Radial Styloidectomy: Indications, Biomechanics, and Surgical Technique
Key Takeaway
Radial styloidectomy is a valuable surgical adjunct for treating scaphoid nonunions complicated by localized radioscaphoid arthritis. While rarely indicated as an isolated procedure in young patients, it provides significant pain relief in older patients with degenerative changes confined to the scaphoid fossa. This guide details the Stewart technique, emphasizing precise osteotomy execution and the critical preservation of the volar radiocarpal ligaments to prevent postoperative ulnar carpal translocation.
Introduction to Radial Styloidectomy
Radial styloidectomy is a highly specific, targeted surgical procedure designed to address localized degenerative changes at the radioscaphoid articulation. Historically popularized by Stewart, the procedure involves the precise resection of the radial styloid to decompress the radioscaphoid joint and eliminate painful impingement.
In contemporary orthopedic practice, radial styloidectomy is rarely performed as an isolated procedure in young, high-demand patients. However, it remains a critical adjunct in the management of scaphoid nonunions complicated by early arthritic changes (Scaphoid Nonunion Advanced Collapse, or SNAC, Stage I). When arthritic changes are strictly confined to the scaphoid fossa of the radiocarpal joint, styloidectomy is highly indicated in conjunction with scaphoid bone grafting, internal fixation, or excision of a fragmented proximal pole. Furthermore, in older, lower-demand patients presenting with predominant radioscaphoid arthritis—provided the proximal scaphoid fragment is stable—an isolated radial styloidectomy can yield profound and durable pain relief.
Pathoanatomy and Biomechanics
To master the radial styloidectomy, the orthopedic surgeon must possess an intimate understanding of distal radius articular geometry and the complex ligamentous stabilizers of the carpus.
Articular Geometry of the Distal Radius
The distal articular surface of the radius is biconcave, divided into two distinct fossae separated by a subtle, yet biomechanically crucial, anteroposterior ridge of bone (the interfossal ridge).
* The Scaphoid Fossa: The lateral (radial) concavity that articulates with the proximal pole of the scaphoid.
* The Lunate Fossa: The medial (ulnar) concavity that articulates with the lunate.
In the setting of a scaphoid nonunion, the uncoupled scaphoid fragments undergo predictable postural changes: the distal fragment flexes (driven by the radioscaphocapitate ligament and the trapezium), while the proximal fragment extends with the lunate. This foreshortening and angular deformity create a severe kinematic mismatch at the radioscaphoid joint. The abnormal point-loading rapidly degrades the articular cartilage of the radial styloid, initiating the SNAC sequence.
Ligamentous Anatomy and the Risk of Ulnar Translocation
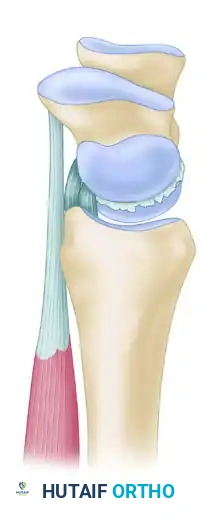
The most critical anatomical structures in the vicinity of the radial styloid are the volar radiocarpal ligaments, which serve as the primary restraints against the natural tendency of the carpus to slide ulnarly down the inclined articular surface of the radius.
- Radioscaphocapitate (RSC) Ligament: Originates from the volar aspect of the radial styloid.
- Long Radiolunate (LRL) Ligament: Originates just ulnar to the RSC ligament.
- Short Radiolunate (SRL) Ligament: Originates from the volar margin of the lunate fossa.
🚨 Surgical Warning: The RSC Ligament
The most devastating complication of a radial styloidectomy is iatrogenic ulnar translocation of the carpus. This occurs when the origin of the radioscaphocapitate (RSC) ligament is inadvertently resected or irreparably damaged during the osteotomy. While Stewart recommended resecting enough styloid to remove the entire articulation with the scaphoid, modern biomechanical studies mandate that the volar cortical rim—where the RSC ligament attaches—must be meticulously preserved via subperiosteal dissection.
Indications and Contraindications
Indications
- SNAC Stage I Wrist: Localized arthritis between the radial styloid and the scaphoid, performed as an adjunct to scaphoid reconstruction (bone grafting and internal fixation).
- Symptomatic Scaphoid Nonunion in the Elderly: As an isolated palliative procedure for pain relief in older, low-demand patients where the proximal fragment is not loose or highly unstable.
