Comprehensive Surgical Management of Syndactyly and Apert Syndrome Hand Deformities

Key Takeaway
Syndactyly release utilizing the Skoog technique employs matching volar and dorsal proximally based V-shaped flaps to reconstruct the web space while minimizing scar contracture. In complex cases like Apert syndrome, surgical reconstruction prioritizes creating a functional, three-fingered hand with an opposable thumb. Early release of border digits and strategic full-thickness skin grafting are critical to optimizing biomechanical outcomes and preventing angular deformities in the growing pediatric hand.
Introduction to Complex Syndactyly and Acrocephalosyndactyly
Syndactyly is one of the most common congenital hand anomalies, presenting either as an isolated finding or as a component of a complex syndromic condition. The primary goal of surgical intervention is to establish independent digital motion, optimize prehensile function, and prevent secondary angular deformities during skeletal growth. Among the most challenging presentations of complex syndactyly is Apert syndrome (acrocephalosyndactyly), a rare and intricate condition requiring a highly staged, multidisciplinary reconstructive approach.
This comprehensive guide details the Skoog technique for syndactyly release—utilizing matching volar and dorsal proximally based V-shaped flaps—and outlines the specialized surgical protocols required for managing the severely deformed hand in Apert syndrome.
Apert Syndrome: Pathoanatomy and Clinical Evaluation
Described by Eugène Apert in 1906, Apert syndrome is a rare congenital disorder (incidence of approximately 1 in 200,000 live births) characterized by craniosynostosis, severe midface hypoplasia, and complex, symmetrical syndactylies of the hands and feet. The condition is driven by a single-gene mutation (typically the FGFR2 gene) and can be inherited in an autosomal dominant fashion, though most cases arise from sporadic mutations.
Blank classified Apert syndrome into two primary categories:
* True (Typical) Apert Syndrome: Characterized by multiple, complex syndactylies involving both soft tissue and bone.
* Atypical Apert Syndrome: Presenting with only partial or simple syndactylies.
Craniofacial and Systemic Manifestations
At birth, patients exhibit a high, broad forehead with a flattened occiput due to premature fusion of the coronal sutures. The orbits are shallow, leading to widely set eyes (hypertelorism) with the outer canthus positioned lower than the inner canthus. The maxilla is severely shortened and hypoplastic, while the lower jaw appears prominent.
Clinical Pearl: While mental retardation is common in Apert syndrome, it is not universal. Early cranial vault remodeling to relieve intracranial pressure is paramount and takes absolute priority over hand reconstruction. Hand surgery should never be performed simultaneously with major craniofacial procedures. Associated visceral abnormalities (cardiac, genitourinary) must also be ruled out preoperatively.
Upton’s Classification of the Apert Hand
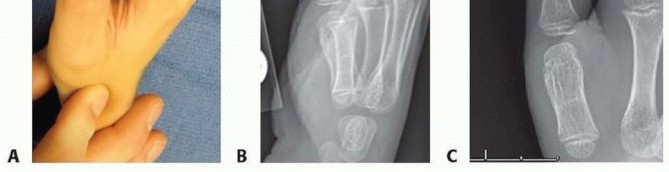
The hand deformities in Apert syndrome are typically symmetrical and severely restrict function. The untreated hand operates in a "spoon-like" fashion, relying on a crude two-handed scoop or a lateral thumb-to-index prehensile pattern. Upton classified these hands into three distinct types based on severity:
- Type 1 ("Spade Hand"): The thumb is separate and mobile, but there is complete, complex syndactyly of the index, long, ring, and small fingers.
- Type 2 ("Spoon Hand"): Syndactyly involves all digits, including the thumb. The hand is concave or spoon-shaped with a tapering terminal end. There is complex syndactyly of the index, long, and ring fingers, often sharing a single conjoined nail. The small finger typically exhibits complete simple syndactyly with the ring finger. Digital motion is severely limited due to symphalangism (incomplete joint development), and the digits are globally shortened.
- Type 3 ("Rosebud Hand" or "Hoof Hand"): The most severe form, featuring complex syndactyly with distal osseous synostosis between the thumb and index finger. A broad, conjoined nail overlies the thumb, index, long, and ring fingers.

