessel injury, nerve transection) that are not immediately resolved by reduction, require urgent surgical exploration.
- Intra-articular Step-off or Gap: Significant articular displacement or incongruity, especially in weight-bearing joints, often requires surgical correction to minimize the risk of post-traumatic arthritis.
- Associated Injuries: Other injuries (e.g., severe soft tissue injury, crush injury, polytrauma) that may complicate cast management or require early mobilization.
- Patient Non-compliance: Patients unable or unwilling to adhere to cast care instructions or follow-up appointments may be at higher risk for complications.
Operative Versus Non-Operative Indications
The following table provides a general summary of common orthopedic fracture types and typical indications for operative versus non-operative management.
| Fracture Type | Typical Non-Operative Indications (Closed Reduction & Casting) | Typical Operative Indications (ORIF or External Fixation) |
|---|---|---|
| Distal Radius | Minimally displaced; stable after reduction (acceptable angulation/shortening) | Unstable reductions; significant articular step-off (>2mm); irreducible fractures |
| Ankle Fractures | Stable unimalleolar; selected stable bimalleolar with intact syndesmosis | Displaced bimalleolar/trimalleolar; syndesmotic disruption; open fractures |
| Tibia Shaft | Minimally displaced stable (transverse/short oblique); pediatric diaphyseal | Displaced spiral/oblique/comminuted; open fractures; significant shortening/angulation |
| Humeral Shaft | Non-operative for most (functional bracing); stable after reduction | Open fractures; neurovascular compromise; irreducible; polytrauma |
| Forearm (Pediatric) | Greenstick; buckle; minimally displaced complete fractures | Complete displacement; irreducible; significant angulation after reduction |
| Supracondylar Humerus (Pediatric) | Type I (non-displaced) | Type II (displaced, posterior cortex intact); Type III (complete displacement); open |
Pre Operative Planning and Patient Positioning
Thorough pre-operative planning and meticulous patient positioning are crucial steps for ensuring a safe and successful closed reduction and casting procedure. This phase encompasses careful assessment, adequate analgesia, and appropriate setup.
Comprehensive Assessment
Prior to any reduction attempt, a comprehensive clinical and radiographic assessment is mandatory.
* Clinical Examination: Evaluate the skin integrity, swelling, any open wounds, and perform a detailed neurovascular assessment, documenting sensory and motor function, as well as distal pulses (or capillary refill).
* Radiographic Imaging: Obtain adequate radiographs, typically AP and lateral views, often supplemented with oblique views or comparison films of the contralateral limb, especially in children. For complex periarticular fractures, a CT scan may be indicated to fully delineate fragment anatomy and guide reduction strategy, even if closed reduction is initially planned.
* Fracture Pattern Analysis: Carefully analyze the fracture morphology, degree and direction of displacement, comminution, and any soft tissue interposition. This dictates the reduction maneuvers needed.
* Patient Factors: Consider patient age, comorbidities, ability to cooperate, and potential for remodeling.
Analgesia and Muscle Relaxation
Adequate analgesia and muscle relaxation are critical for successful reduction, minimizing patient discomfort and overcoming muscular spasm, which can impede manipulation.
- Hematoma Block: A common and effective method for many appendicular fractures, particularly distal radius and ankle fractures. Local anesthetic (e.g., 1% lidocaine without epinephrine) is injected directly into the fracture hematoma, typically 5-10 mL depending on the fracture size. Allow 10-15 minutes for onset.
- Regional Anesthesia: Anesthetic nerve blocks (e.g., axillary block for upper extremity, femoral or popliteal block for lower extremity) can provide profound analgesia and muscle relaxation, offering prolonged pain control.
- Conscious Sedation: Administered intravenously by a physician (often an emergency physician or anesthesiologist), conscious sedation (e.g., ketamine, propofol, midazolam/fentanyl combination) provides anxiolysis, analgesia, and muscle relaxation, but requires continuous monitoring of vital signs.
