Zancolli Reconstruction for Tetraplegia: Surgical Guide
Key Takeaway
The Zancolli reconstruction is a two-stage surgical technique designed to restore hand function in patients with C6 tetraplegia. The first stage establishes active finger and thumb extension alongside thumb stabilization. The second stage, performed four to six months later, restores active grasp and pinch through synergistic tendon transfers. This evidence-based guide details the biomechanics, step-by-step surgical approaches, and postoperative protocols essential for optimizing functional outcomes in the tetraplegic hand.
INTRODUCTION TO THE ZANCOLLI RECONSTRUCTION
The restoration of upper extremity function in the tetraplegic patient represents one of the most profound interventions in reconstructive orthopedic surgery. For patients with a C6 spinal cord injury, the preservation of active, strong wrist extension—typically mediated by the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB)—provides a critical biomechanical foundation. Eduardo Zancolli pioneered a highly systematic, two-step reconstructive technique designed specifically for this patient population.
The Zancolli reconstruction aims to restore two fundamental upper extremity functions:
1. Step One: Active finger and thumb extension, coupled with thumb stabilization.
2. Step Two: Active finger flexion and thumb flexion (grasp and key pinch).
This staged approach mitigates the risk of antagonistic tendon transfers competing simultaneously, allowing the patient to master the cerebral re-education required for extension before introducing the mechanics of flexion.
INDICATIONS AND PATIENT SELECTION
Patient selection is paramount. The Zancolli procedure is primarily indicated for patients classified with C6 level function. In the context of the International Classification Scheme for tetraplegia, these patients typically fall into Groups 3 through 5, where wrist extensors are grade 4 or better, but active digital flexion and extension are absent.
The International Classification Scheme in Tetraplegia
To appropriately plan a Zancolli reconstruction, the surgeon must classify the patient's retained motor function below the elbow (muscle grade 4 or better):
- Group 0: No muscles below elbow grade 4. (Options: Elbow extension via Moberg).
- Group 1: Brachioradialis (BR). (Options: Elbow extension; key grip).
- Group 2: Extensor carpi radialis longus (ECRL). (Options: Elbow extension, key grip).
- Group 3: Extensor carpi radialis brevis (ECRB). (Primary indication for Zancolli two-stage).
- Group 4: Pronator teres (PT). (Primary indication for Zancolli two-stage).
- Group 5: Flexor carpi radialis (FCR). (Primary indication for Zancolli two-stage).
- Group 6: Finger extensors. (Options: Modified House procedure).
- Group 7: Thumb extensor. (Options: House two-stage).
- Group 8: Partial finger flexors. (Options: Zancolli two-stage).
- Group 9: Lacks only intrinsics. (Options: Opponens transfer).
Clinical Pearl: Always assess for the presence of an accessory radial wrist extensor (extensor carpi radialis tertius) during the first stage of the reconstruction. If present, it serves as an invaluable synergistic motor unit for thumb flexion in the second stage.
BIOMECHANICS AND PREOPERATIVE PLANNING
The success of the Zancolli reconstruction relies heavily on the tenodesis effect and the precise tensioning of transferred muscle-tendon units.
Donor Muscle Evaluation
- Brachioradialis (BR): Utilized in Step 1 for digital extension. The BR has a high cross-sectional area but limited excursion (approximately 30 mm). Extensive proximal dissection is required to maximize its excursion.
- Extensor Carpi Radialis Longus (ECRL): Utilized in Step 2 for digital flexion. It is synergistic with finger flexion, making motor re-education intuitive.
- Extensor Carpi Radialis Brevis (ECRB): Must be preserved as the primary wrist extensor to maintain the tenodesis effect.
Joint Stabilization Principles
In the paralyzed hand, transferring a tendon across an unstable joint will result in joint collapse rather than the intended distal motion. Therefore, the thumb carpometacarpal (CMC) joint or metacarpophalangeal (MCP) joint must be stabilized during Step 1 to provide a rigid post against which the transferred tendons can act.
SURGICAL TECHNIQUE: FIRST STEP (EXTENSION PHASE)
The primary objectives of the first stage are to provide active extension of the fingers and thumb, and to stabilize the thumb column to prepare for future pinch reconstruction.
1. Incisions and Exposure
Three primary incisions are typically required for the first stage. A long, curved radial incision is utilized to harvest the brachioradialis and expose the extensor compartments.
2. Thumb Stabilization
The thumb must be stabilized to prevent collapse during pinch. This is achieved either through CMC arthrodesis or MCP capsuloplasty, depending on the patient's specific joint laxity and preoperative assessment.
