Advanced Reconstruction of Ankle and Hindfoot Malunions: Osteotomies and Arthrodesis
Key Takeaway
Reconstructive surgery for ankle and hindfoot malunions requires precise restoration of biomechanical alignment. This guide details the surgical management of calcaneal malunions via subtalar arthrodesis and corrective osteotomies, alongside fibular lengthening techniques for bimalleolar malunions. Emphasizing evidence-based indications, step-by-step surgical approaches, and postoperative protocols, it provides orthopedic surgeons with a comprehensive framework for optimizing functional outcomes and mitigating posttraumatic arthritis.
Introduction to Ankle and Hindfoot Malunions
The management of malunited fractures of the ankle and hindfoot represents one of the most formidable challenges in reconstructive orthopedic surgery. Malunions in this anatomically complex and highly loaded region inevitably lead to altered contact mechanics, progressive posttraumatic arthritis, and profound functional disability. The primary goal of surgical intervention is the precise restoration of the mechanical axis, joint congruency, and ligamentous stability to halt degenerative cascades and relieve pain.
Historically, the magnitude of normal contact stresses was considered the primary driver of posttraumatic arthritis. However, contemporary biomechanical models have elucidated the profound impact of even minor spatial displacements. Thordarson et al. utilized a cadaveric model of a pronation-lateral rotation ankle injury to evaluate the effect of fibular malunion on tibiotalar contact pressures. Their findings were definitive: shortening or lateral displacement of the fibula by 2 mm or more, or an external rotation of 5 degrees or more, significantly increased contact pressures in the posterolateral and midlateral quadrants of the talar dome. This was accompanied by a corresponding decrease in contact pressures in the medial quadrants. Consequently, anatomical reduction of the lateral malleolus is paramount to diminishing the risk of posttraumatic arthritis.
Clinical Evaluation and Indications for Surgery
Surgical decision-making must be highly individualized, taking into account the patient's age, functional demands, occupation, severity of the deformity, duration of the malunion, existing range of motion, and the presence of established arthritic changes.
When surgery is indicated, the fundamental choice lies between a joint-preserving realignment osteotomy and a salvage arthrodesis. Often, a meticulously executed osteotomy can fulfill both the restoration of weight-bearing alignment and the relief of early arthritic symptoms.
The "Overt" vs. "Occult" Malunion
Yablon and Leach categorized lateral malleolar malunions into two distinct clinical entities:
1. Overt Malunions: Characterized by obvious displacement of the talus within the mortise alongside the malunited lateral malleolus.
2. Occult Malunions: Characterized by isolated shortening and external rotation of the lateral malleolus without gross talar shift on standard radiographs.
Patients with occult malunions often function reasonably well for an average of 5 years before developing poorly localized, diffuse, activity-related pain, followed by swelling 3 to 6 months later.
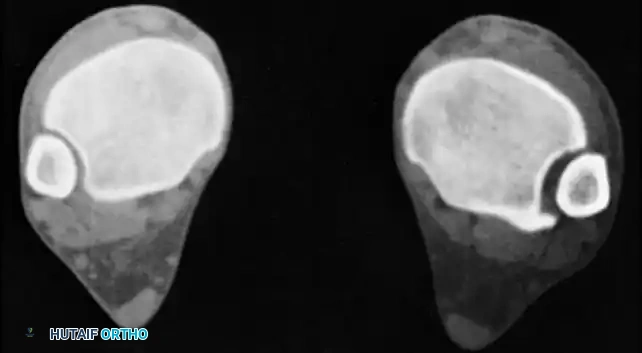
Fig. 55-9 CT scan of occult malunion. Right ankle (left) is normal; left ankle shows widening of the distal tibiofibular joint, indicating fibular shortening and external rotation of the lateral malleolus.
Clinical Pearl: Advanced imaging, particularly computed tomography (CT), is mandatory for evaluating suspected occult malunions. Widening of the distal tibiofibular syndesmosis on axial cuts is a hallmark sign of fibular shortening and external rotation.
Surgical Management of Calcaneal Malunions
Calcaneal malunions frequently present with loss of height, increased heel width, subfibular impingement, and subtalar arthritis. Surgical reconstruction is dictated by the Stephens and Sanders classification, specifically addressing Type II (subtalar arthritis with normal heel morphology) and Type III (subtalar arthritis with severe axial deformity) malunions.
Subtalar Arthrodesis and Bone Grafting (Type II Malunion)
For Type II malunions, an in situ subtalar arthrodesis with structural bone grafting is indicated to restore calcaneal height and fuse the degenerative joint.
