Mastering Finger Infections: Surgical Management of Paronychia & Felons

Key Takeaway
Welcome to the OR, fellows. Today, we're tackling acute and chronic paronychia, and felons – common, yet often complex, hand infections. This masterclass will guide you through precise surgical anatomy, meticulous patient positioning, and granular step-by-step intraoperative execution. We'll cover incision and drainage techniques, eponychial marsupialization, and crucial pearls to prevent complications, ensuring optimal patient outcomes and functional recovery.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of hand infections, specifically acute and chronic paronychia, as well as felons, represents a fundamental pillar of orthopedic and hand surgery practice. While these conditions are frequently encountered in both emergency departments and outpatient clinics, they are paradoxically among the most mismanaged pathologies in the upper extremity. A superficial understanding of these distinct clinical entities often leads to inadequate drainage, iatrogenic injury to specialized structures, and prolonged patient morbidity. As orthopedic surgeons, we must approach these seemingly straightforward infections with the same anatomical reverence and technical precision as we would a complex intra-articular fracture or a microsurgical replantation. The overarching goal is the swift eradication of infection, preservation of the highly specialized digital anatomy, and the rapid restoration of pain-free function.
To master these pathologies, one must first delineate the distinct pathogenetic mechanisms that drive them. Acute paronychia is characterized by a rapid-onset bacterial infection of the soft tissue fold surrounding the fingernail (the perionychium). The infectious cascade is typically initiated by minor, often unnoticed mechanical trauma—such as nail biting, aggressive manicures, or simple hangnails—which breaches the protective seal between the nail plate and the eponychium. This breach allows for the inoculation of normal skin flora into the paronychial space. Staphylococcus aureus remains the most frequently isolated pathogen, although mixed infections involving Streptococcus species and oral anaerobes (particularly in nail-biters) are increasingly common. The localized inflammatory response rapidly progresses from cellulitis to a frank abscess, tracking along the path of least resistance within the paronychial fold.
Conversely, chronic paronychia represents a fundamentally different pathophysiological process. It is not merely an unresolved acute infection, but rather a chronic inflammatory dermatitis of the eponychium. This condition is disproportionately prevalent in individuals subjected to repeated, prolonged environmental exposures, particularly frequent water immersion or contact with chemical irritants (e.g., dishwashers, bartenders, healthcare personnel, and agricultural workers). The persistent environmental insult compromises the cuticle, leading to colonization by opportunistic organisms, most notably Candida albicans, alongside gram-positive cocci and atypical mycobacteria. The chronic inflammatory milieu induces progressive fibrosis and thickening of the eponychium. This fibrotic transformation compromises the microvascular supply to the dorsal nail fold, creating a vicious cycle of localized ischemia, impaired local immunity, and recurrent acute exacerbations.
A felon, in stark contrast to paronychial infections, is a deep-seated, closed-space infection of the distal digital pulp. The pathogenesis of a felon is intimately tied to the unique microanatomy of the fingertip. Inoculation typically occurs via penetrating trauma, such as a splinter or a contaminated needle stick. As the bacterial load proliferates, the ensuing inflammatory exudate and edema are trapped within the inelastic, compartmentalized spaces defined by the vertical fibrous septa of the digital pad. This results in a rapid, exponential rise in localized tissue pressure, effectively creating a micro-compartment syndrome of the fingertip. If surgical decompression is delayed, this elevated pressure precipitates microvascular compromise, ischemic necrosis of the adipose tissue, and ultimately, osteomyelitis of the underlying distal phalanx or proximal extension into the flexor tendon sheath. Differentiating these bacterial entities from herpetic whitlow—a self-limiting viral infection caused by the Herpes Simplex Virus (HSV)—is absolutely critical, as surgical intervention in a herpetic whitlow is strictly contraindicated and can lead to disastrous secondary bacterial superinfections.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of digital anatomy is the absolute prerequisite for any surgical intervention in the hand. The margin for error is measured in millimeters, and an imprecise incision can yield devastating functional and cosmetic consequences. The nail complex, or perionychium, is a highly specialized epidermal appendage designed for protection, tactile counter-pressure, and precise manipulation. The visible nail plate rests upon the nail bed, which is functionally divided into the proximal germinal matrix and the distal sterile matrix. The germinal matrix, situated deep to the eponychial fold, is responsible for approximately 90% of the nail plate's longitudinal growth. Iatrogenic injury to the germinal matrix during incision and drainage procedures is a primary cause of permanent, irreversible nail dystrophy, ridging, or split nail deformities.

