Management of Chronic Unreduced Shoulder Dislocations: A Comprehensive Surgical Guide

Key Takeaway
The management of chronic unreduced shoulder dislocations requires a highly individualized approach, balancing patient functional demands with complex pathoanatomy. Treatment options range from benign neglect in low-demand patients to complex open reduction, tendon transfers, and arthroplasty. Successful intervention demands a thorough understanding of capsular contractures, humeral head impression defects, and altered neurovascular anatomy to restore glenohumeral stability and optimize functional outcomes.
INTRODUCTION TO CHRONIC UNREDUCED SHOULDER DISLOCATIONS
The management of an old, unreduced dislocation of the shoulder presents one of the most formidable challenges in orthopedic surgery. Defined generally as a dislocation that has been neglected or unrecognized for greater than three to four weeks, the chronic unreduced shoulder is characterized by profound pathoanatomic changes. The glenoid fossa becomes obliterated by dense fibrous scar tissue, the joint capsule undergoes severe contracture and bowstringing, and the rotator cuff musculature shortens and retracts. Furthermore, the constant pressure of the glenoid rim against the dislocated humeral head inevitably leads to progressive impression fractures—the Hill-Sachs lesion in anterior dislocations, and the reverse Hill-Sachs (McLaughlin) lesion in posterior dislocations.

Clinical Pearl: Posterior dislocations are notoriously missed on initial presentation. As demonstrated in the radiographs above, an anteroposterior (AP) radiograph may show only subtle changes, such as the "lightbulb sign" or loss of the normal elliptical overlap of the humeral head and glenoid. An axillary lateral radiograph is absolutely mandatory to confirm the posterior displacement of the humeral head and to quantify the extent of the anterior impression defect where the posterior glenoid rim is incarcerated.
Treatment options for chronic unreduced dislocations span a wide spectrum, including benign neglect (no treatment), closed reduction (with or without arthroscopic assistance), open reduction, hemiarthroplasty, and total shoulder arthroplasty. The decision-making process must meticulously account for the patient's physiological age, functional demands, medical comorbidities, the duration of the dislocation, and the precise size of the humeral head defect.
NON-OPERATIVE MANAGEMENT: THE ROLE OF BENIGN NEGLECT
It is a critical clinical axiom that not all patients with old unreduced dislocations of the shoulder require surgical intervention. In a carefully selected subset of patients, the upper extremity remains surprisingly functional despite limited motion and mild discomfort.
If a patient is elderly, highly inactive, or presents with severe medical comorbidities that render them a poor surgical risk, the option of no surgical treatment should be strongly considered.
Biomechanical Implications of Neglected Dislocations
The functional deficit of an untreated dislocation depends heavily on the direction of the displacement:
* Untreated Posterior Dislocations: Patients with unreduced posterior dislocations generally exhibit better functional tolerance than those with anterior dislocations. In a posterior dislocation, the arm rests at the side in a position of internal rotation. This biomechanical posture allows the patient to perform essential activities of daily living, such as reaching their face to feed themselves, reaching their head for grooming, and reaching the rear of their body for hygiene.
* Untreated Anterior Dislocations: Conversely, the arm of a patient with an unreduced anterior dislocation is mechanically locked away from the body in a position of fixed external rotation and slight abduction. This renders the extremity highly dysfunctional, making it exceedingly difficult to reach the face and virtually impossible to reach the back.
CLOSED REDUCTION: INDICATIONS AND LIMITATIONS
Attempting a closed manipulative reduction of a chronic shoulder dislocation is fraught with difficulty and potential peril. As emphasized by numerous academic authorities, closed reduction should never be undertaken without a comprehensive evaluation of the patient’s age, the degree of humeral osteoporosis, the vascular status of the upper extremity, and the exact duration of the dislocation.
Pathoanatomic Barriers to Closed Reduction
While a few isolated cases of successful closed reduction in shoulders dislocated for more than four weeks exist in the literature, they are the exception rather than the rule. Beyond the three-to-four-week mark, several insurmountable barriers typically develop:
1. Soft Tissue Contracture: The capsule and surrounding musculature lose their elasticity.
2. Glenoid Fibrosis: The empty glenoid cavity fills with dense, organized fibrous tissue, preventing the humeral head from seating.
3. Rotator Cuff Retraction: The rotator cuff muscles shorten, acting as a tether against reduction.
Surgical Warning: It is generally unwise and potentially dangerous to attempt closed reduction for a shoulder that has been dislocated for more than 3 to 4 weeks, or for a shoulder with an impression defect involving more than 20% of the articular surface.
Technique and Vascular Risks
If closed reduction is deemed appropriate, it must be performed under general anesthesia with complete neuromuscular blockade to ensure absolute muscle relaxation. The reduction maneuver must utilize minimal, sustained traction. Leverage techniques must be strictly avoided to prevent iatrogenic fractures of the osteoporotic proximal humerus.