- General Anesthesia: For complex reductions, highly anxious patients, or those requiring sustained muscle relaxation, general anesthesia may be necessary.
Patient Positioning and Equipment
Appropriate positioning allows for optimal access, visualization, and application of reduction forces.
- Upper Extremity:
- Distal Radius: Supine position. For sustained traction, a finger trap system (traction applied via the digits with counter-traction at the elbow, often with 5-10 lbs of weight) is frequently employed. The arm should be elevated, typically around 60-90 degrees of shoulder flexion.
- Forearm: Supine, arm abducted on a hand table.
- Humerus: Supine or semi-recumbent, with an assistant providing counter-traction or directly applying traction.
- Lower Extremity:
- Ankle/Foot: Supine position with the knee flexed or hip abducted to allow access for manipulation and casting.
- Tibia/Fibula: Supine. A knee flexion position (e.g., with knee over edge of table) can facilitate access and allow gravity to assist.
Necessary Equipment
- Stockinette: To protect the skin and serve as the innermost layer.
- Cast Padding: Abundant, soft cotton or synthetic padding to protect bony prominences and allow for post-injury swelling.
- Cast Material: Plaster of Paris (exothermic reaction, longer working time) or fiberglass (lighter, stronger, faster curing).
- Water: Appropriate temperature (cooler for plaster to prolong working time, warmer for fiberglass to accelerate setting).
- Utility Scissors and Cast Shears: For cutting cast materials and padding.
- Goniometer: For measuring angulation and range of motion.
- Lead Protection: For fluoroscopy (if used).
- Fluoroscopy Unit (C-arm): Essential for intra-procedure real-time visualization of reduction and confirmation of alignment.
Detailed Surgical Approach and Technique
The execution of a closed reduction and subsequent casting is a meticulous process, demanding adherence to fundamental principles to ensure an acceptable and stable outcome.
Principles of Closed Reduction
The foundational principles guiding closed reduction are derived from the understanding of fracture mechanics and soft tissue response:
- Minimizing Soft Tissue Trauma: Even for fractures destined for internal fixation, prompt and gentle reduction minimizes ongoing soft tissue damage, reduces hematoma size, and can alleviate tension on neurovascular structures. This is particularly crucial in the initial management phase.
- Adequate Analgesia and Muscle Relaxation: As previously discussed, this is paramount. Without it, muscle spasm will prevent effective manipulation, leading to patient distress and failed reduction.
- Axial Traction and Reversal of Injury Mechanism: This is the primary maneuver. Disimpact the fracture by applying longitudinal traction in the line of the bone. Then, gently reverse the forces that caused the injury. For example, in a dorsally displaced distal radius fracture, apply traction, then perform volar flexion and ulnar deviation.
- Restoration of Length, Rotation, and Angulation: The goal is to achieve an acceptable anatomical alignment, prioritizing length restoration first, followed by correction of rotational deformities, and finally angulation.
- Length: Restoring length minimizes tension on neurovascular structures and maintains normal limb biomechanics.
- Rotation: Rotational malalignment is poorly tolerated, especially in the forearm and lower extremity. Clinical assessment (e.g., examining finger cascades for upper limb, foot position for lower limb) is essential as it is difficult to assess radiographically.
- Angulation: Correction of varus/valgus or anterior/posterior angulation is typically achieved through direct manipulation over the fracture site after traction.
- Location-Specific Maneuvers: While general principles apply, specific fractures require tailored techniques. For instance, pronation for reducing an apex dorsal distal radius fracture (Galeazzi-type) or specific molding techniques for supracondylar humerus fractures.
- Immobilize the Joint Above and Below: To effectively stabilize the fracture, the cast or splint must span the joint proximal and distal to the injury, preventing movement that could compromise the reduction. Exceptions exist, such as a sugar-tong splint for a forearm fracture which necessarily includes the elbow, or a short leg cast for an ankle fracture.
