Mastering the Management of Chronic Unreduced Shoulder Dislocations
Key Takeaway
Chronic unreduced shoulder dislocations present complex reconstructive challenges due to severe soft-tissue contractures, capsular bowstringing, and significant osteochondral defects. Management requires meticulous preoperative CT evaluation to quantify articular damage. Treatment ranges from benign neglect in low-demand patients to complex open reduction, subscapularis transfer (McLaughlin procedure), or arthroplasty. Successful surgical intervention demands precise neurovascular protection, particularly of the axillary artery and nerve, alongside rigid postoperative immobilization protocols.
Introduction to Chronic Unreduced Shoulder Dislocations
Old, unreduced dislocations of the glenohumeral joint represent a formidable challenge to the orthopaedic surgeon. Typically defined as dislocations present for greater than 3 to 4 weeks, these injuries most frequently occur in patients older than 50 years. The primary clinical complaints are chronic, debilitating pain and a profound limitation of glenohumeral motion. Pain is typically exacerbated by attempts to move the shoulder beyond its newly restricted, pathological range.
While the majority of these chronic dislocations are traumatic in origin, they are frequently precipitated by seemingly trivial injuries. This phenomenon is largely attributed to age-related degeneration of the dynamic and static stabilizers of the shoulder, including the rotator cuff musculature, the subscapularis tendon, and the capsulolabral complex. In younger demographics, unreduced dislocations are highly correlated with specific comorbidities, notably chronic alcoholism, seizure disorders, or polytrauma, where the initial shoulder injury may be overlooked during the acute resuscitation phase.
Clinical Pearl: According to Schulz et al., more than 50% of chronic unreduced dislocations are complicated by concomitant fractures of the glenoid cavity, humeral tuberosities, or the proximal humeral shaft. Furthermore, over one-third present with established neurological deficits, mandating a thorough preoperative electromyographic (EMG) and clinical neurological assessment.
Pathoanatomy and Biomechanics
The chronicity of the dislocation induces profound pathological alterations in both the osseous architecture and the surrounding soft-tissue envelope. Understanding these changes is paramount for successful surgical reconstruction.
Soft-Tissue Contractures and "Bowstringing"
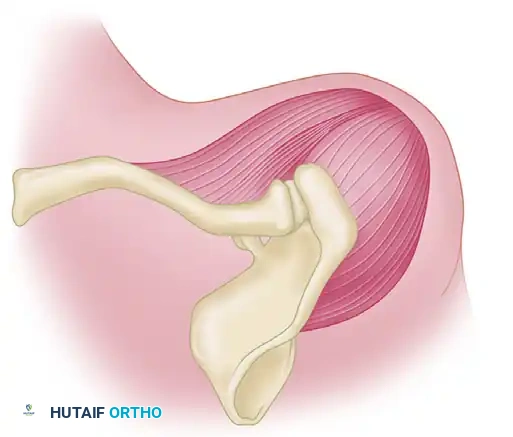
Within weeks of the initial dislocation, severe fibrous and capsular contractures develop across the base of the glenoid. The rotator cuff muscles undergo adaptive shortening and fibrosis. This fibrotic cascade frequently engulfs adjacent critical structures, including the axillary nerve and axillary artery, severely distorting normal surgical planes.
Neviaser classically described the capsular "bowstringing" phenomenon. In this state, the redundant joint capsule becomes densely adherent to the articular surface of the empty glenoid fossa. This fibrotic obliteration of the joint space acts as an absolute mechanical block, rendering closed reduction impossible and necessitating meticulous open surgical release.
Osseous Pathology
Bony architecture is progressively destroyed by the persistent abnormal articulation.
Anterior Dislocations:
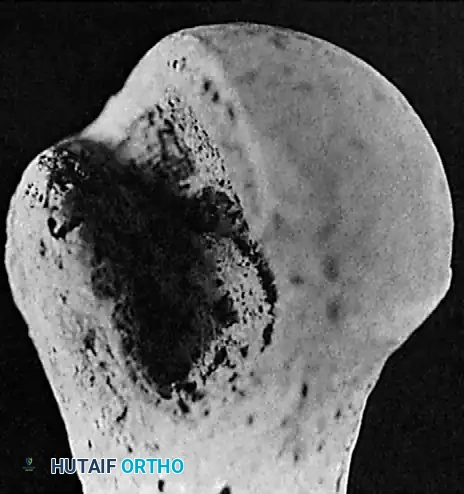
In chronic anterior dislocations, the posterolateral aspect of the humeral head is driven against the sharp anterior rim of the glenoid. This constant impingement produces a massive compression fracture. Because the patient repeatedly attempts to mobilize the joint, this defect is typically much larger and deeper than the classic Hill-Sachs lesion seen in recurrent, acute anterior instability.
