Pelvis Fractures and Dislocations: Your Complete Guide
Key Takeaway
We review everything you need to understand about Pelvis Fractures and Dislocations: Your Complete Guide. Pelvis fractures and dislocations are injuries to the pelvic ring, comprised of the sacrum and two innominate bones, inherently stabilized by a complex network of ligaments. These injuries commonly result from high-energy trauma in younger individuals and minimal trauma in the elderly. The estimated annual incidence is 37 cases per 100,000 population.
Introduction and Epidemiology
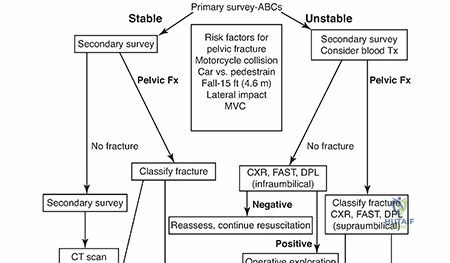
Pelvic ring injuries represent a heterogeneous group of fractures and dislocations that range from low-energy, stable osteoporotic fractures to high-energy, life-threatening disruptions of the pelvic architecture. The incidence of pelvic fractures in the United States has been estimated to be 37 cases per 100,000 population per year. The demographic distribution of these injuries demonstrates a classic bimodal curve. In persons younger than 35 years, males sustain more pelvic fractures than females, predominantly due to high-energy trauma such as motor vehicle collisions, motorcycle accidents, pedestrian-versus-auto incidents, and falls from significant heights. Conversely, in persons older than 35 years, women sustain more pelvic fractures than men. Most pelvic fractures sustained in the elderly population occur from minimal trauma, such as a low fall from a standing height, reflecting the increasing prevalence of Fragility Fractures of the Pelvis (FFP).
High-energy pelvic ring disruptions are frequently associated with multisystem polytrauma. Mortality rates in patients with hemodynamically unstable pelvic fractures remain high, historically reported between 15% and 40%, primarily driven by acute retroperitoneal hemorrhage and subsequent multiorgan failure. The management of these injuries requires a multidisciplinary approach, integrating advanced trauma life support (ATLS) protocols, aggressive resuscitation, damage control orthopedics, and precise definitive surgical reconstruction to restore pelvic biomechanics.
Surgical Anatomy and Biomechanics
A profound understanding of pelvic osteology, ligamentous stabilizers, and surrounding neurovascular structures is paramount for accurate diagnosis, classification, and safe surgical intervention.
Osteology of the Pelvic Ring
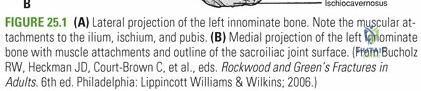
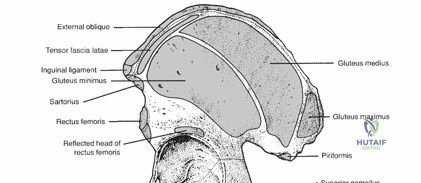
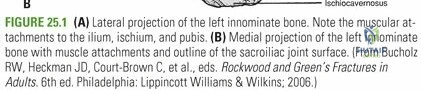
The pelvic ring is composed of the sacrum and two innominate bones joined anteriorly at the symphysis pubis and posteriorly at the paired sacroiliac joints. The innominate bone is formed at maturity by the fusion of three distinct ossification centers: the ilium, the ischium, and the pubis. These segments converge and fuse through the triradiate cartilage at the dome of the acetabulum.
The pelvic brim is formed by the arcuate lines that join the sacral promontory posteriorly and the superior pubic rami anteriorly. Below this anatomical landmark lies the true or lesser pelvis, which contains the pelvic viscera, including the bladder, rectum, and reproductive organs. Above the pelvic brim is the false or greater pelvis, representing the inferior aspect of the abdominal cavity and providing support for the lower abdominal viscera.
Ligamentous Stabilizers
Inherent stability of the pelvis is almost entirely conferred by its robust ligamentous structures rather than bony congruence. These stabilizers are anatomically and functionally divided into distinct groups based on their attachments:
Sacrum to Ilium Ligaments
The strongest and most critical ligamentous structures reside in the posterior aspect of the pelvis, connecting the sacrum to the innominate bones.
* The sacroiliac ligamentous complex is divided into posterior (short and long) and anterior ligaments. The posterior sacroiliac ligaments are massive and provide the majority of the weight-bearing stability to the posterior ring.