- Three-Point Contact and Stabilization: This biomechanical principle is essential to maintain reduction. The cast must be molded to provide counter-pressures at three distinct points around the fracture to prevent re-displacement. One point is typically at the apex of the deformity (correcting point), with two opposing points proximal and distal to the fracture.
General Reduction Steps
- Pre-Reduction Set Up: Ensure adequate analgesia, patient positioning, and all necessary equipment are at hand. Position the C-arm for optimal AP and lateral views without repositioning the limb.
- Traction and Disimpaction: Apply sustained axial traction to disimpact the fracture fragments and restore length. This often requires an assistant or a finger-trap system.
- Correction of Angulation and Rotation: While maintaining traction, manipulate the distal fragment by reversing the mechanism of injury. Apply direct pressure over the fracture site (e.g., applying volar pressure to reduce dorsal angulation of a distal radius fracture).
- Verification of Reduction: Use fluoroscopy to confirm acceptable alignment in both AP and lateral planes. Assess length, angulation, and articular congruity. For rotation, rely on clinical assessment.
Splinting and Casting Techniques
Once an acceptable reduction is achieved, immobilization must be applied immediately and meticulously to maintain the reduction.
-
Soft Tissue Respect and Padding:
- Pad all bony prominences: Generous padding (at least 2-3 layers) is crucial over areas like the olecranon, humeral epicondyles, ulnar styloid, malleoli, and fibular head to prevent pressure sores.
- Allow for post-injury swelling: Initial immobilization should often be with a splint rather than a circumferential cast to accommodate swelling. Even with a cast, ensure padding is not too tight and apply the cast in a non-constrictive manner.
- ``
-
Application of Stockinette and Padding: Apply a stockinette, extending beyond the planned cast length. Follow with liberal cast padding, ensuring there are no wrinkles and that it's applied without excessive tension. The "Bulky Jones" technique emphasizes abundant cast padding to accommodate swelling.
 -
Splinting Techniques (Custom Made): Splints are advantageous initially due to swelling.
- Bulky Jones Splint:
- Lower Extremity: Commonly applied for foot, ankle, and fractures about the knee. Uses fluffy cotton or abundant cast padding to manage post-injury swelling. A posterior slab is applied from below the knee to the tips of the toes (or mid-calf to toes). For ankle/tibia, a U-shaped slab is applied from medial to lateral around the malleoli. For knee injuries, a knee immobilizer or a long posterior leg splint with a well-molded knee provides immobilization. The extremity should be padded well proximal and distal to the injury.
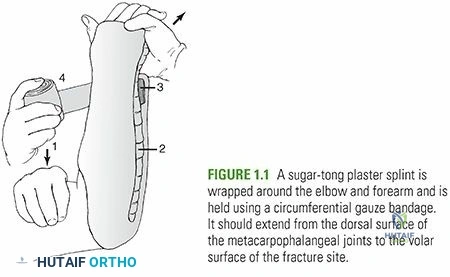
- Sugar-Tong Splint:
- Upper Extremity: Predominantly for distal forearm fractures. A U-shaped slab is applied from the volar aspect of the hand, encircling the elbow, and extending dorsally along the forearm to the metacarpal heads. This provides excellent rotational control for forearm fractures. The elbow is typically flexed to 90 degrees and the forearm in neutral rotation.
- Coaptation Splint:
- Upper Extremity: For humerus shaft fractures. A U-shaped slab is applied to the medial and lateral aspects of the arm, extending from the axilla around the elbow to the shoulder. It's often combined with a coaptation dressing or sugar-tong to prevent rotation and sag.
- Volar Forearm Splint: For stable wrist injuries, carpal fractures, or as a temporary measure. Extends from the palm to just below the elbow, immobilizing the wrist in slight extension.
- Dorsal Forearm Splint: Less common as a primary splint due to potential for pressure on dorsal veins, but can be used in combination.
- Thumb Spica Splint: For injuries involving the thumb metacarpal or phalanges, or scaphoid fractures. Immobilizes the thumb and wrist.