In elderly patients, particularly those with peripheral arterial disease or atherosclerosis, the axillary artery becomes tethered by scar tissue and the pectoralis minor. Forceful manipulation carries a catastrophic risk of axillary artery rupture.
Post-Reduction Immobilization (Rowe and Zarins Method)
If closed reduction is successful, the shoulder must be immobilized for a minimum of 6 weeks to allow capsular healing and prevent immediate recurrence. The position of immobilization is dictated by the direction of the initial instability, as described by Rowe and Zarins:
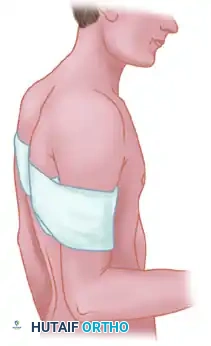
- Posterior Dislocations: The arm is immobilized posterior to the coronal plane of the body to prevent the humeral head from translating posteriorly.
- Anterior Dislocations: The arm is immobilized anterior to the coronal plane of the body to relax the anterior capsule and prevent anterior translation.
OPEN REDUCTION: SURGICAL STRATEGIES AND TECHNIQUES
When closed reduction is contraindicated or fails, open reduction becomes necessary. The surgeon must be prepared to confront two primary obstacles during open reduction:
- Difficulty in Achieving Reduction: This is caused by severe fibrosis, muscle shortening, capsular contracture, bowstringing of the capsule across the glenoid, scar tissue filling the glenoid fossa, and the mechanical block of the articular impression defect.
- Difficulty in Maintaining Reduction: Once reduced, the joint is often grossly unstable due to the large humeral head defect engaging the glenoid rim.
Management of the Humeral Head Defect
Preventing recurrent dislocation caused by the humeral head defect is paramount. This challenge is encountered far more frequently in old unreduced posterior dislocations (reverse Hill-Sachs lesions) than in anterior dislocations.
The McLaughlin Procedure and Neer Modification
For anteromedial impression defects of the humeral head (seen in posterior dislocations), McLaughlin introduced the concept of transferring the subscapularis tendon into the defect. This effectively fills the void, preventing the defect from engaging the posterior glenoid rim during internal rotation.
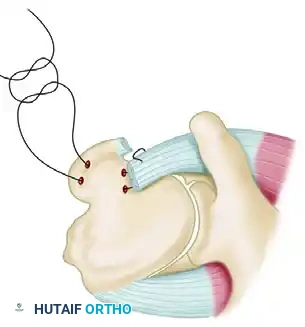
- McLaughlin Technique: The subscapularis tendon is detached from its insertion, and two drill holes are placed transversely through the area of the anterior humeral defect. A mattress suture is passed through the freed tendon and the drill holes, tying it securely to fix the tendon directly into the defect.
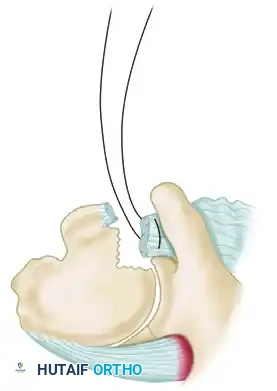
- Neer Modification: Neer advanced this concept by performing an osteotomy of the lesser tuberosity. The subscapularis tendon, with its attached bone block from the lesser tuberosity, is mobilized and rigidly fixed into the anterior defect using a cancellous screw. This provides superior bone-to-bone healing compared to tendon-to-bone healing.
Surgical Approaches Based on Defect Size (Rockwood Criteria)
Rockwood established a highly regarded algorithm for the surgical approach to old unreduced posterior dislocations based on the size of the anteromedial humeral head defect:
* Defect < 15%: A posterior approach is recommended to address the posterior capsular redundancy and achieve reduction.
* Defect > 15%: An anterior reconstruction through a standard deltopectoral approach is mandated to address the large impression defect via a McLaughlin or Neer transfer.
* Note: Superior and anteromedial approaches have also been advocated by some authors for specific complex presentations.
Posterior Capsular Shift (Elshewy Technique)
For chronic posterior dislocations with moderate head defects (less than 25%), Elshewy et al. demonstrated good pain relief and functional improvement utilizing an open reduction combined with a posterior capsular shift, originally described by Neer.




This technique involves a T-shaped incision of the posterior capsule. After the joint is reduced and cleared of scar tissue, the inferior capsular flap is shifted upward to eliminate redundancy. The superior flap is then brought down to overlap the inferior flap, robustly reinforcing the posterior repair and preventing posterior subluxation.