* The sacrotuberous ligament runs from the posterolateral aspect of the sacrum and the dorsal aspect of the posterior iliac spine to the ischial tuberosity. This ligament, functioning in association with the posterior sacroiliac ligaments, is exceptionally important in maintaining the vertical stability of the hemipelvis.
* The sacrospinous ligament is a triangular structure running from the lateral margins of the sacrum and coccyx to insert on the ischial spine. It plays a primary role in maintaining rotational control of the pelvis, functioning optimally when the posterior sacroiliac ligaments remain intact.
Pubis to Pubis Ligaments
The symphyseal ligaments, particularly the superior and arcuate (inferior) pubic ligaments, stabilize the anterior ring. The anterior ring acts as a tie strut, contributing approximately 40% of the overall stiffness of the pelvic ring.
Spine to Pelvis Ligaments
Additional stability is conferred by ligamentous attachments between the lumbar spine and the pelvic ring:
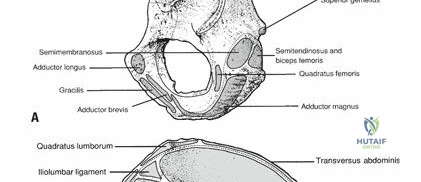
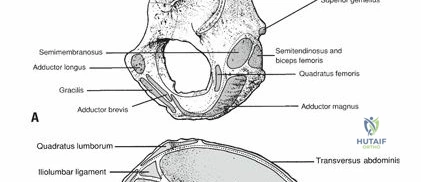
* The iliolumbar ligaments originate from the L4 and L5 transverse processes and insert on the posterior iliac crest.
* The lumbosacral ligaments originate from the transverse process of L5 and extend to the ala of the sacrum.
From a biomechanical perspective, transversely placed ligaments (short posterior sacroiliac, anterior sacroiliac, iliolumbar, and sacrospinous ligaments) primarily resist rotational forces. Vertically placed ligaments (long posterior sacroiliac and sacrotuberous ligaments) resist vertical shear forces.
Neurovascular Considerations
Surgical approaches to the pelvis are fraught with neurovascular hazards. The internal iliac artery and its branches, notably the superior gluteal artery (exiting the greater sciatic notch) and the obturator artery, are frequently implicated in major pelvic hemorrhage. The "corona mortis," an anastomotic connection between the external iliac/inferior epigastric and obturator vessels, courses over the superior pubic ramus and must be meticulously ligated during anterior approaches (e.g., Stoppa approach).

Neurologically, the lumbosacral plexus is at high risk during both injury and surgical fixation. The L5 nerve root courses directly over the sacral ala, making it highly vulnerable during sacral fractures, sacroiliac dislocations, and the placement of iliosacral screws. The sciatic nerve exits the greater sciatic foramen and is at risk during posterior approaches and retractor placement.
Indications and Contraindications
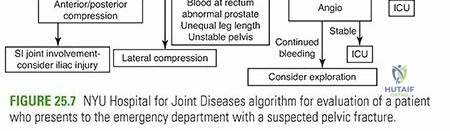
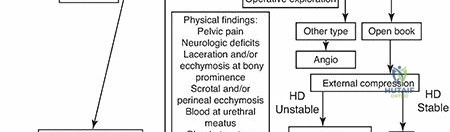
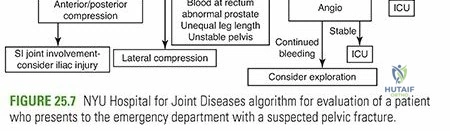
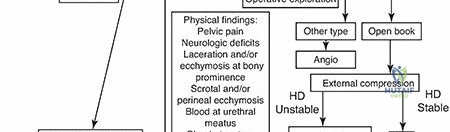
The decision to proceed with operative versus non-operative management depends on the hemodynamic status of the patient, the mechanical stability of the pelvic ring, and the presence of associated injuries.