Concurrently, the anterior glenoid rim suffers compression fractures, and in long-standing cases, a false joint or "pseudoarticulation" forms between the humeral head and the anterior scapular neck.

Posterior Dislocations:
Chronic posterior dislocations produce a reverse Hill-Sachs lesion—a large compression fracture on the anteromedial aspect of the humeral head caused by impingement against the posterior glenoid rim. Similar to anterior variants, these defects enlarge over time due to the patient's continual, forceful attempts to increase their range of motion.
Clinical and Radiographic Evaluation
Clinical Presentation
Loss of motion is the hallmark clinical finding. The pattern of restriction is diagnostic:
* Old Anterior Dislocations: Severe restriction in abduction and internal rotation. The arm is typically held away from the body in fixed external rotation, making it difficult for the patient to reach their face and impossible to reach their back.
* Old Posterior Dislocations: Severe restriction in abduction and external rotation. The arm rests at the side in fixed internal rotation. Interestingly, this position allows the patient to reach their face, head, and torso, often masking the functional deficit and delaying diagnosis.
Imaging Strategy
A complete radiographic trauma series is mandatory, including true anteroposterior (Grashey) and axillary lateral views. The axillary view is the gold standard for confirming the direction of the dislocation and identifying engagement of the glenoid rim within the humeral head defect.

As emphasized by Kirtland et al., computed tomography (CT) with three-dimensional (3D) reconstruction is the definitive modality for evaluating bony injuries. CT accurately quantifies the percentage of articular surface damage on the humeral head, which is the primary determining factor in selecting the appropriate surgical intervention.

Treatment Algorithm
The management of chronic unreduced dislocations is highly individualized. Options include benign neglect, closed reduction (with or without arthroscopic assistance), open reduction, hemiarthroplasty, and total shoulder arthroplasty (TSA).
1. Non-Operative Management (Benign Neglect)
Not all patients require surgical intervention. In elderly, low-demand patients with severe medical comorbidities, the risks of surgery may outweigh the benefits. Hawkins et al. documented patients with persistent locked posterior dislocations who underwent no treatment; over a 3 to 8-year follow-up, their pain did not progress and remained tolerable.
Surgical Warning: Patients with untreated posterior dislocations generally exhibit higher functional scores than those with untreated anterior dislocations, as the internally rotated position of a posterior dislocation preserves hand-to-mouth function.
2. Closed Reduction
Manipulative closed reduction is fraught with complications and should only be attempted after careful consideration of the patient's age, bone density (osteoporosis), vascular status, and the duration of the dislocation.
Contraindications for Closed Reduction:
* Dislocation present for >4 weeks.
* Humeral head impression defect >20% of the articular surface.
* Severe osteoporosis (high risk of iatrogenic proximal humerus fracture).
If attempted, it must be performed under general anesthesia with complete neuromuscular blockade. Traction must be minimal, and leverage maneuvers are strictly forbidden. In elderly patients with atherosclerotic disease, forceful reduction carries a catastrophic risk of axillary artery rupture.
3. Open Reduction
Open reduction is indicated for dislocations present for less than 6 months with an articular surface defect of less than 45%.
Surgical Obstacles:
1. Achieving Reduction: Hindered by severe fibrosis, muscle shortening, capsular bowstringing, and glenoid fossa scarring.
2. Maintaining Reduction: Hindered by the large osteochondral defect and inherent instability.
Hawkins et al. noted that open reduction uniformly fails if the articular defect exceeds 45% or if the dislocation has been present for over a year. In such cases, arthroplasty is the treatment of choice.
Surgical Techniques
Open Reduction of Anterior Dislocations (Rowe and Zarins Technique)
1. Patient Positioning and Approach:
Place the patient in the beach-chair position. An anterior approach via the deltopectoral interval is standard. Make a 10 to 12.5 cm incision extending inferiorly from the lateral third of the clavicle.
2. Deep Dissection:
Develop the deltopectoral interval, retracting the cephalic vein laterally with the deltoid. Retract the conjoined tendon (short head of the biceps and coracobrachialis) medially. The displaced humeral head will be palpable or visible inferior to the coracoid process.
3. Capsular Release and Nerve Protection:
Before attempting reduction, the capsule must be opened, and the coracohumeral ligament completely divided. The glenoid cavity must be meticulously cleared of all adherent fibrous tissue (Neviaser's bowstringing).