- Bulky Jones Splint:
-
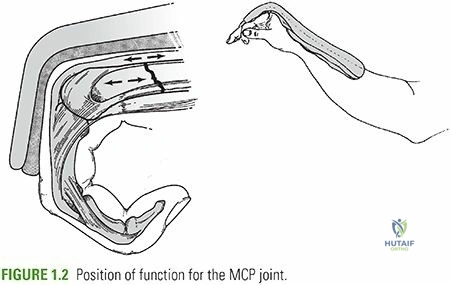
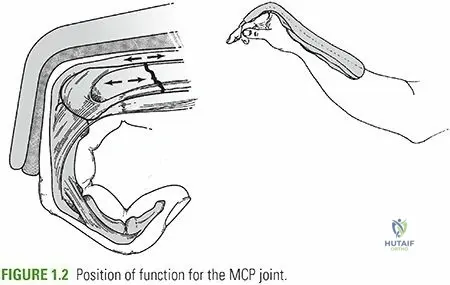
Molding: This is the most critical step for maintaining reduction. While the cast material is setting, carefully mold the cast to create the three-point contact and anatomical contours. Ensure the position of function for the immobilized joints is maintained (e.g., wrist in slight extension, elbow at 90 degrees).
-
Post-Reduction Radiographs: Immediately after the cast or splint has set, obtain repeat AP and lateral radiographs to confirm that the reduction has been maintained during cast application.
-
Patient Education and Discharge: Provide clear instructions on elevation, ice application, pain management, neurovascular monitoring (what signs to watch for, e.g., increasing pain, numbness, pallor, tingling, inability to move fingers/toes), and emergency contact information. Schedule follow-up imaging (typically within 7-10 days to assess for loss of reduction as swelling subsides).

Complications and Management
Despite its relative safety, closed reduction and casting is not without potential complications, both early and late. Vigilance and prompt intervention are crucial for optimal outcomes.
Common Complications and Salvage Strategies
| Complication | Incidence | Pathophysiology / Clinical Presentation | Salvage Strategy |
|---|---|---|---|
| Compartment Syndrome | Rare but devastating (0.1-10% depending on fracture type and location) | Increased pressure within a closed fascial compartment, compromising neurovascular function. Severe pain, paresthesia, pallor, pulselessness. | Emergency fasciotomy. Early recognition is critical. Remove constrictive dressing/cast immediately. If symptoms persist or worsen, measure compartment pressures. |
| Loss of Reduction (Re-displacement) | Varies widely (5-30%), depends on fracture stability and cast technique | Inadequate initial reduction, unstable fracture pattern, poor cast molding, excessive swelling leading to cast loosening, patient non-compliance. | Early re-reduction and recasting. If reduction is acceptable after re-manipulation, continue non-operative management. If repeatedly unstable or unacceptable, convert to operative fixation (e.g., K-wires, plate fixation). |
| Neurovascular Compromise | <5% | Direct injury during trauma or reduction, nerve entrapment by fracture fragments, compression by tight cast/splint, swelling. | Remove cast/splint immediately. Re-evaluate neurovascular status. If due to fracture displacement, attempt re-reduction. If persistent despite adequate reduction and loosening of external compression, urgent surgical exploration may be required. |
| Skin Breakdown / Pressure Sore | 1-5% | Inadequate padding over bony prominences, cast applied too tightly, foreign body in cast, prolonged immobilization. | Immediate cast bivalving/removal and inspection. Treat skin injury. Reapply cast/splint with additional padding and meticulous technique. Educate patient on signs of pressure points. |
| Thermal Injury (Cast Burn) | Rare (<0.1%) | Exothermic reaction during plaster setting, especially with warm water and rapid application of multiple layers. | Immediate cast removal. Treat burn according to severity. Monitor for infection. |
| Malunion | Varies greatly based on fracture type and acceptable limits (5-20%) | Healing of a fracture in an anatomically unacceptable position (angulation, rotation, shortening). | Early detection through regular radiographic follow-up. For symptomatic malunion or severe deformity, corrective osteotomy and internal fixation. Many malunions are asymptomatic and do not require intervention, particularly in children or non-weight-bearing bones if functional. |
| Nonunion | <5% (varies greatly by bone/site) | Failure of a fracture to heal after an appropriate period (typically 6-9 months), often due to inadequate immobilization, poor biology, or excessive distraction. | Surgical intervention: Debridement of fibrous tissue, bone grafting (autograft/allograft), and internal fixation (plate/nail). May require revision of immobilization strategy if identified early. |