Surrounding the nail plate are the protective soft tissue envelopes: the eponychium (proximal nail fold), the lateral paronychial folds, and the hyponychium (the distal seal beneath the free edge of the nail). The eponychium forms a critical, watertight seal over the base of the nail. In chronic paronychia, the destruction of this seal and the subsequent fibrotic thickening of the eponychium are the primary anatomical targets for surgical correction. The hyponychium serves a similar protective role distally, preventing subungual bacterial ingress. Understanding the continuity of these spaces is vital; an untreated unilateral paronychia can easily track proximally beneath the eponychium to involve the contralateral fold, creating a classic "runaround" abscess, or it can track deep to the nail plate, necessitating nail plate removal for adequate drainage.
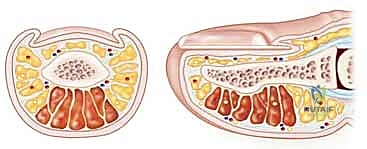
The anatomy of the digital pulp is equally complex and clinically relevant, particularly in the management of felons. The volar pad of the distal phalanx is not a singular, homogenous space. It is meticulously partitioned by numerous vertical fibrous septa that extend from the periosteum of the distal phalanx dorsally to the deep dermis volarly. These septa provide essential structural stability, preventing the volar skin from shearing during pinch and grasp activities. However, it is precisely this rigid compartmentalization that dictates the pathophysiology of a felon. When purulence accumulates within these unyielding compartments, the pressure cannot dissipate.
Navigating the neurovascular anatomy during digital decompression requires meticulous attention. The proper digital arteries and nerves bifurcate at the level of the metacarpophalangeal joint and course distally along the mid-lateral line of the digit. At the level of the distal interphalangeal (DIP) joint, they arborize extensively to supply the highly sensitive tactile pad. Crucially, the proper digital nerves lie volar to the digital arteries. When executing a lateral longitudinal incision for a felon, the surgeon must stay strictly dorsal to the mid-lateral line—typically within 3 to 5 millimeters of the lateral nail margin—to avoid transecting the terminal branches of the digital nerve. Injury to these structures not only results in a devastating loss of tactile sensation but frequently leads to the formation of exquisitely painful terminal neuromas, which can render the digit functionally useless.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention versus conservative management hinges on a precise clinical diagnosis, the duration of symptoms, and the presence of localized fluctuance or systemic involvement. The threshold for surgical intervention varies significantly between acute paronychia, chronic paronychia, and felons.
Indications for Surgical Management
For acute paronychia, the primary indication for surgery is the presence of a localized, fluctuant abscess or a subungual collection of purulence. If the infection has progressed beyond the early cellulitic phase (characterized merely by erythema and mild swelling) to a state of palpable fluctuance or visible pus beneath the cuticle or nail plate, conservative measures will invariably fail. Surgical drainage is mandatory to prevent ischemic necrosis of the nail matrix and proximal extension. For chronic paronychia, surgical intervention is indicated when the condition becomes refractory to exhaustive medical management. This includes failure to improve after prolonged avoidance of environmental irritants, topical or oral antifungal therapies, and topical corticosteroid application. The presence of a persistently thickened, fibrotic, and indurated eponychium that harbors recurrent acute exacerbations necessitates an eponychial marsupialization.
Felons represent an absolute indication for urgent surgical decompression. The presence of a tense, exquisitely tender, and swollen digital pulp—often described by the patient as a severe, throbbing pain that precludes sleep—demands immediate incision and drainage. Because of the rapid escalation of compartmental pressures, a "watch and wait" approach with isolated antibiotic therapy is highly discouraged, as it significantly increases the risk of distal phalangeal osteomyelitis and irreversible pulp necrosis. Any clinical suspicion of a felon warrants swift surgical exploration.
Contraindications and the Herpetic Whitlow Pitfall
The most critical absolute contraindication to surgical incision and drainage in the distal digit is the presence of a herpetic whitlow. Caused by HSV-1 or HSV-2, this viral infection presents with localized pain, erythema, and the pathognomonic appearance of grouped, non-purulent vesicles on an erythematous base. The digital pulp, while swollen, lacks the extreme, woody tension characteristic of a bacterial felon. Incising a herpetic whitlow is a grave error; it does not relieve symptoms, frequently introduces a secondary bacterial infection, delays viral clearance, and can lead to systemic viral dissemination.