Surgical Steps:
* Approach and Preparation: Utilize an extensile lateral approach. Carefully elevate a full-thickness subperiosteal flap. Do not release the deltoid ligament from inside the subtalar joint; doing so renders the joint highly unstable and may result in overdistraction of the graft.
* Graft Placement: Place the previously excised lateral wall fragment (exostosis) within the prepared subtalar joint as an autograft bone block. This bone can be folded over on itself to obtain more height if needed. It must completely fill the subtalar joint, as the height of the lateral calcaneus (and the graft) is usually equal to the width of the posterior facet. Supplement with cancellous allograft chips in the debrided sinus tarsi to enhance fusion rates.
* Provisional Fixation: Hold the subtalar joint in neutral to slight valgus alignment (approximately 5 degrees). Place two terminally threaded 3.2-mm guide pins percutaneously from the posterior plantar edge of the calcaneal tuberosity. Advance them across the subtalar joint, perpendicular to the plane of the posterior facet, and into the talar dome.
* Trajectory Optimization: Angle the guide pins in a divergent fashion into the talar dome to maximize rotational stability. Strictly avoid placing a pin into the lateral aspect of the ankle joint.
* Imaging Verification: Obtain intraoperative fluoroscopic anteroposterior (AP), mortise, and axial calcaneal views to verify correct pin placement, graft seating, and hindfoot alignment.
* Supplemental Fixation: If enhanced stability is required, place a third guide pin from the plantar margin of the anterior process of the calcaneus into the distal aspect of the talar neck and head. Ensure the talonavicular joint is not violated.
* Definitive Fixation: Overdrill and place large-fragment, partially threaded (7.3 mm or 8.0 mm) cannulated screws in lag mode to achieve robust compression across the arthrodesis site.
Axial Realignment and Arthrodesis (Type III Malunion)
In patients with a Type III malunion, correction of the axial malalignment is a prerequisite to fusion. Rotation of the midfoot in the coronal plane around an AP axis (pronation-supination) cannot compensate for a calcaneal tuberosity rigidly healed in varus or valgus.
- Varus Malalignment: Perform a Dwyer lateral closing wedge osteotomy posterior to the posterior facet.
- Valgus Malalignment: Perform a medial displacement calcaneal osteotomy with rotation.
- Fixation Sequence: Complete the osteotomy prior to placing the fixation for the subtalar arthrodesis. Once the osteotomy is reduced, insert the guide pins as described above. This allows the osteotomy and the subtalar fusion to be compressed simultaneously by the same lag screws. Any bone removed during a closing wedge osteotomy should be morselized and utilized as local autograft.
Management of Peroneal Tendon Pathology
Lateral wall blowout frequently leads to peroneal tendon subluxation, dislocation, or stenosing tenosynovitis.
- Decompression: Remove the Kirschner wires and examine the tendons. In many cases, simple removal of the lateral wall exostosis allows the tendons to fall back into their anatomic position behind the fibula.
- Tenolysis: Enter the peroneal tendon sheath distally with a Freer elevator to evaluate for proximal stenosis. If stenosis is identified, incise the sheath over a length of 2 to 3 cm along the undersurface of the subperiosteal flap to perform a thorough tenolysis.
- Retinacular Reconstruction: If frank peroneal tendon dislocation is identified, reconstruct the superior peroneal retinaculum through a small, separate incision in the flap to ensure dynamic stability.
Soft Tissue Management and Closure
Wound complications are the Achilles heel of calcaneal reconstruction. Meticulous layered closure is non-negotiable.
- Place a deep closed-suction drain exiting at the proximal tip of the vertical limb of the incision.
- Pass interrupted 0-Vicryl sutures through the deep layers of the subperiosteal flap, angling the needle such that the flap is advanced toward the apex of the incision to reduce tension.
- Clamp all deep sutures until they are entirely placed. Hand-tie them sequentially, starting at the proximal and distal ends and working toward the apex.
- Close the subcuticular layer with interrupted 2-0 Vicryl, followed by the skin with 3-0 nylon, again progressing from the ends toward the apex.
- Salvage technique: If massive height restoration prevents tension-free wound closure at the apex, extend the vertical limb of the incision proximally. This allows the flap to shift and rotate downward, leaving the proximal extension open to heal by secondary intention.
Reconstructive Osteotomies for Bimalleolar Ankle Malunions
The decision to perform a joint-preserving osteotomy versus an ankle arthrodesis hinges on the condition of the articular cartilage. Fogel and Sim historically suggested that displacement of the talus for more than 3 months results in irreversible chondral damage, portending a poor outcome for osteotomy. However, contemporary literature (Offierski, Bircher, Hughes, Weber, Marti) demonstrates that if normal weight-bearing alignment and precise articular relationships are restored, excellent function can be achieved even in delayed presentations.