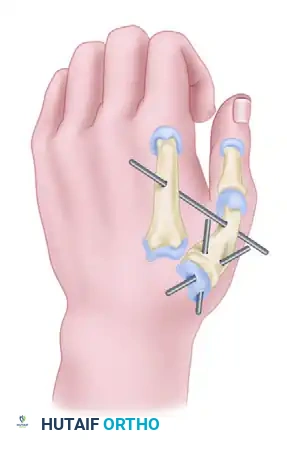
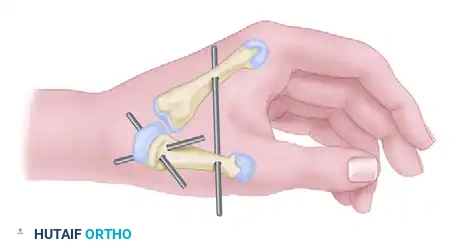
Option A: Carpometacarpal (CMC) Arthrodesis
The CMC joint is exposed and the articular cartilage is denuded. The joint is fused in a highly specific functional position:
* 45 degrees of palmar abduction
* 20 degrees of radial abduction
Fixation is achieved using two crossed Kirschner wires across the CMC joint. A third Kirschner wire is placed between the first and second metacarpals to rigidly fix the relationship of the first web space during healing.

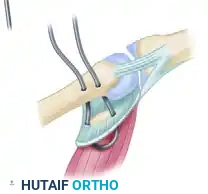
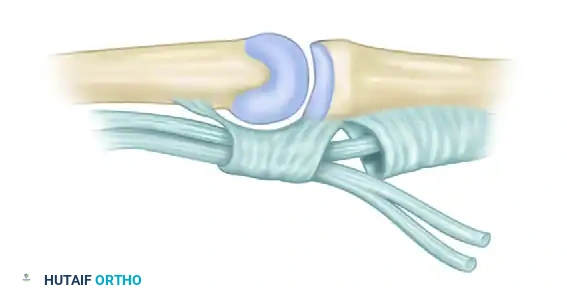
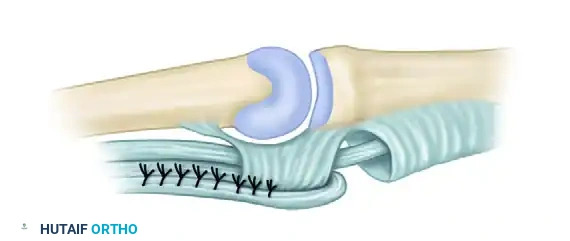
Option B: Metacarpophalangeal (MCP) Volar Plate Capsuloplasty
If the MCP joint demonstrates a tendency to hyperextend (a common finding in the paralyzed thumb), a volar plate capsuloplasty is indicated.
The volar plate and its associated radial sesamoid are advanced and sutured directly to the neck of the first metacarpal. This creates a robust volar tether that prevents hyperextension while allowing flexion.

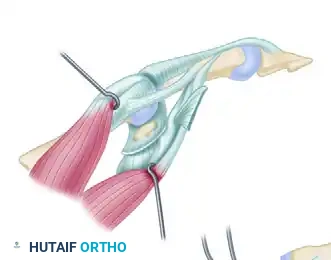
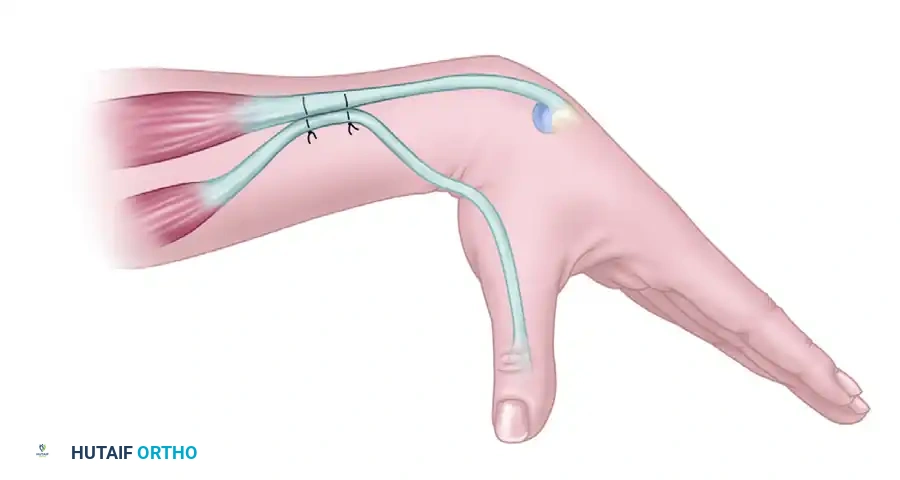
3. Tendon Transfer: Brachioradialis to EDC and EPL
The brachioradialis (BR) is mobilized proximally to its fascial origin to maximize excursion. It is then transferred to the extensor digitorum communis (EDC) and the extensor pollicis longus (EPL).