| Clinical Entity | Primary Indications for Surgery | Absolute/Relative Contraindications |
|---|---|---|
| Acute Paronychia | Palpable fluctuance; visible purulence; subungual extension; failure of 48hr oral antibiotics. | Early cellulitis without fluctuance (relative - trial warm soaks/antibiotics first); Herpetic Whitlow (absolute). |
| Chronic Paronychia | Refractory to medical management (antifungals/steroids); severe eponychial fibrosis; recurrent acute flares. | Active, untreated fungal infection without fibrosis (relative - treat medically first). |
| Felon | Tense, throbbing, swollen digital pulp; suspected compartment syndrome of the fingertip. | Herpetic Whitlow (absolute); superficial epidermal blister (relative - requires unroofing, not deep septal release). |
| Herpetic Whitlow | NONE. Surgery is strictly contraindicated. | ALL SURGICAL I&D. Management is strictly medical (observation, antivirals). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative preparation is the cornerstone of a safe and effective surgical outcome. While these procedures are frequently performed in the emergency department or minor procedure room, the standards of surgical sterility, adequate anesthesia, and optimal visualization must not be compromised.
The initial clinical evaluation must rigorously differentiate between the various infectious etiologies. A thorough history should elicit the mechanism of injury, occupational hazards, duration of symptoms, and the patient's immune status. Immunocompromised patients, particularly those with poorly controlled diabetes mellitus, end-stage renal disease, or those undergoing active chemotherapy, require an aggressive approach, as they are highly susceptible to rapid proximal spread and systemic sepsis. In such patients, a comprehensive laboratory workup, including a complete blood count (CBC), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and blood cultures, is mandatory.
Radiographic evaluation is a critical, yet frequently overlooked, step in preoperative planning. Standard anteroposterior, lateral, and oblique radiographs of the affected digit should be obtained in all cases of felons, severe acute paronychia, and chronic, recalcitrant infections. The primary objective is to rule out underlying osteomyelitis of the distal phalanx, which manifests radiographically as cortical destruction, periosteal reaction, or focal osteopenia. Furthermore, radiographs are essential for identifying radio-opaque foreign bodies that may be serving as a persistent nidus for infection. If osteomyelitis is confirmed, the surgical plan must be expanded to include aggressive bone debridement and prolonged, culture-directed intravenous antibiotic therapy.
Anesthesia for digital infections is best achieved via a precise digital nerve block. The preferred agent is 1% or 2% lidocaine, or a 50/50 mixture of lidocaine and 0.5% bupivacaine for prolonged postoperative analgesia. The use of epinephrine in digital blocks for infected, already ischemic digits is historically debated, but in the setting of a tense felon with compromised microcirculation, it is strictly avoided to prevent irreversible digital necrosis. The block is administered via a dorsal approach at the level of the metacarpal neck. The needle is advanced from dorsal to volar, infiltrating the anesthetic adjacent to the proper digital nerves on both the radial and ulnar aspects of the digit. This technique is significantly less painful than volar injections and provides profound anesthesia. The surgeon must wait a minimum of 10 to 15 minutes to ensure a complete block before initiating the incision.
Patient positioning and the establishment of a bloodless field are vital for precise anatomical dissection. The patient is positioned supine with the affected extremity extended on a standard radiolucent hand table. A sterile field is prepped and draped using standard orthopedic protocols. To achieve a bloodless field, a digital tourniquet (such as a sterile Penrose drain or a specialized digital tourniquet ring) is applied at the base of the digit. For more extensive infections or when multiple digits are involved, a pneumatic forearm or upper arm tourniquet is utilized, inflated to 250 mmHg or approximately 100 mmHg above the patient's systolic blood pressure. This bloodless field is non-negotiable; it allows the surgeon to visualize the delicate neurovascular structures, thoroughly assess the extent of tissue necrosis, and ensure complete evacuation of the abscess cavity.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution must be deliberate, respecting the distinct anatomical boundaries of the nail complex and the digital pulp. The choice of incision is dictated entirely by the location and extent of the purulent collection.
Surgical Management of Acute Paronychia
For a localized acute paronychia confined to a single lateral nail fold, a simple longitudinal incision is employed.


