Orthopedic Anatomy Practice Questions (Set 1): Musculoskeletal & Clinical Concepts for AAOS/ABOS

Key Takeaway
This high-yield question set (Set 1) for AAOS/ABOS exams rigorously tests foundational orthopedic anatomy. It covers essential musculoskeletal structures, clinical anatomy applications, and topographical regions critical for understanding orthopedic principles and surgical approaches, ensuring comprehensive board preparation.
Orthopedic Anatomy Practice Questions (Set 1): Musculoskeletal & Clinical Concepts for AAOS/ABOS
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
During a retroperitoneal approach to the L4-5 disk, what structure must be ligated to safely mobilize the common iliac vessels toward the midline from laterally and gain exposure?
Explanation
Question 2
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms?
Explanation
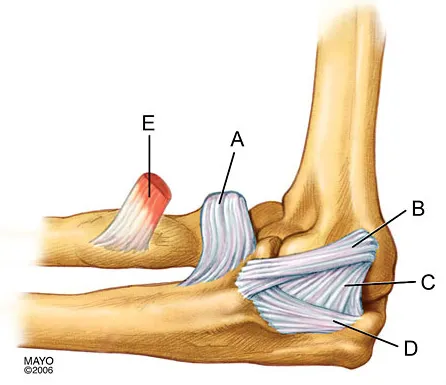
Question 3
In Figure 2, which of the following structures is the primary stabilizer in preventing valgus instability of the elbow?
Explanation
Question 4
When performing surgical excision of the lesion shown in the MRI scan in Figure 3, what nerve is most likely at risk?
Explanation
Question 5
Figure 4a shows the radiograph of a 20-year-old man who has an injury to the right shoulder. Figure 4b shows an arthroscopic view (posterior portal). The arrow points to a
Explanation
Question 6
A 15-year-old girl who swims the breaststroke has had hip pain after training excessively for a national level competition. Based on the MRI scans shown in Figures 5a through 5c, what is the most likely diagnosis?
Explanation
Question 7
During placement of an external fixator for a distal radius fracture, the most commonly injured nerve is a branch of which of the following nerves?
Explanation
Question 8
Figure 6 shows a sagittal oblique MRI scan. The arrow is pointing to what structure?
Explanation
Question 9
An 18-year-old woman sustains a twisting injury of the knee while skiing. Figures 7a and 7b show the radiograph and coronal MRI scan of the knee. In addition to the injury shown, what is the most likely associated injury?
Explanation
Question 10
A 42-year-old athletic trainer has a persistent popping sensation about the lateral ankle associated with weakness and pain following a remote injury. Deficiency in what structure directly leads to this pathology?
Explanation
Question 11
A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely occurred at which of the following locations?
Explanation
Question 12
A woman with a neck and chest tumor has weakness in the biceps and paresthesias in the thumb. Brachioradialis and infraspinatus function are normal. The lesion is affecting which of the following structures?
Explanation
Question 13
Figure 8 shows the radiograph of a 76-year-old man who has knee pain and swelling. History reveals that he underwent total knee arthroplasty 18 years ago. What is the most likely diagnosis?
Explanation
Question 14
Which of the following radiographic images is best for detecting anterior acetabular deficiency in the dysplastic hip?
Explanation
Question 15
Figure 9 shows the AP radiograph of a 65-year-old man who has knee pain and swelling. What is the most likely diagnosis?
Explanation
Question 16
If a surgeon inadvertently burrs through the midlateral wall of C5 during a anterior corpectomy, what structure is at greatest risk for injury?
Explanation
Question 17
In patients with displaced radial neck fractures treated with open reduction and internal fixation with a plate and screws, the plate must be limited to what surface of the radius to avoid impingement on the proximal ulna?
Explanation
Question 18
A 57-year-old man reports right hip pain that has been progressive for the past several months. The pain is exacerbated by weight-bearing activities and improves somewhat with rest. A radiograph is shown in Figure 10a and a coronal T1-weighted MRI scan is shown in Figure 10b. What is the most likely diagnosis?
Explanation
Question 19
The arrow in Figure 11 points toward a finding consistent with which of the following?
Explanation
Question 20
The attachments of the transverse carpal ligament include which of the following structures?
Explanation
Question 21
A 23-year-old woman falls from a bicycle and sustains a right knee injury. Figures 12a through 12d show radiographs and MRI scans of the knee. What is the most likely diagnosis?