Surgical Warning: Adhesions at the graft site are a primary cause of transfer failure. Minimize adhesions by excising a portion of the proximal aspect of the dorsal carpal ligament and by placing the tendon sutures as far proximally as possible in the forearm.
Tensioning the Transfer
Tensioning is the most critical step of the procedure.
* The elbow must be maintained at 60 degrees of flexion during tensioning.
* Slightly more tension is applied to the EDC than to the EPL. This is because subsequent elbow extension will naturally reduce the tension on the EDC due to the origin of the BR.

Verification of Correct Tension:
The tension is deemed correct when full passive finger flexion can be obtained with maximal wrist extension and the elbow at 60 degrees of flexion. Conversely, passive wrist flexion should result in full extension of the MCP joints and the interphalangeal (IP) joint of the thumb.
4. Management of MCP Hyperextension: The Zancolli Lasso
If the digital MCP joints tend to hyperextend (clawing), intrinsic tenodesis is required. While this can be performed in Step 2, it is often integrated into Step 1. The Zancolli lasso procedure is the gold standard for this indication.
Through a transverse palmar incision just proximal to the MCP flexion creases, the flexor digitorum sublimis (FDS) tendons and the A1/proximal A2 pulleys are exposed.
1. The FDS tendons are divided as far distally as possible.
2. The two slips of each FDS tendon are routed out through the distal margins of the A1 pulleys.
3. They are looped back and sutured to themselves.
Lasso Tensioning: Adjust the tension so that with the wrist held in 40 degrees of flexion, the MCP joints extend exactly to 0 degrees (neutral).
POSTOPERATIVE CARE: FIRST STEP
Meticulous postoperative immobilization is required to protect the transfers and joint fusions.
* Immobilization: The hand and elbow are immobilized in a long-arm splint for 4 weeks. The wrist is positioned in 45 degrees of extension, MCP joints in 20 degrees of flexion, and IP joints in extension.
* Thumb Protection: After the initial 4 weeks, the thumb fusion/capsulodesis is protected with a localized splint for an additional 4 weeks.
* Rehabilitation: At 3 to 4 weeks, muscle re-education begins. The patient is taught to initiate active MCP extension by utilizing elbow flexion (firing the BR). Passive finger flexion exercises are mandatory to prevent extension contractures.
* Precautions: The transfers must be protected from heavy resistance for a minimum of 3 months.
SURGICAL TECHNIQUE: SECOND STEP (FLEXION PHASE)
Four to six months following the first step, once the patient has successfully integrated active extension into their motor patterns, the hand is ready for the second step. The objective here is to provide active finger flexion and active thumb flexion (key pinch).
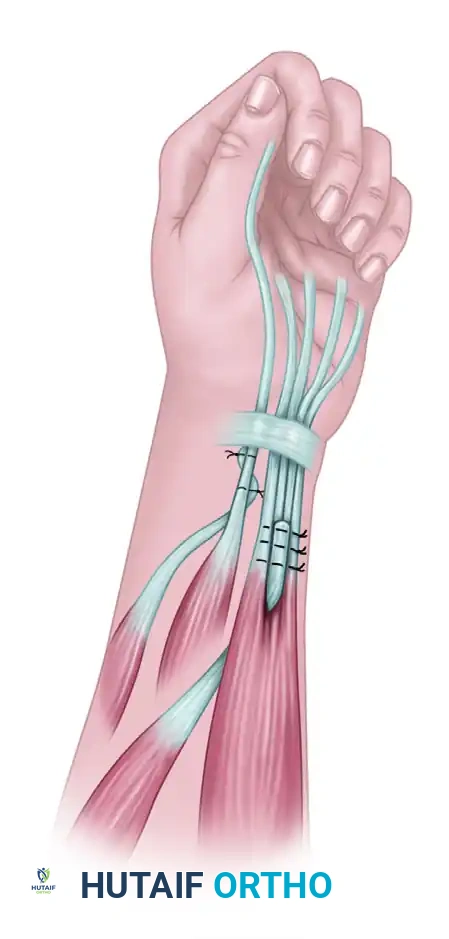
1. Tendon Transfer: ECRL to FDP
The extensor carpi radialis longus (ECRL) is harvested and transferred to the flexor digitorum profundus (FDP) tendons.
* The ECRL is routed volarly.