| Joint Stiffness / Post-traumatic Arthritis | Common, especially with intra-articular fractures (10-50%) | Prolonged immobilization, articular incongruity (even if subtle), capsular contracture, scarring. | Early judicious mobilization (when appropriate). Physical and occupational therapy. For severe, symptomatic arthritis, surgical options include arthroscopy, osteotomy, arthroplasty, or arthrodesis. |
| Complex Regional Pain Syndrome (CRPS) | <1% | Pathological pain response after trauma, often with autonomic features (swelling, skin changes, temperature changes, allodynia). | Multidisciplinary approach: Physical therapy, neuropathic pain medications (gabapentin, pregabalin), regional nerve blocks, psychological support. Early recognition and aggressive management are key. |
Post Operative Rehabilitation Protocols
Post-reduction and casting rehabilitation is an integral part of fracture management, aiming to optimize functional recovery while protecting the healing fracture. Protocols vary significantly based on the fracture type, stability, and patient factors.
Immobilization Phase
This initial phase focuses on protecting the healing fracture and managing early symptoms.
- Elevation: Keep the injured limb elevated above heart level, especially for the first 48-72 hours, to minimize swelling and edema.
- Ice Application: Apply ice packs intermittently over the cast/splint, being cautious to avoid frostbite, to further reduce swelling and pain.
- Pain Management: Prescribe appropriate analgesics, starting with NSAIDs or acetaminophen, escalating to opioids if necessary for breakthrough pain.
- Neurovascular Monitoring: Patients must be educated to monitor for any signs of neurovascular compromise (numbness, tingling, increasing pain, pallor, inability to move digits).
- Early Digital Motion: Encourage active range of motion of all uninvolved joints, particularly fingers and toes, to prevent stiffness, improve circulation, and reduce swelling. For upper extremity casts, shoulder and elbow (if not immobilized) motion is crucial.
- Weight-bearing Restrictions: Adhere strictly to non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) instructions for lower extremity fractures as per the fracture stability and healing stage. Crutch or walker training is essential.
- Cast Care: Instruct patients on keeping the cast dry and clean, avoiding foreign objects inside the cast, and reporting any skin irritation or foul odor.
Transition to Mobilization
Typically, after an initial period of immobilization (e.g., 4-6 weeks for many distal radius fractures, 6-10 weeks for tibia fractures), the cast or splint is removed. Radiographic evidence of early healing (e.g., callus formation) should be present.
- Initial Range of Motion (ROM):
- Passive ROM: Gentle passive motion, initially guided by a therapist, to regain joint flexibility.
- Active-Assisted ROM: Patient participates in movement with assistance.
- Active ROM: Independent movement by the patient.
- Focus on the joints that were immobilized, gradually increasing the arc of motion.
- Edema Control: Continued elevation, compression garments, and gentle massage techniques to manage residual swelling.
- Strengthening: Once a reasonable range of motion is achieved and pain allows, progressive resistive exercises are introduced to rebuild muscle strength and endurance. This might start with isometric exercises, progressing to elastic bands, light weights, and functional movements.
- Scar Management: If any open wounds were present or skin breakdown occurred, scar massage and desensitization may be necessary.
- Functional Training: Integration of the injured limb into daily activities. For lower extremity fractures, this involves progressive weight-bearing exercises, gait training, and balance activities. For upper extremity, it focuses on fine motor skills, grip strength, and tasks of daily living.