Using a No. 15 or No. 11 scalpel blade, the incision is made directly into the paronychial fold, parallel to the nail edge. The critical technical nuance here is the orientation of the blade: the sharp edge must be directed strictly away from the nail bed and germinal matrix. Angling the blade towards the nail plate risks lacerating the matrix, guaranteeing a permanent longitudinal ridge or split in the patient's nail.


Upon entering the abscess cavity, a rush of purulent fluid is typically encountered. A small curved hemostat is then introduced into the cavity to gently break up any fibrous loculations and ensure complete drainage. The cavity is copiously irrigated with sterile saline.
If the infection has tracked beneath the eponychium to the contralateral side (a "runaround" abscess) or if there is visible purulence beneath the proximal nail plate (subungual extension), a more aggressive approach is required.


In these instances, the proximal one-third of the nail plate must be removed. The eponychium is carefully elevated off the nail plate using a Freer elevator. The proximal nail plate is then sharply excised and removed, exposing the underlying germinal matrix and allowing for complete evacuation of the subungual abscess. The eponychial fold is held open by packing the space lightly with a small strip of iodoform or plain gauze to prevent premature closure and re-accumulation of pus.
Surgical Management of Chronic Paronychia (Eponychial Marsupialization)
Chronic paronychia requires the excision of the diseased, fibrotic tissue to restore a healthy paronychial environment. The procedure of choice is eponychial marsupialization.


Following adequate anesthesia and tourniquet application, a crescent-shaped incision is marked over the dorsal aspect of the proximal nail fold. The maximum width of the crescent is typically 3 to 5 millimeters, centered over the area of greatest induration.


Using a No. 15 blade, the fibrotic eponychial tissue is excised en bloc, taking extreme care to stay superficial to the underlying germinal matrix. The excision should extend proximally enough to remove all diseased tissue but must not violate the matrix itself.

Once the fibrotic tissue is removed, the wound is left open to heal by secondary intention. This process allows for the regeneration of a thin, pliable, and healthy eponychial fold. Postoperatively, the wound is dressed with non-adherent gauze, and the patient is instructed to begin daily warm water soaks after 48 hours to promote drainage and healing.
Surgical Management of Felons
The surgical decompression of a felon requires dividing the vertical fibrous septa to release the compartmentalized pressure. Several incisions have been historically described, but many are now condemned due to high complication rates. The "fish-mouth" and "hockey-stick" incisions, which curve around the tip of the digit, are absolutely contraindicated as they routinely lead to ischemic necrosis of the tactile pad and severe, painful neuromas.

The preferred approach is the unilateral high lateral longitudinal incision. The incision is placed on the non-contact, non-tactile side of the digit (e.g., the ulnar side of the index, middle, and ring fingers; the radial side of the thumb and small finger).

The incision begins approximately 5 millimeters distal to the DIP joint flexion crease and extends distally, staying strictly dorsal to the mid-lateral line and within 3 to 5 millimeters of the lateral nail margin. This dorsal placement is critical to avoid transecting the volar terminal branches of the proper digital nerve.