Yablon and Leach emphasized that abnormal-appearing cartilage does not strictly preclude a good result. They recommend preoperative arthroscopy to evaluate the joint. Arthrodesis is reserved for complete loss of articular cartilage on the talus or tibial plafond; if any viable cartilage remains, a realignment osteotomy should be attempted.
Biomechanical Prerequisites for Ankle Restoration
Weber and Simpson defined three absolute radiographic requirements for the anatomical restoration of the ankle joint:
1. A perfectly equidistant and parallel tibiotalar joint space.
2. The fibular spike must reside in its normal position, pointing exactly to the level of the distal tibial subchondral bone (confirming correct fibular length).
3. A normal, unbroken continuous curve from the lateral articular surface of the talus to the recess of the distal fibula where the peroneal tendons lie (Shenton's line of the ankle).
Surgical Technique: Fibular Lengthening Osteotomy (Weber Technique)
Fibular shortening is the most common deformity in ankle malunions. Lengthening and internally rotating the fibula is critical to restoring the mortise.
Surgical Warning: Failure to adequately clear the syndesmosis of scar tissue is the most common reason for inability to mobilize and lengthen the distal fibular fragment.
Step 1: Approach and Osteotomy Preparation
Make a longitudinal lateral incision over the previous fibular fracture, curving slightly anteriorly at its distal extent. Expose the malunion site. Using an oscillating saw or sharp osteotome, create a transverse or oblique osteotomy through the fibula at the apex of the deformity.
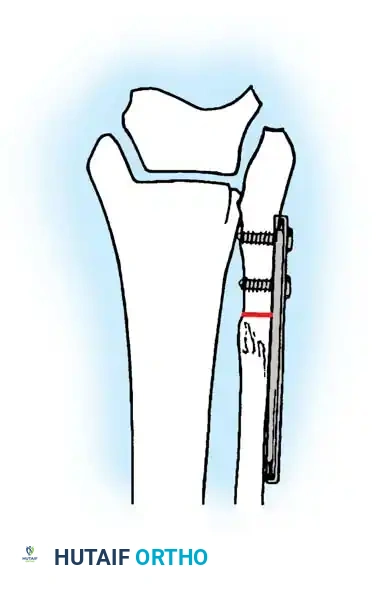
Fig. 55-10A: A five-hole or six-hole 3.5-mm dynamic compression plate is secured to the distal fibular fragment with two screws, and the osteotomy is made.
Step 2: Syndesmotic Release and Plate Application
Radically excise all fibrotic scar tissue between the fibula and tibia (within the syndesmotic incisura) to allow unhindered distal translation and internal rotation of the lateral malleolus. Create a small recess in the distal fibula to prevent hardware prominence. Attach a 3.5-mm dynamic compression plate (DCP) or locking compression plate (LCP) to the distal fragment using two screws. Ensure the plate is positioned slightly posterior on the distal fragment to account for the natural anterior bow of the fibula.
Step 3: Distraction and Realignment
Apply an articulated tension device (distractor) to the proximal fibular shaft and connect it to the proximal end of the plate.
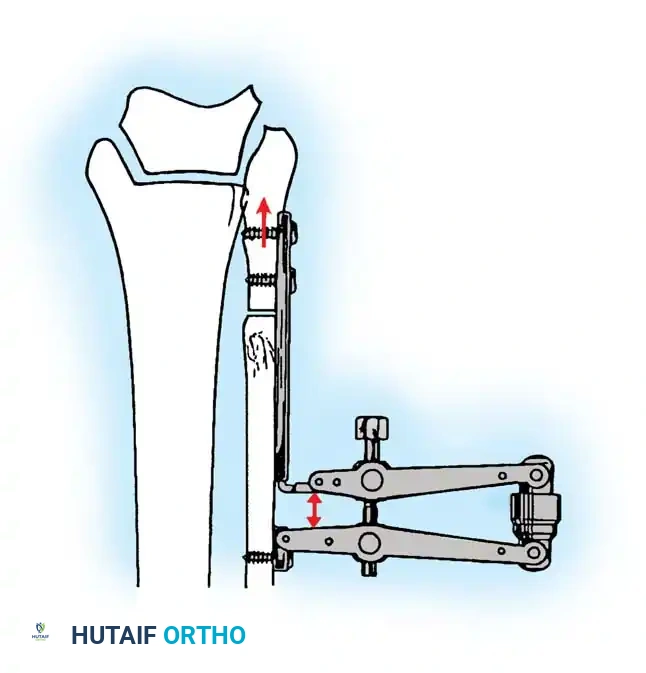
Fig. 55-10B: Controlled lengthening is obtained using the distraction device. The distal fragment is pulled distally and rotated internally to restore the mortise.