- Radioscaphoid Impingement: Secondary to malunion of the distal radius or scaphoid.
Contraindications
- Midcarpal Arthritis: If degenerative changes have progressed to the capitolunate joint (SNAC Stage II or III), a styloidectomy will fail to relieve pain. Proximal row carpectomy (PRC) or scaphoid excision with four-corner fusion is required.
- Pancarpal Arthritis: Requires total wrist arthrodesis or arthroplasty.
- Pre-existing Carpal Instability: Evidence of ulnar translocation or severe dorsal intercalated segment instability (DISI) that cannot be corrected.
Preoperative Evaluation
A meticulous preoperative assessment is mandatory to ensure the pathology is strictly limited to the radial styloid.
- Clinical Examination: Patients typically present with localized tenderness over the anatomic snuffbox and radial styloid. Pain is exacerbated by radial deviation and wrist extension.
- Radiographic Imaging: Standard posteroanterior (PA), lateral, and scaphoid views are required. Look for the classic "beaking" or sclerosis of the radial styloid.
- Advanced Imaging: Computed Tomography (CT) is invaluable for assessing the exact location and extent of cystic changes and osteophytes. Magnetic Resonance Imaging (MRI) may be utilized to assess the viability of the proximal scaphoid pole if concurrent grafting is planned.
Surgical Technique: The Stewart Approach
The following technique details the classic Stewart approach, enhanced with modern principles of soft tissue preservation and precise osteotomy execution.
1. Anesthesia and Positioning
- Anesthesia: Regional anesthesia (supraclavicular or axillary brachial plexus block) is preferred, though general anesthesia is acceptable.
- Positioning: The patient is placed supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg after exsanguination with an Esmarch bandage.
2. Incision and Superficial Dissection
Stewart described a highly utilitarian bayonet-shaped incision that provides extensile exposure while minimizing the risk of scar contracture across the wrist crease.
- The Incision: Make a bayonet-shaped incision along the radial aspect of the wrist.
- Begin distally over the dorsum of the first metacarpal.
- Proceed proximally into the anatomical snuffbox.
- Turn dorsally to run parallel along the extensor crease of the wrist.
- Finally, turn proximally along the dorsoradial aspect of the distal radius.
- Nerve Protection: Carefully dissect through the subcutaneous tissues. The superficial sensory branches of the radial nerve (SBRN) are highly variable and exquisitely sensitive to traction. Identify, mobilize, and protect these branches using vessel loops.
- Vascular Protection: Identify the radial artery as it passes through the anatomical snuffbox deep to the tendons of the first extensor compartment (abductor pollicis longus and extensor pollicis brevis). Retract the artery gently to avoid vasospasm or injury.
💡 Clinical Pearl: SBRN Management
Neuroma of the superficial branch of the radial nerve is a notoriously difficult complication to treat and can leave the patient with pain worse than their preoperative arthritis. Avoid aggressive retraction. Keep the nerve branches moist and protected within the subcutaneous fat flaps rather than skeletonizing them.
3. Deep Dissection and Capsulotomy
- Extensor Compartments: Open the first extensor compartment and retract the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons volarly. Retract the extensor pollicis longus (EPL) tendon dorsally.
- Capsular Incision: Incise the radiocarpal joint capsule longitudinally over the radial styloid.
- Subperiosteal Elevation: Expose the radial styloid strictly subperiosteally.
- Careful subperiosteal dissection on both the dorsal and palmar surfaces is the most critical step of the exposure.
- By elevating the periosteum volarly, the origins of the volar radiocarpal ligaments (specifically the RSC) are peeled back and protected from the subsequent osteotomy. Excessive disruption of these ligaments will lead to catastrophic ulnar translocation of the carpus.
4. The Osteotomy
The goal of the osteotomy is to remove the arthritic scaphoid fossa while preserving the lunate fossa and the critical ligamentous attachments.
- Identify the Landmarks: Inspect the articular surface of the distal radius. Locate the interfossal ridge—the small ridge of bone that separates the articular fossa for the lunate from that for the scaphoid.
- Orientation: The osteotomy cut must be made perpendicular to the long axis of the radius. An oblique cut that travels too far proximally will compromise the structural integrity of the metaphysis, while a cut that angles into the lunate fossa will damage the lunate articulation.
- Execution:
- Use a sharp, thin osteotome or a thin oscillating saw blade.
- Place a small Hohmann or malleable retractor into the joint to protect the scaphoid articular surface from the saw blade.