Explanation
Question 22
A 25-year-old man has a mass on the medial aspect of the left knee. He reports that the mass has been present for several years, but a recent increase in physical activity has resulted in periodic tenderness. Radiographs are shown in Figures 13a and 13b. What is the most likely diagnosis?
Explanation
Question 23
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?
Explanation
Question 24
A patient is treated with volar plating for a distal radius fracture. The CT scan shown in Figure 15 is obtained after union of the fracture because the patient reports ongoing symptoms. The prominent hardware is most likely injuring what tendon?
Explanation
Question 25
A 9-year-old child sustains a proximal tibial physeal fracture with a hyperextension mechanism. What structure is at most risk for serious injury?
Explanation
Question 26
During an open posterior approach to the shoulder, the axillary nerve is at risk as it exits the quadrangular space. What forms the superior boundary of this space?
Explanation
Question 27
In the lumbar spine, a far-lateral (extraforaminal) disc herniation at the L4-L5 level will most likely result in direct compression of which neural structure?
Explanation
Question 28
During the ilioinguinal approach to the acetabulum, significant hemorrhage occurs while dissecting near the superior pubic ramus. This is most likely due to an injury to the corona mortis, which represents an anastomosis between the obturator vessels and which of the following?
Explanation
Question 29
The deep branch of the medial femoral circumflex artery (MFCA) provides the primary blood supply to the femoral head. Prior to piercing the hip capsule, it courses posteriorly between which two muscles?
Explanation
Question 30
During reconstruction of the coracoclavicular (CC) ligaments for an acromioclavicular joint separation, anatomic placement is crucial. Which of the following best describes the normal anatomic orientation of the CC ligaments?
Explanation
Question 31
During an anterior cervical discectomy and fusion (ACDF), excessive lateral dissection risks injury to the vertebral artery. At which cervical level does the vertebral artery typically enter the transverse foramen?
Explanation
Question 32
When treating stenosing tenosynovitis (trigger finger) surgically, the A1 pulley is released. To prevent biomechanical bowstringing of the flexor tendons, which two pulleys of the finger must remain intact?
Explanation
Question 33
When establishing the anterolateral portal for ankle arthroscopy, the superficial peroneal nerve (SPN) is at risk. What is the most reliable external landmark to minimize injury to the SPN during portal placement?
Explanation
Question 34
The volar (Henry) approach to the proximal radius exposes the bone while navigating between muscle intervals. To safely protect the posterior interosseous nerve (PIN) during proximal exposure, the forearm should be placed in which position?
Explanation
Question 35
The direct lateral (Hardinge) approach to the hip involves splitting the gluteus medius. To avoid denervating the anterior portion of the gluteus medius, the proximal split should not extend beyond what distance from the tip of the greater trochanter?
Explanation
Question 36
During surgical reconstruction of the posterolateral corner (PLC) of the knee, accurate femoral tunnel placement is required. What is the normal anatomic relationship of the femoral footprints of the fibular collateral ligament (FCL) and the popliteus tendon?
Explanation
Question 37
During the deltopectoral approach to the shoulder, the conjoined tendon is often retracted to gain exposure. How far distal to the tip of the coracoid process does the musculocutaneous nerve typically enter the coracobrachialis muscle?
Explanation
Question 38
When performing a volar (Henry) approach to the proximal radius, which structure must be carefully identified and ligated to safely retract the brachioradialis laterally and the pronator teres medially?
Explanation
Question 39
During a posterior (Kocher-Langenbeck) approach to the acetabulum, the quadratus femoris muscle is carefully preserved or only partially released. This is primarily to protect which of the following structures?
Explanation
Question 40
Which of the following best describes the precise anatomic attachment of the popliteus tendon on the lateral femoral condyle relative to the fibular collateral ligament (FCL)?
Explanation
Question 41
When performing a lateral transpsoas approach to the lumbar spine (LLIF), a surgeon must navigate the lumbar plexus safely. Which nerve lies directly on the anterior surface of the psoas major muscle?
Explanation
Question 42
The recurrent motor branch of the median nerve provides innervation to the thenar muscles. Which of the following is the most common anatomic variation of its course relative to the transverse carpal ligament?
Explanation
Question 43
During a lateral extensile approach for a displaced intra-articular calcaneus fracture, full-thickness flaps are elevated. Which structure is at highest risk of iatrogenic injury during the creation of the inferior and posterior limb corner?
Explanation
Question 44
In an anterior pelvic approach (ilioinguinal), a vascular anastomosis known as the 'corona mortis' may be encountered. This structure typically connects the obturator vessels with which of the following?