Diagnostic Distinction: The presence of exactly five digits in Apert syndrome distinguishes it from Carpenter syndrome (acrocephalopolysyndactyly), which presents with polydactyly. Additionally, Apert patients frequently exhibit shortened upper extremities with limited elbow motion (radiohumeral synostosis).
Principles of Surgical Management and Timing
The overarching goal of reconstructive surgery in Apert syndrome is to create a functional, three-fingered hand with a sensate, opposable thumb.
Flatt’s Reconstructive Protocol
Surgical management should adhere to the staged protocol outlined by Flatt, prioritizing the release of border digits to prevent growth tethering and angular deformity.
- Timing by Age: In children younger than 2 years, bilateral simultaneous reconstructive procedures are permissible, as infants are not yet dependent on self-care. In older children, surgery must be staged, reconstructing only one hand at a time to preserve independence in activities of daily living.
- Border Digit Release: The border digits (thumb and small finger) must be released before 1 year of age. Early release prevents the shorter digits from tethering the longer adjacent digits, which would otherwise lead to severe flexion and deviation contractures.
- Thumb Management: If the thumb is not incorporated into the complex syndactyly mass, a simple four-part Z-plasty is utilized to deepen the first web space.
- Central Ray Deletion: For the central complex syndactyly mass, Flatt recommends the release of the central syndactylies combined with the deletion (ray amputation) of the middle finger at the metacarpophalangeal (MCP) joint. This strategic deletion provides the necessary local skin coverage for the adjacent digits and ensures good sensibility.
Surgical Warning: Ray amputation of the long finger combined with ulnar transposition of the index finger is strictly not recommended. Flatt observed that this specific transposition leads to progressive, severe angular deformities in the Apert hand.
The Skoog Technique: Syndactyly Release with Matching V-Shaped Flaps
For simple and complex syndactylies, the Skoog technique provides a robust, biomechanically sound method for web space reconstruction. It utilizes matching volar and dorsal proximally based V-shaped flaps to recreate the commissure, supplemented by full-thickness skin grafts (FTSG) to cover the remaining digital defects.
Preoperative Planning and Flap Design
Meticulous flap design is the most critical step in preventing postoperative web creep and scar contracture.
- Incision Outlining: Using a sterile skin marker, outline the incisions on the dorsal and volar aspects of the conjoined fingers. The flaps must be designed so that, when mobilized, they cover the majority of the denuded side of one finger entirely without tension.
- Irregular Borders: To prevent linear scar contracture (which leads to flexion deformities), design the free borders of the flaps to be irregular. Incorporate small triangular points precisely at the level of the proximal and distal interphalangeal joints.

- Matching Key Points: To ensure the dorsal and volar flaps interdigitate perfectly, first outline the incision on one side (e.g., dorsal). Then, establish the corresponding key points for the volar incision by pushing straight needles vertically through the web space from dorsal to volar.
Surgical Dissection
- Exsanguination and Tourniquet: Elevate the limb, exsanguinate with an Esmarch bandage (or elevate for 3 minutes in small infants), and inflate the pneumatic tourniquet to the appropriate pediatric pressure.
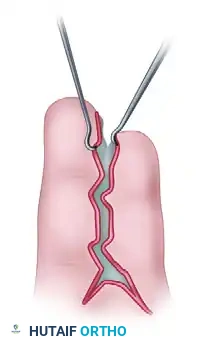
- Flap Elevation: Raise the dorsal and volar flaps, which consist primarily of the skin forming the abnormal web.
- Tissue Preservation: It is imperative to preserve all subcutaneous tissue to maintain venous drainage. Dissect under loupe magnification, taking extreme care to identify and protect the digital nerves and common digital arteries.
Surgical Warning: The bifurcation of the common digital artery may be located abnormally distal in syndactyly. If the bifurcation extends beyond the planned web space, the artery to one digit must be carefully ligated and divided to allow the web to drop proximally. Never ligate the digital arteries to both sides of a single digit.
- Hemostasis: Release the tourniquet prior to closure to ensure adequate perfusion of the flaps and digits, and to achieve meticulous bipolar hemostasis.
Web Space Reconstruction and Grafting
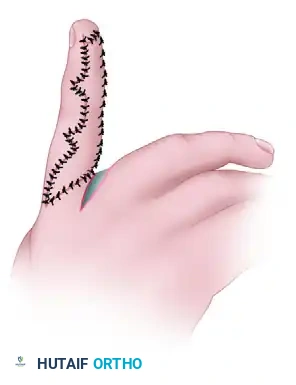
- Commissure Creation: Inset the proximally based triangular flaps to reconstruct the new web space. The dorsal flap typically drops into the web, interdigitating with the volar flap to create a smooth, U-shaped commissure.

- Primary Closure: On one finger, close the interdigitating flaps as planned. A small residual defect will remain at the dorsomedial aspect of the base of this finger.
- Full-Thickness Skin Grafting (FTSG): Obtain a full-thickness skin graft from the inguinal region (the groin crease provides excellent, hairless skin with minimal donor site morbidity).
- Graft Application: Make a precise template of the denuded area on the adjacent finger and the newly formed web. Defat the FTSG meticulously, and carefully suture the graft into place using fine absorbable sutures (e.g., 5-0 or 6-0 chromic gut or fast-absorbing plain gut).