| Clinical Scenario | Operative Indications | Non Operative Indications | Contraindications to Immediate Definitive Fixation |
|---|---|---|---|
| Hemodynamic Status | Persistent instability requiring pelvic packing/binder; definitive fixation once stable. | Hemodynamically stable from presentation. | Profound shock, coagulopathy, severe acidosis (Damage Control Orthopedics required). |
| Anterior Ring Injury | Symphyseal diastasis > 2.5 cm (APC II/III); irreducible overlapping pubic symphysis. | Symphyseal widening < 2.5 cm with intact posterior ligaments (APC I). | Active infection or massive contamination in the suprapubic region. |
| Posterior Ring Injury | SI joint displacement > 1 cm; complete posterior disruption (Vertical Shear); sacral fractures with neuro deficit. | Impacted sacral fractures (LC I) with minimal displacement; stable SI joint. | Severe soft tissue degloving (Morel-Lavallée lesion) over the planned surgical approach. |
| Fragility Fractures | Intractable pain preventing mobilization; progressive displacement (FFP Type III/IV). | Pain controlled with oral analgesics; ability to mobilize (FFP Type I/II). | Extreme medical comorbidities precluding anesthesia. |
| Open Fractures | All open pelvic fractures require emergent debridement and stabilization. | N/A | N/A |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is critical to achieving anatomic reduction, restoring pelvic stability, and avoiding iatrogenic complications.
Imaging Protocols and Classification
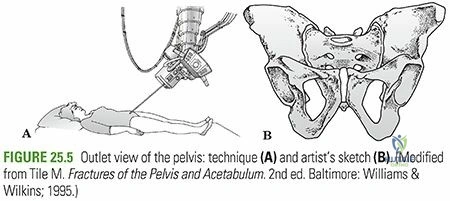
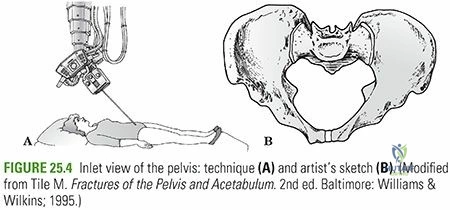
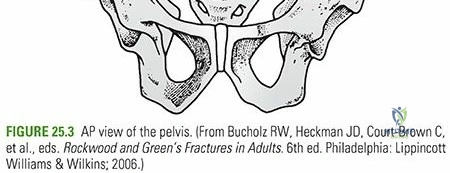
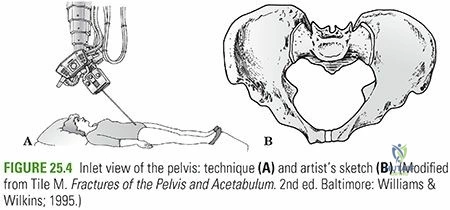
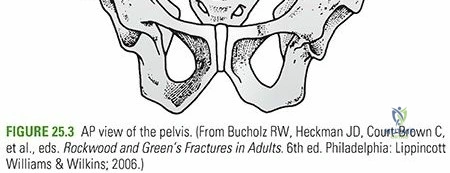
Standard radiographic evaluation includes an anteroposterior (AP) view of the pelvis, supplemented by specialized Inlet and Outlet views.
* Inlet View: Directed 25 to 30 degrees caudad. This view best evaluates the AP translation of the hemipelvis, internal/external rotation (open/closed book), and sacral impaction.
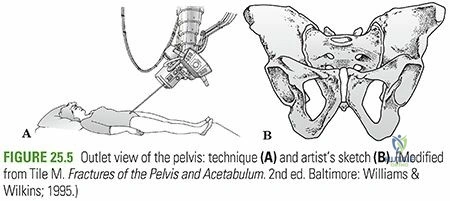
* Outlet View: Directed 40 to 45 degrees cephalad. This view best evaluates superior/inferior translation (vertical shear), sacral foraminal fractures, and leg length discrepancy.

High-resolution computed tomography (CT) with two-dimensional multiplanar reformats and three-dimensional surface rendering is the gold standard. CT is essential for defining posterior ring anatomy, identifying occult sacral dysmorphism, evaluating the neuroforamina, and planning percutaneous screw trajectories.