Explanation
Question 45
The axillary nerve is at risk during inferior capsular release of the shoulder. It exits the axilla through the quadrangular space. What forms the superior border of this space?
Explanation
Question 46
The lateral ulnar collateral ligament (LUCL) is the primary stabilizer against posterolateral rotatory instability (PLRI) of the elbow. Where does the LUCL typically insert?
Explanation
Question 47
A 25-year-old gymnast presents with ulnar-sided wrist pain. MRI reveals a central tear of the triangular fibrocartilage complex (TFCC). Why is debridement preferred over repair for this specific injury pattern?
Explanation
Question 48
A patient presents with an inability to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. Which nerve is most likely compressed or injured?
Explanation
Question 49
During a posterior approach to the hip, the surgeon must remember the anatomical relationship of the sciatic nerve to the short external rotators. In the majority of the population, the sciatic nerve exits the pelvis through the greater sciatic foramen in what relation to the piriformis muscle?
Explanation
Question 50
In the cervical spine, the vertebral artery typically enters the transverse foramen at which vertebral level?
Explanation
Question 51
Which of the following structures passes anterior to the medial malleolus and is at risk during the placement of the anteromedial portal in ankle arthroscopy?
Explanation
Question 52
In the evaluation of a patient with scapular winging, physical examination reveals medial prominence of the scapula when pushing against a wall. Injury to which nerve is the most likely cause?
Explanation
Question 53
During an open carpal tunnel release, the surgeon must be mindful of the superficial palmar arch. This structure is primarily formed by the continuation of which artery?
Explanation
Question 54
The anterior cruciate ligament (ACL) is composed of two primary bundles. Which statement accurately describes the tension pattern of these bundles during knee range of motion?
Explanation
Question 55
During a posterolateral approach to the ankle for fixation of a posterior malleolar fracture, the internervous plane is developed between the flexor hallucis longus (FHL) and the peroneal muscles. Which nerve is at greatest risk during the superficial dissection of this approach?
Explanation
Question 56
The major blood supply to the body of the talus is derived primarily from which of the following vessels?
Explanation
Question 57
During the anterior (Smith-Petersen) approach to the hip, an internervous plane is utilized. Which of the following describes the correct muscular interval and their respective innervations?
Explanation
Question 58
During a posterior approach to the humerus, the radial nerve is identified. It passes from the posterior compartment to the anterior compartment through the lateral intermuscular septum. At what average distance proximal to the lateral epicondyle does this occur?
Explanation
Question 59
During an ilioinguinal approach for an acetabular fracture, significant hemorrhage occurs while dissecting near the superior pubic ramus. This is most likely due to an injury of an anastomotic vessel connecting which two vascular systems?
Explanation
Question 60
When extending the anterolateral approach to the distal tibia, which of the following neurologic structures is at greatest risk of iatrogenic injury as it crosses the surgical field?
Explanation
Question 61
A 28-year-old volleyball player presents with isolated weakness of external rotation of the shoulder. An MRI reveals a paralabral cyst. If the cyst is located strictly at the spinoglenoid notch, which muscle will show denervation changes on EMG?
Explanation
Question 62
The volar (Henry) approach to the radius utilizes an internervous plane. Proximally, this plane is found between which of the following two muscles?
Explanation
Question 63
To preserve the primary blood supply to the adult femoral head during a posterior approach to the hip, which of the following structures must be carefully protected as it defines the upper limit of the deep dissection?
Explanation
Question 64
A surgeon is placing pedicle screws in the L4 vertebra during a lumbar fusion. A breach of the inferior cortex of the L4 pedicle places which of the following structures at highest immediate risk of injury?
Explanation
Question 65
Placement of an anterior shoulder arthroscopy portal typically requires passing lateral to the coracoid process. If the portal is placed medially to the coracoid by mistake, which structure is at greatest immediate risk of injury?
Explanation
Question 66
During a medial approach to the midfoot, the surgeon encounters the "Master Knot of Henry". This anatomic structure is formed by the crossing of which two tendons?
Explanation
Question 67
While performing an in situ decompression of the ulnar nerve at the elbow, the surgeon releases the aponeurosis connecting the two heads of the flexor carpi ulnaris (FCU). This aponeurotic band is classically known as:
Explanation
Question 68
In an extensile lateral approach for an intra-articular calcaneus fracture, a full-thickness flap is created. Which of the following structures must be intentionally kept within the flap to prevent necrosis and wound complications?
Explanation
Question 69
The anterolateral (Watson-Jones) approach to the hip joint utilizes the interval between the gluteus medius and the tensor fasciae latae. Since both are innervated by the superior gluteal nerve, what anatomical characteristic makes this approach viable?