- Occupational and Physical Therapy Referrals: Essential for structured and supervised rehabilitation, especially for complex fractures or patients at risk for stiffness or weakness.
Long-Term Rehabilitation
- Return to Activity: Gradually progress to sport-specific or work-specific activities, ensuring adequate strength, flexibility, and confidence.
- Monitoring for Complications: Continue to monitor for late complications such as malunion, nonunion, or post-traumatic arthritis, which may require further intervention.
- Patient Education: Reinforce the importance of continued home exercise programs and activity modification as needed.
Summary of Key Literature and Guidelines
The practice of closed reduction and casting is continuously refined by clinical experience, biomechanical studies, and evidence-based medicine. Several key sources guide contemporary orthopedic practice.
AO Principles
The AO Foundation principles emphasize accurate reduction and stable fixation, respect for soft tissues, and early, pain-free mobilization. While often associated with internal fixation, these principles fundamentally apply to closed reduction as well, particularly regarding anatomic reduction, gentle soft tissue handling, and the imperative for stable immobilization to allow for biological healing. The "bridge plating" concept for comminuted diaphyseal fractures, for instance, has its non-operative corollary in closed reduction and casting where the periosteum acts as the biological "bridge."
American Academy of Orthopaedic Surgeons (AAOS) Guidelines
The AAOS develops clinical practice guidelines (CPGs) for various orthopedic conditions, including numerous fracture types. These guidelines often provide evidence-based recommendations on the utility of closed reduction versus operative management for specific fractures, defining acceptable reduction parameters and recommended follow-up schedules. For example, CPGs for distal radius fractures outline specific radiographic criteria (e.g., dorsal angulation <10 degrees, radial shortening <3mm) for acceptable closed reduction, beyond which operative intervention is often favored. Similar guidelines exist for ankle and pediatric fractures.
Major Trauma Texts and Atlases
Comprehensive textbooks such as "Skeletal Trauma" by Browner, Jupiter, Krettek, and Anderson; "Campbell's Operative Orthopaedics"; and specialized pediatric orthopedic texts (e.g., "Rockwood and Wilkins' Fractures in Children") serve as encyclopedic references. They detail specific reduction techniques, acceptable radiographic parameters, and casting protocols for nearly every fracture pattern, often incorporating historical context, anatomical insights, and practical pearls from experienced surgeons.
Evolution of Casting Materials and Techniques
Historically, plaster of Paris was the sole option. Its advantages include excellent moldability and lower cost, though its weight and longer setting time can be drawbacks. The advent of fiberglass casting materials revolutionized external immobilization, offering superior strength-to-weight ratio, durability, and water resistance, albeit with a higher cost and faster setting time requiring more rapid application. Hybrid techniques, combining plaster for molding with fiberglass for strength, are also employed. The understanding of appropriate padding and splinting versus circumferential casting has also evolved, emphasizing the importance of initial splinting to accommodate swelling, reducing the risk of compartment syndrome.
Role as Definitive Treatment and Temporizing Measure
Current literature underscores closed reduction as a definitive treatment for a significant proportion of fractures, particularly in pediatric populations and stable adult fractures, achieving outcomes comparable to surgical methods with fewer risks. Simultaneously, its role as an immediate temporizing measure for acutely displaced or open fractures awaiting definitive surgical stabilization remains paramount. This allows for stabilization, pain control, and protection of neurovascular structures while definitive surgical planning is underway. The emphasis is consistently on achieving an "acceptable" reduction rather than a purely "anatomical" one if the latter requires excessive manipulation or carries greater risk.
Future Directions
Research continues into advanced casting materials, imaging techniques to better assess fracture stability (e.g., dynamic ultrasound), and the long-term outcomes of various reduction and immobilization strategies. Telemedicine and remote monitoring are also emerging areas, allowing for more frequent follow-up and earlier detection of complications in casted patients. The principles, however, of meticulous technique, anatomical understanding, and respect for soft tissues, will remain the cornerstones of effective closed reduction and casting.
Clinical & Radiographic Imaging