* It is woven into the FDP tendons using a Pulvertaft weave.
* Tensioning: Slightly more tension is applied to the more ulnar digits to recreate the natural cascade of the hand and ensure a strong power grip.
2. Activation of the Flexor Pollicis Longus (FPL)
Restoring thumb flexion is critical for key pinch. Zancolli described several methods for activating the FPL, depending on the available local anatomy.
Option A: Extensor Carpi Radialis Tertius (Preferred)
If a supernumerary radial wrist extensor (ECR tertius) was identified during Step 1, it is the motor unit of choice. It is transferred directly to the FPL. This is a highly synergistic transfer that allows for independent, conscious control of thumb flexion.
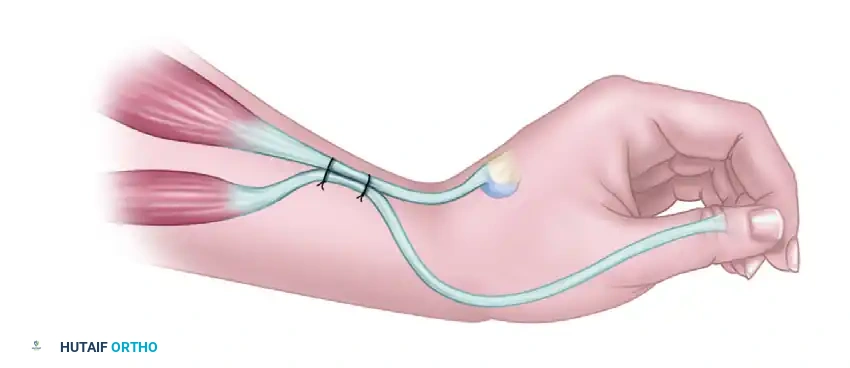
Option B: ECRB to FPL Side-to-Side Tenodesis
If the ECR tertius is absent, the FPL can be activated by suturing it side-to-side to the active extensor carpi radialis brevis (ECRB).
* Biomechanics: Thumb flexion occurs automatically with active wrist extension (key pinch). Conversely, thumb extension occurs with wrist flexion (release).
Tensioning the ECRB-FPL Tenodesis:
With the wrist placed in complete passive extension, the FPL tendon is pulled until the thumb firmly rests against the lateral aspect of the index finger (the key pinch position). The FPL is sutured to the ECRB at this exact tension.
Option C: Passive Tenodesis (Moberg Style)
A third option, if active motor units are unavailable, is a passive tenodesis of the FPL to the volar aspect of the distal radius. This relies entirely on the natural tenodesis effect of wrist extension to drive the thumb into the index finger.
POSTOPERATIVE CARE: SECOND STEP
The postoperative protocol for the flexion phase focuses on protecting the volar transfers while preventing stiffness.
* Immobilization: The arm is immobilized for 4 weeks in a long-arm splint.
* Positioning: Unlike Step 1, the wrist is held in neutral, the thumb is positioned resting between the index and middle fingers, and the fingers are gently flexed.
* Rehabilitation: Active and passive exercises commence at 4 weeks, focusing on synergistic muscle re-education (e.g., extending the wrist to flex the digits).
* Precautions: As with the first stage, the transfers must be protected from heavy use and sudden forceful stretching for 3 months.
COMPLICATIONS AND PITFALLS
Surgeons undertaking the Zancolli reconstruction must be vigilant regarding several potential pitfalls:
1. Over-tensioning the BR to EDC: If the EDC is excessively tight, the patient will lose the ability to passively flex the fingers, destroying the grasp reconstructed in Step 2. Always tension with the elbow at 60 degrees of flexion.
2. Failure of Thumb Stabilization: If the CMC fusion fails to unite, or the MCP capsulodesis stretches out, the thumb will collapse into hyperextension during key pinch, rendering the FPL transfer ineffective. Meticulous joint preparation and rigid K-wire fixation are mandatory.
3. Adhesion Formation: The forearm is prone to severe scarring. Handling tissues with atraumatic technique, ensuring robust hemostasis, and placing tendon weaves in healthy, well-vascularized beds (away from the extensor retinaculum) minimizes this risk.
CONCLUSION
The Zancolli two-step reconstruction remains a cornerstone in the surgical rehabilitation of the tetraplegic upper extremity. By systematically addressing extension and joint stability in the first stage, and synergistic flexion in the second stage, the orthopedic surgeon can reliably restore functional independence, grasp, and key pinch to patients with C6 spinal cord injuries. Strict adherence to biomechanical principles, precise tensioning, and rigorous postoperative rehabilitation are the absolute prerequisites for success.
You Might Also Like