- Begin the cut at the lateral cortex of the radial styloid and advance medially.
- The ulnar border of the osteotomy must terminate exactly at the interfossal ridge just located.
- Resection: Complete the osteotomy and remove the resected styloid fragment.
🔪 Surgical Pitfall: Over-Resection
Stewart historically recommended resecting enough styloid to remove the entire articulation with the scaphoid. However, modern surgeons must balance this against ligamentous stability. Resecting more than 3 to 4 mm of the styloid exponentially increases the risk of detaching the RSC ligament. Limit the resection to the arthritic radial styloid tip and the lateral aspect of the scaphoid fossa, ensuring the volar cortical rim remains intact.
5. Joint Inspection and Closure
- Debridement: Inspect the joint space. Remove any loose bodies, osteophytes, or debris generated by the saw.
- Fluoroscopy: Utilize intraoperative fluoroscopy to confirm adequate resection of the styloid and ensure no step-off or damage has occurred at the lunate fossa.
- Capsular Closure: Repair the radiocarpal capsule meticulously using interrupted absorbable sutures (e.g., 3-0 Vicryl). A robust capsular repair adds a secondary layer of stability against carpal translation.
- Skin Closure: Deflate the tourniquet and achieve meticulous hemostasis. Close the subcutaneous tissue and skin according to surgeon preference. Apply a sterile dressing and a volar plaster splint.
Postoperative Protocol and Rehabilitation
The postoperative rehabilitation protocol depends heavily on whether the radial styloidectomy was performed in isolation or as an adjunct to scaphoid reconstruction.
Isolated Radial Styloidectomy
- Phase I (0-2 Weeks): The wrist is immobilized in a bulky dressing and a volar short-arm splint to allow the capsular repair and soft tissues to heal. Finger range of motion (ROM) and shoulder/elbow exercises are initiated immediately to prevent stiffness.
- Phase II (2-6 Weeks): Sutures are removed at 10-14 days. The patient is transitioned to a removable wrist orthosis. Active and active-assisted ROM exercises for the wrist are initiated under the guidance of a hand therapist.
- Phase III (6+ Weeks): Progressive strengthening exercises are introduced. The orthosis is weaned for daily activities. Full recovery and maximal pain relief may take 3 to 6 months as the joint adapts to the altered kinematics.
Styloidectomy with Concurrent Scaphoid Grafting/Fixation
If the styloidectomy was performed alongside scaphoid bone grafting and internal fixation, the postoperative protocol is dictated entirely by the scaphoid fracture.
* The wrist is typically immobilized in a thumb spica cast or splint for 6 to 8 weeks, or until radiographic evidence of scaphoid union is observed.
* Once union is confirmed, a structured therapy program focusing on restoring wrist extension, flexion, and radioulnar deviation is commenced.
Complications and Management
While generally a safe and effective procedure, radial styloidectomy carries specific risks that the orthopedic surgeon must anticipate and mitigate.
- Ulnar Translocation of the Carpus: As emphasized, this is the most severe complication, resulting from over-resection of the styloid and detachment of the RSC ligament. If recognized postoperatively, it may necessitate complex ligamentous reconstruction or partial wrist arthrodesis (e.g., radioscapholunate fusion).
- SBRN Neuritis: Injury or traction to the superficial branch of the radial nerve can cause debilitating neuropathic pain. Management includes gabapentinoids, desensitization therapy, and, in refractory cases, surgical exploration and nerve burying.
- Inadequate Resection: Failure to resect enough of the arthritic scaphoid fossa will result in persistent impingement and ongoing pain. Preoperative and intraoperative fluoroscopic templating is essential to ensure adequate decompression.
- Progression of Arthritis: Patients must be counseled that radial styloidectomy does not halt the progression of carpal instability if a scaphoid nonunion remains unhealed. It is a palliative or adjunctive measure; progressive midcarpal arthritis may eventually require salvage procedures such as a proximal row carpectomy.
Conclusion
Radial styloidectomy remains a highly effective surgical tool in the armamentarium of the orthopedic hand and wrist surgeon. When applied to the correct indications—specifically SNAC Stage I wrists or isolated radioscaphoid arthritis in the elderly—it provides reliable pain relief and functional improvement. Mastery of this technique requires a profound respect for the volar radiocarpal ligaments, meticulous soft-tissue handling, and precise execution of the osteotomy to balance adequate joint decompression with the preservation of carpal stability.
You Might Also Like