Carefully distract the osteotomy. Monitor the reduction fluoroscopically, ensuring the talus follows the lateral malleolus and the medial clear space is restored. The fibula must be pulled distally to restore the Shenton line of the ankle and rotated internally to correct the typical external rotation deformity.
Step 4: Structural Grafting and Definitive Fixation
Once anatomical length and rotation are achieved, measure the resulting osteotomy gap. Harvest a precisely matched corticocancellous block autograft from the ipsilateral proximal tibia or iliac crest.
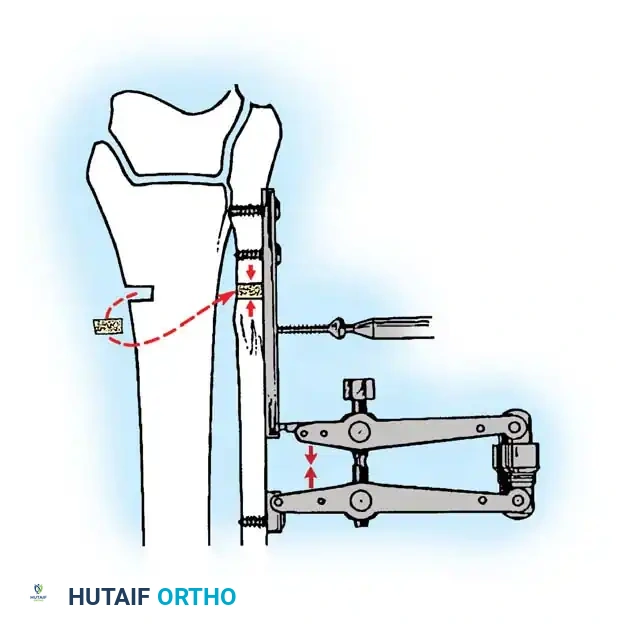
Fig. 55-10C: The corticocancellous graft is impacted into the osteotomy defect. Compression is applied across the graft via the tension device, and the remaining proximal screws are inserted to secure the construct.
Insert the remaining screws into the proximal fragment. If syndesmotic instability persists after fibular length is restored, place a position screw across the syndesmosis.
Revision Fixation for Complex Bimalleolar Malunions
In cases involving both medial and lateral malleolar malunions, particularly in osteopenic bone, robust fixation strategies are required. The medial malleolus may require osteotomy, curettage of fibrous nonunion tissue, and structural grafting.

Fig. 55-8 A and B, Malunion of a bimalleolar ankle fracture previously fixed with interfragmentary screws in an elderly patient. C and D, Revision fixation utilizing a one-third tubular buttress plate with hydroxyapatite grafting for the medial malleolus, and tension band wire fixation for the lateral malleolus.
Postoperative Protocols and Rehabilitation
Successful reconstruction relies heavily on strict adherence to postoperative rehabilitation protocols to protect the osteotomies and arthrodesis sites while promoting biological healing.
- Phase I (0-2 Weeks): The limb is placed in a well-padded, short-leg splint. Strict non-weight-bearing (NWB) status is enforced. Elevation above heart level is critical to manage edema and protect the soft tissue envelope. Deep vein thrombosis (DVT) prophylaxis is administered per institutional guidelines.
- Phase II (2-6 Weeks): Sutures are removed at 2 to 3 weeks, provided the incisions are fully healed. The patient is transitioned to a rigid cast or a locked controlled ankle motion (CAM) boot. NWB status is maintained. If an osteotomy was performed without arthrodesis, gentle active range of motion (AROM) may be initiated out of the boot if rigid internal fixation was achieved.
- Phase III (6-12 Weeks): Radiographs are obtained at 6 weeks to assess callus formation and graft incorporation. If clinical and radiographic signs of healing are present, progressive partial weight-bearing (PWB) is initiated in the CAM boot, advancing by 25% body weight weekly. Physical therapy focuses on restoring tibiotalar and subtalar kinematics, peroneal strengthening, and proprioceptive retraining.
- Phase IV (12+ Weeks): Transition to standard footwear, often utilizing a custom orthotic or ankle brace for transitional support. High-impact activities are restricted until complete radiographic consolidation is confirmed, typically between 4 to 6 months postoperatively.
By adhering to these rigorous biomechanical principles and meticulous surgical techniques, orthopedic surgeons can reliably salvage complex ankle and hindfoot malunions, restoring function and significantly delaying or preventing the onset of end-stage posttraumatic arthritis.
🔗 Read the comprehensive guide: Operative Principles of Lower Extremity Arthrodesis: Ankle and Knee