Humeral Rotational Osteotomy
In highly selected cases, a proximal humeral rotational osteotomy can be utilized for locked posterior shoulder dislocations. By rotating the humerus, the impression defect is moved out of the functional arc of motion, preventing it from engaging the glenoid.
Strict criteria must be met for this procedure:
1. The articular cartilage must be healthy and viable.
2. The humeral head defect must involve less than 40% of the articular surface.
3. The patient must be cognitively and physically capable of participating in a rigorous, active rehabilitation program.
INTERNAL FIXATION ADJUNCTS
In cases where severe capsular deficiency or massive bone loss renders the reduction acutely unstable despite soft tissue reconstruction, temporary internal fixation across the glenohumeral joint may be a necessary adjunct.
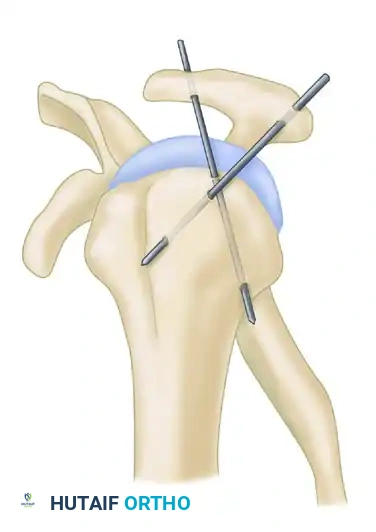

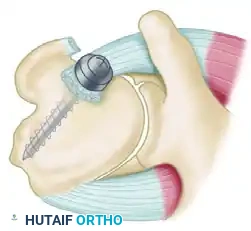
- Swiss Screw Fixation: As described by Neviaser, a large Swiss screw can be driven through the acromion directly into the humeral head to maintain reduction.
- Kirschner Wire Fixation: The Wilson and McKeever method utilizes two heavy, crossed Kirschner wires driven through the acromion into the humeral head to stabilize the joint after the reduction of a posterior dislocation.
- Coracoid Transfer: Goga described using K-wire fixation for anterior dislocations in conjunction with a Latarjet-type transfer of the coracoid process to the anterior glenoid to provide a bony block.
Clinical Pearl: While internal fixation can salvage an unstable reduction, it carries risks of hardware migration, articular cartilage damage, and pin-tract infections. Rowe and Zarins argued that transfixing the joint is often unnecessary if the arm is strictly immobilized in the correct spatial plane (anterior to the coronal plane for anterior dislocations; posterior to the coronal plane for posterior dislocations).
NEUROVASCULAR CONSIDERATIONS: PROTECTING THE AXILLARY NERVE
The altered anatomy of a chronic dislocation places major neurovascular structures at extreme risk during surgical dissection. The axillary nerve is particularly vulnerable.
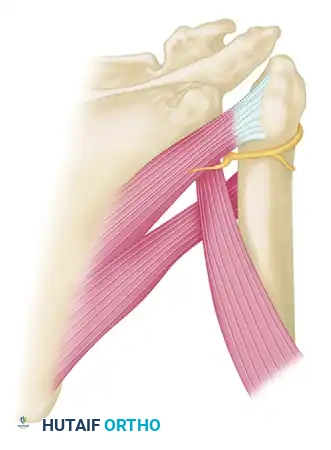
In chronic anterior dislocations, the subscapularis muscle is displaced anteriorly and inferiorly. This creates a severe traction injury to the axillary nerve. The nerve becomes entrapped and tethered—held above by the brachial plexus cords and held below where it wraps tightly behind the surgical neck of the humerus through the quadrangular space.
During the anterior approach, the surgeon must meticulously identify and protect the axillary nerve at the inferior border of the subscapularis before any capsular release or tendon transfer is performed. Aggressive retraction in this scarred bed can easily result in permanent denervation of the deltoid muscle.
POSTOPERATIVE REHABILITATION AND PROGNOSIS
The postoperative management of a surgically treated chronic shoulder dislocation requires a delicate balance between protecting the repair and preventing devastating stiffness.
Immobilization in the appropriate plane (as dictated by the direction of instability) is typically maintained for 4 to 6 weeks. Following this, a carefully phased rehabilitation program is initiated, focusing first on passive range of motion, progressing to active-assisted motion, and finally to strengthening.
Managing Patient Expectations
It is imperative that the surgeon has a frank discussion with the patient regarding functional outcomes prior to surgery. Full function of the shoulder is rarely, if ever, regained after operations for chronic unreduced dislocations.
Motion will almost certainly be permanently limited, particularly in abduction and external rotation. The primary goals of surgery are the relief of pain, the restoration of basic glenohumeral stability, and the return of the hand to a functional position in space. While the patient should not expect a full recovery to pre-injury levels, a meaningful and significant improvement in overall shoulder function and quality of life should be expected.
You Might Also Like