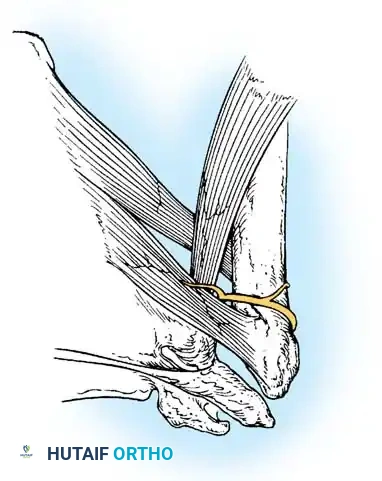
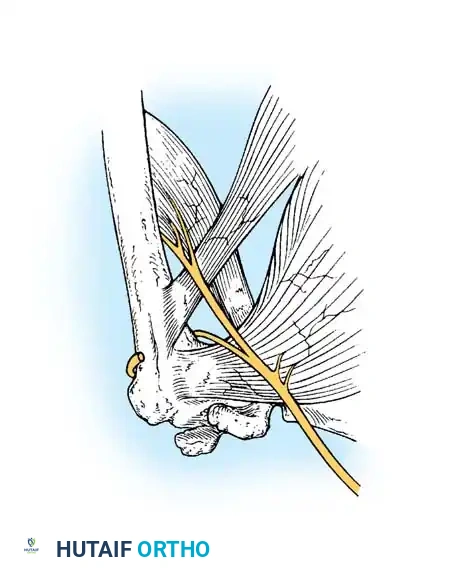
Release of the subscapularis is mandatory. Crucial Step: The axillary nerve is highly vulnerable during this step. In anterior dislocations, the subscapularis is displaced anteriorly, creating a traction injury on the axillary nerve, which is tethered at the brachial plexus above and the quadrangular space below.
4. Joint Reduction:
Gently lever the humeral head back into the glenoid cavity. Avoid excessive mechanical force with retractors or bone levers to prevent iatrogenic fractures of the osteoporotic humeral head or glenoid rim. Once reduced, gently manipulate the shoulder to stretch the contracted soft tissues until a near-normal range of motion is achieved.
5. Closure:
The capsule is typically too contracted to permit primary closure. Carefully repair the subscapularis tendon, maintaining strict awareness of the axillary nerve's proximity.
Management of Posterior Dislocations and Bony Defects
For chronic posterior dislocations, the surgical approach may vary. While Neviaser and Rowe recommended a superior approach, an anteromedial approach (deltopectoral) is generally preferred for addressing the reverse Hill-Sachs defect.
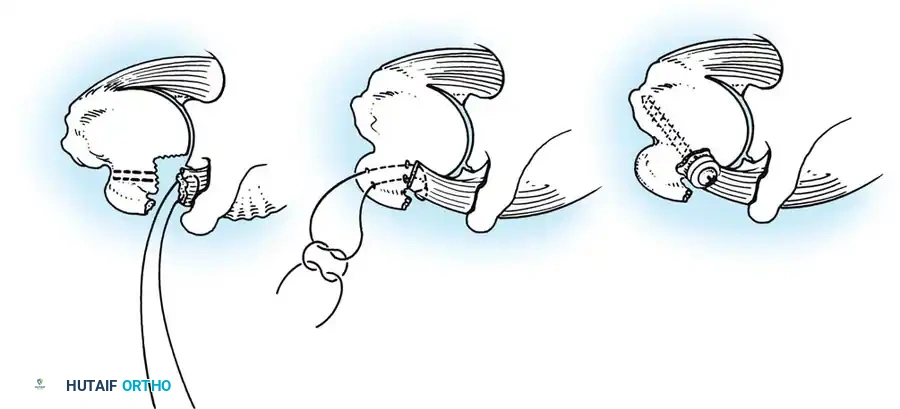
The McLaughlin Procedure:
When the anteromedial humeral head defect is between 20% and 45%, it will engage the posterior glenoid rim, causing recurrent instability. McLaughlin described a technique to fill this defect by transferring the subscapularis tendon (with or without the lesser tuberosity) directly into the defect, effectively converting an intra-articular defect into an extra-articular one and preventing engagement.
Advanced Reconstruction and Arthroplasty
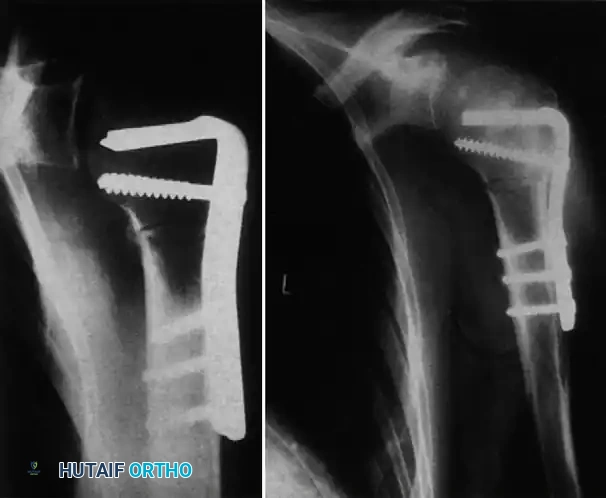
In cases where the humeral head is non-salvageable (defect >45%, duration >6 months, or severe avascular necrosis), prosthetic replacement is required. Depending on glenoid bone stock, this may involve a hemiarthroplasty or a total shoulder arthroplasty. In cases complicated by severe proximal humerus fractures or nonunions associated with the dislocation, rigid internal fixation with locking plates may be required as a salvage procedure before or in conjunction with joint reconstruction.