Explanation
Question 70
During an anterior cervical discectomy and fusion (ACDF), excessive lateral dissection carries the risk of vertebral artery injury. At which cervical level does the vertebral artery typically enter the transverse foramen from the neck?
Explanation
Question 71
During a posterior approach to the knee, the surgeon dissects through the popliteal fossa. From superficial to deep (posterior to anterior), what is the correct order of the major neurovascular structures encountered?
Explanation
Question 72
To safely expose the anterior L4-L5 disc space during an anterior retroperitoneal approach, which of the following vascular structures typically requires ligation and division to allow mobilization of the common iliac vessels?
Explanation
Question 73
When performing a volar Henry approach to the proximal radius, which structure must be ligated to safely mobilize the brachioradialis laterally and the pronator teres medially?
Explanation
Question 74
During a lateral extensile approach to the calcaneus for an intra-articular fracture, the sural nerve is at risk of injury. What is the normal anatomic course of the sural nerve at the level of the lateral malleolus?
Explanation
Question 75
During an ilioinguinal approach to the acetabulum, the surgeon encounters bleeding from the 'corona mortis.' This vascular structure represents an anastomosis between which two vascular systems?
Explanation
Question 76
A patient is undergoing arthroscopic medial meniscus repair using an inside-out technique. Which anatomic structure is at greatest risk of iatrogenic injury when passing sutures through the posterior horn?
Explanation
Question 77
During a direct anterior approach (Smith-Petersen) for total hip arthroplasty, the superficial internervous plane is developed between which two muscles?
Explanation
Question 78
A patient presents with weakness in internal rotation and adduction of the shoulder, specifically lacking the ability to perform latissimus dorsi pull-downs. Which of the following cords of the brachial plexus provides the primary innervation to this muscle?
Explanation
Question 79
In an adult patient, which vessel provides the primary blood supply to the weight-bearing dome of the femoral head?
Explanation
Question 80
During an anterolateral approach to the distal tibia, the superficial peroneal nerve must be identified and protected. At what approximate distance proximal to the lateral malleolus does this nerve typically pierce the deep fascia to become subcutaneous?
Explanation
Question 81
During anterior cervical spine surgery, knowledge of vertebral artery anatomy is crucial. The vertebral artery typically enters the transverse foramen at which cervical level?
Explanation
Question 82
In the anatomic reconstruction of the medial patellofemoral ligament (MPFL), the femoral tunnel placement is highly sensitive. The exact anatomic femoral insertion of the MPFL is located in which relation to bony landmarks?

Explanation
Question 83
During hip arthroscopy, a variety of portals are established. Which nerve is at greatest risk of iatrogenic injury during the placement of the anteroinferior portal?
Explanation
Question 84
When performing an arthroscopic subacromial decompression, brisk bleeding may be encountered from the acromial branch of the thoracoacromial artery. This vessel typically runs in close proximity to which structure?
Explanation
Question 85
A patient presents with an attritional tendon rupture following a distal radius fracture. The ruptured tendon normally passes through the third dorsal extensor compartment. Which tendon is this?
Explanation
Question 86
The internervous plane for the Smith-Petersen (anterior) approach to the hip lies between muscles innervated by which of the following pairs of nerves?
Explanation
Question 87
During a volar Henry approach to the forearm, which of the following vascular structures must be mobilized and its recurrent branches ligated to safely expose the proximal radius?
Explanation
Question 88
Which of the following tendons are contained within the first dorsal compartment of the wrist?
Explanation
Question 89
What nerve is at greatest risk of injury during a standard medial approach to the knee for a medial meniscus repair?
Explanation
Question 90
A 25-year-old male sustains a midshaft humerus fracture and is noted to have a profound wrist drop on examination. The nerve responsible for this deficit passes through which of the following anatomical spaces?
Explanation
Question 91
In the lumbar spine, a central-posterolateral disc herniation at the L4-L5 level will most likely impinge which of the following nerve roots?
Explanation
Question 92
Which ligament is considered the primary static restraint to anterior translation of the talus relative to the tibia in a plantarflexed ankle?
Explanation
Question 93
During an Ilioinguinal approach to the acetabulum, the "lateral window" is bounded medially by which of the following anatomical structures?
Explanation
Question 94
A surgeon is performing a posterolateral (Kocher) approach to the radial head. Maximal pronation of the forearm during this approach is necessary to protect which of the following neural structures?
Explanation
None