Clinical Pearl: If more than two fingers are involved in a syndactyly mass, never separate both sides of a single finger during the same surgical stage. Doing so risks catastrophic vascular compromise and digital necrosis. Stage the procedures, separating only one side of a digit at a time.
Advanced Thumb Reconstruction in Apert Syndrome
When the thumb is severely angulated or involved in a complex synostosis (Type 3), specialized reconstructive techniques are required to establish opposition and pinch kinematics.
- Dao’s Technique: For radially angulated thumbs, Dao recommends releasing the abnormal insertion of the abductor pollicis brevis (APB) tendon from the distal phalanx and reinserting it into the proximal phalanx. This is combined with the excision of the ulnar prominence of the metacarpal head and longitudinal Kirschner wire (K-wire) pinning of the MCP and IP joints to maintain alignment.
- Oishi and Ezaki’s Technique: This approach involves releasing the abnormal APB insertion, performing an opening or closing wedge osteotomy of the proximal phalanx to correct the angular deformity, and utilizing a V-Y advancement flap on the radial side of the thumb to relieve skin tension.
Simultaneously, any synostosis between the ring and small metacarpals should be released during the time of digital separation to optimize the transverse metacarpal arch.
Postoperative Protocol and Rehabilitation
The success of a syndactyly release relies heavily on meticulous postoperative immobilization and graft protection.
- Immediate Postoperative Dressing:
- Apply a non-adherent layer (e.g., Xeroform gauze) directly over the skin grafts and suture lines.
- Spread the fingers widely and place saline-moistened cotton or fluffed gauze precisely between the digits, pressing it gently to fit the contours of the new web space and fingers. This acts as a stent to prevent hematoma beneath the graft.
- Wrap the hand in dry gauze and cast padding (Webril).
- Apply a well-molded plaster or fiberglass splint. In pediatric patients, the splint must extend proximal to the elbow (long-arm cast) with the elbow flexed at 90 degrees to prevent the child from slipping out of the dressing.
- Elevation: The operated limb must be strictly elevated for at least 3 to 5 days postoperatively to minimize edema and venous congestion.
- First Dressing Change: The initial dressing is left undisturbed for 10 to 14 days. In young children, this first dressing change and suture removal (if non-absorbable sutures were used) should be performed under general anesthesia or deep sedation in the operating room to prevent trauma to the newly taken grafts.
- Subsequent Care: Following the first dressing change, a lighter protective bandage or custom thermoplastic spacer splint is maintained for an additional 10 to 14 days.
- Rehabilitation: Gradual resumption of normal activities is allowed after 4 weeks. Occupational therapy is critical, focusing on scar massage, silicone gel sheeting to prevent hypertrophic scarring, and active range-of-motion exercises to maximize prehensile function.
Complications and Surgical Pitfalls
- Web Creep: The most common long-term complication, characterized by the distal migration of the web space as the child grows. This is minimized by using proximally based, tension-free flaps and full-thickness (rather than split-thickness) skin grafts.
- Graft Failure: Usually secondary to hematoma formation, inadequate immobilization, or infection. Meticulous hemostasis and the use of a wet-cotton stent dressing are preventative.
- Vascular Compromise: Releasing both sides of a digit simultaneously or aggressively dissecting the distal bifurcation of the common digital artery can lead to digital ischemia. Always stage multi-digit syndactylies.
- Angular Deformity: Failure to release border digits early (before 1 year of age) will result in the shorter digit tethering the longer digit, causing irreversible joint contractures and skeletal deviation.
📚 Medical References
- syndactyly release, J Hand Surg 14B:201, 1989.
- Apert Syndrome Al-Qattan MM: The use of split thickness skin grafts in the correction of Apert’s syndactyly, J Hand Surg 26B:8, 2001.
- Apert E: De l’acrocephalosyndactylie, Bull Mem Soc Med Hôp Paris 23:1310, 1906.
- Bauer TB, Tondra JM, Trusler HM: Technical modifi cation in repair of syndactylism, Plast Reconstr Surg 17:385, 1956.
- Blank CE: Apert’s syndrome: a type of acrocephalosyndactyly: observations on a British series of thirty-nine cases, Ann Hum Genet 24:151, 1960.
- Dao KD, Shin AY, Kelley S, et al: Synostosis of the ring-small fi nger metacarpal in Apert acrosyndactyly hands: incidence and treatment, J Pediatr Orthop 21:502, 2001.
- Dao KD, Shin AY, Kelley S, et al: Thumb radial angulation correction without phalangeal osteotomy in Apert’s syndrome, J Hand Surg 27A:125, 2002.
- [Flatt AE: The care of congenital hand anomalies, St Louis, 1977, Mosby.
Preaxial Polydactyly Al-Aithan B, Al-Blaihed L, Mahmoud S, et al:](https://pubmed.ncbi.nlm.nih.gov/?term=Flatt%20AE%3A%20The%20care%20of%20congenital%20hand%20anomalies%2C%20St%20Louis%2C%201977%2C%20Mosby.%0A%0APreaxial%20Polydactyly%20Al-Aithan%20B%2C%20Al-Blaihed%20L%2C%20Mahmoud%20S%2C%20et%20al%3A)
You Might Also Like