Once the skin is incised, a blunt instrument, such as a small hemostat, is introduced into the pulp space. The instrument is swept volarly across the distal phalanx to bluntly rupture the fibrous septa and decompress the abscess cavities. Care must be taken not to violate the tendon sheath proximally or the periosteum deeply. The cavity is aggressively irrigated. A small wick is placed loosely into the wound to maintain patency for 48 hours, and a bulky dressing is applied. Alternatively, a volar longitudinal incision directly over the point of maximal fluctuance can be used, particularly if the abscess is pointing volarly, taking care not to cross the DIP flexion crease.
Complications, Incidence Rates, and Salvage Management
Despite seemingly straightforward pathology, the complication rates associated with surgical management of paronychia and felons are non-trivial, particularly when anatomical principles are violated or intervention is delayed. The surgeon must be acutely aware of these potential pitfalls and possess the reconstructive armamentarium to address them.
The most common complication following paronychia drainage is recurrence, often stemming from inadequate initial decompression or failure to remove the proximal nail plate in the setting of subungual extension. Iatrogenic nail deformities represent a devastating complication, occurring in up to 10% of poorly executed procedures. Laceration of the germinal matrix during incision results in permanent longitudinal ridging, splitting, or complete absence of nail growth. Salvage management for severe nail deformities may require complex nail bed grafting using sterile matrix grafts from the toe, though results are functionally and cosmetically variable.
Complications associated with felons are typically more severe due to the closed-space nature of the infection. Delay in surgical decompression rapidly precipitates ischemic necrosis of the digital pulp pad, leading to significant soft tissue loss that may necessitate local advancement flaps (e.g., V-Y advancement, Moberg flaps) for coverage. Proximal extension of the infection can lead to septic flexor tenosynovitis—a surgical emergency requiring immediate mid-axial incision and continuous catheter irrigation of the flexor sheath. Osteomyelitis of the distal phalanx occurs in approximately 5-10% of neglected felons. If osteomyelitis develops, aggressive surgical debridement of the infected bone is required, occasionally resulting in terminal amputation if the bony destruction is extensive.
Neuromas and sensory deficits are the direct result of poor incision placement during felon decompression. Transection of the terminal digital nerve branches via a low lateral or "fish-mouth" incision results in an exquisitely painful neuroma at the fingertip, severely limiting hand function. Management of a terminal neuroma is notoriously difficult, often requiring surgical excision and proximal burying of the nerve stump into bone or muscle, with unpredictable success rates.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management |
|---|---|---|---|
| Nail Deformity (Ridging/Split) | 5-10% | Iatrogenic laceration of germinal matrix; untreated subungual abscess. | Nail bed repair; sterile matrix grafting (toe-to-hand). |
| Osteomyelitis of Distal Phalanx | 5-10% (Felons) | Delayed decompression of felon; chronic untreated paronychia. | Aggressive bone debridement; prolonged IV antibiotics; possible terminal amputation. |
| Septic Flexor Tenosynovitis | < 5% | Proximal tracking of felon into flexor sheath. | Emergent surgical washout of flexor tendon sheath; targeted antibiotics. |
| Painful Terminal Neuroma | Variable (Technique dependent) | Improper incision placement (e.g., fish-mouth, low lateral incision). | Neuroma excision; proximal nerve transposition/burying. |
| Pulp Necrosis | < 5% | Delayed decompression; excessive tourniquet time; use of epinephrine in digital block. | Debridement; local advancement flaps (V-Y, Moberg) for soft tissue coverage. |
Phased Post-Operative Rehabilitation Protocols
The surgical intervention is merely the first phase of treatment; rigorous postoperative care and rehabilitation are essential to ensure complete eradication of the infection and restoration of digital mobility. The rehabilitation protocol is phased, balancing the need for wound drainage with the imperative to prevent debilitating stiffness of the interphalangeal joints.
Phase I: Immediate Post-Operative Period (Days 0-2)
Immediately following surgery, the digit is dressed with a bulky, non-compressive soft dressing. The hand must be strictly elevated above the level of the heart to minimize edema and throbbing pain. If a wick or packing was placed during the procedure, it is typically removed in the clinic at the 48-hour mark. During this initial phase, the patient is maintained on culture-directed oral antibiotics (empiric coverage typically includes a first-generation cephalosporin or clindamycin/trimethoprim-sulfamethoxazole if MRSA is suspected). Active range of motion of the uninvolved digits is highly encouraged to promote venous and lymphatic return.
Phase II: Wound Care and Early Mobilization (Days 3-14)
Once the packing is removed, the patient transitions to a regimen of warm water or dilute chlorhexidine soaks. The patient is instructed to soak the affected digit for 15 to 20 minutes, three to four times daily. This crucial step promotes continuous drainage of residual exudate, prevents premature closure of the skin edges, and provides soothing analgesia. Following each soak, a light, non-adherent dressing is applied. Concurrently, aggressive active and active-assisted range of motion exercises of the distal and proximal interphalangeal joints of the affected digit are initiated. Stiffness is a rapid and unforgiving complication of digital infections; early mobilization prevents the formation of restrictive flexor tendon adhesions and joint capsular contractures.
Phase III: Strengthening and Return to Function (Weeks 2-6)
As the wound heals by secondary intention—a process that typically takes 2 to 3 weeks depending on the extent of the incision and debridement—the frequency of the soaks is gradually reduced. Once the wound is completely epithelial