Methods of Postoperative Fixation and Immobilization
Maintaining reduction postoperatively is as critical as the reduction itself. Several techniques have been described to prevent early re-dislocation:
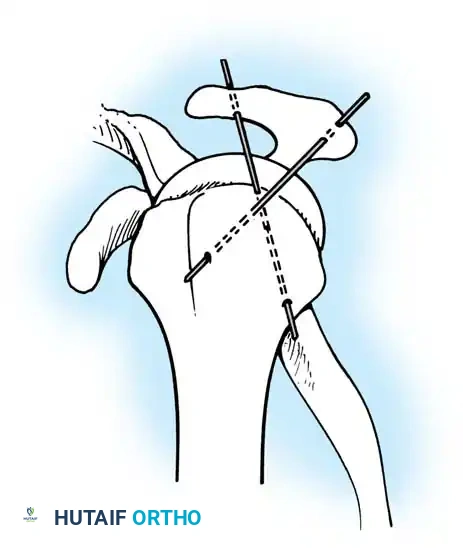
1. Transarticular Fixation:
Neviaser recommended transfixing the glenohumeral joint with a Swiss screw to provide rigid temporary stability.

Alternatively, Wilson and McKeever described the use of crossed Kirschner wires driven through the acromion directly into the humeral head.
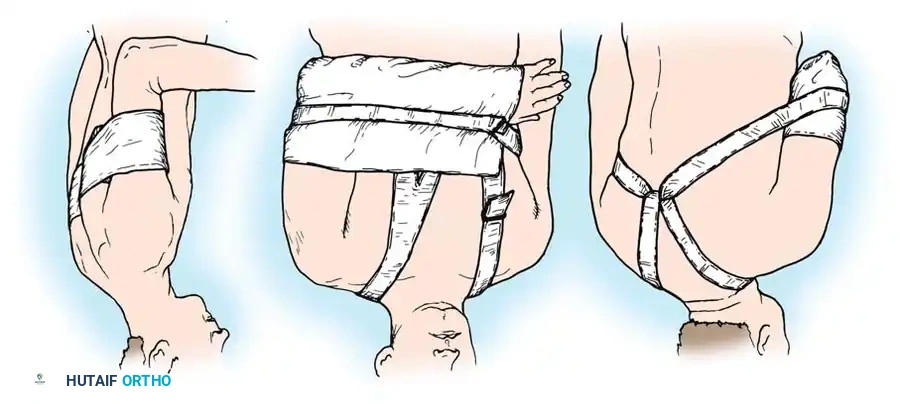
2. Positional Immobilization (Rowe and Zarins):
Rowe and Zarins argued against transarticular hardware, advocating instead for strict positional immobilization.
* For Anterior Dislocations: The arm is immobilized anterior to the coronal plane of the body.
* For Posterior Dislocations: The arm is immobilized posterior to the coronal plane of the body.
Postoperative Protocol and Rehabilitation
If internal fixation (screws or K-wires) is utilized, the arm is supported in an abduction splint or spica cast, and the hardware is removed at 3 to 4 weeks in the clinic.
If positional immobilization (Rowe and Zarins method) is employed, the custom orthosis is maintained for exactly 3 weeks.
Rehabilitation Phases:
* Weeks 3-4: Initiate gentle, gravity-assisted pendulum exercises.
* Weeks 4-8: Progress to active-assisted and passive range of motion within the limits of comfort. Aggressive passive stretching is avoided to prevent re-dislocation.
* Months 2-6: The shoulder should be supported in a splint at night until dynamic stability (deltoid and rotator cuff strength) is restored.
Patient Counseling: It is imperative to manage patient expectations. Full, normal function of the shoulder is rarely, if ever, regained after open reduction of a chronic dislocation. Motion will remain permanently limited, particularly in abduction and external rotation. The primary goals of surgery are pain relief, restoration of basic activities of daily living, and prevention of further neurovascular compromise.
📚 Medical References
- s, J Shoulder Elbow Surg 12:446, 2003.
- Hawkins RJ, Neer CS II, Pianta RM, et al: Locked posterior dislocation of the shoulder, J Bone Joint Surg 69A:9, 1987.
- Keppler P, Holz U, Thielemann FW, et al: Locked posterior dislocation of the shoulder: treatment using rotational osteotomy of the humerus, J Orthop Trauma 8:286, 1994.
- Kirtland S, Resnick D, Sartoris D, et al: Chronic,
You Might Also Like