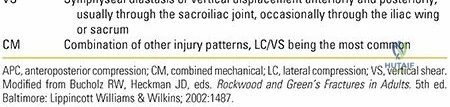
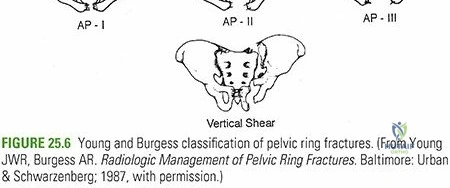
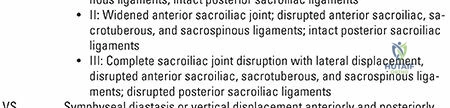
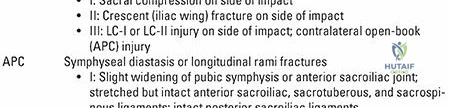
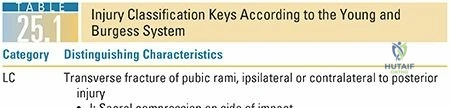
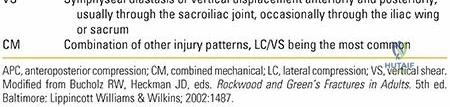
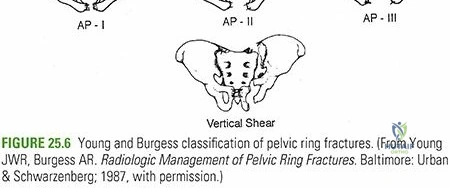
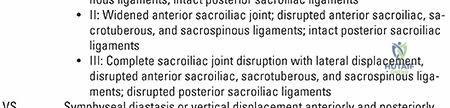
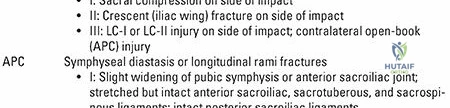
Fractures are classically categorized using the Young-Burgess classification system, which is based on the mechanism of injury (Anteroposterior Compression [APC], Lateral Compression [LC], Vertical Shear [VS], and Combined Mechanism [CM]). The Tile classification focuses on mechanical stability (Type A: rotationally and vertically stable; Type B: rotationally unstable, vertically stable; Type C: rotationally and vertically unstable).

Patient Positioning and Operating Room Setup
Positioning is dictated by the planned approach and the specific injury pattern.
* Supine Position: Most commonly utilized. The patient is placed on a completely radiolucent Jackson table or a flat OSI table. This allows for unrestricted fluoroscopic access for Inlet, Outlet, and Judet views. It is ideal for anterior approaches (Pfannenstiel, Stoppa), anterior external fixation, and percutaneous iliosacral screw placement.
* Prone Position: Utilized for direct open reduction of sacral fractures, posterior sacroiliac joint plating, or tension band wiring. The abdomen must hang free to decrease venous pressure and minimize intraoperative bleeding.
* Lateral Decubitus: Occasionally used for specific iliac wing fractures or combined acetabular-pelvic injuries requiring a Kocher-Langenbeck approach.
The patient should be prepped and draped widely, typically from the costal margin to the bilateral knees, allowing for manipulation of the lower extremities to aid in closed reduction maneuvers.
Detailed Surgical Approach and Technique
The surgical management of pelvic ring injuries requires a comprehensive armamentarium of approaches, ranging from minimally invasive percutaneous techniques to extensile open exposures.
Anterior Surgical Approaches
Pfannenstiel Approach
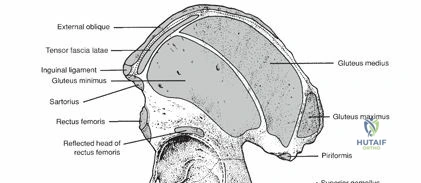
The Pfannenstiel approach is the workhorse for addressing symphyseal diastasis. A transverse incision is made two fingerbreadths superior to the pubic symphysis. The anterior rectus sheath is incised transversely, and the rectus abdominis muscles are split vertically along the linea alba. Subperiosteal dissection exposes the superior pubic rami and the symphysis. Reduction is typically achieved using a Jungbluth clamp or Weber tenaculum applied to screws placed in the pubic tubercles. Fixation is achieved with a multi-hole symphyseal plate (often a 4- to 6-hole dynamic compression plate or specialized pre-contoured symphysis plate).
Modified Stoppa Approach
The Modified Stoppa approach provides excellent access to the anterior pelvic ring, quadrilateral plate, and posterior column. The patient is supine with the hip flexed to relax the iliopsoas. Following a Pfannenstiel skin incision, the rectus abdominis is split, and dissection proceeds extraperitoneally along the posterior aspect of the superior pubic ramus. The corona mortis must be identified and ligated. The iliopectineal fascia is divided to allow access to the true pelvis. This approach allows for the placement of long infrapectineal plates spanning from the symphysis to the sacroiliac joint.
Posterior Surgical Approaches
Direct posterior approaches are reserved for highly displaced sacral fractures, nonunions, or situations where percutaneous reduction is impossible. A longitudinal midline or paramedian incision is made. The gluteus maximus is split in line with its fibers, or its origin is elevated from the ilium. The posterior sacroiliac ligaments are exposed. Open reduction is performed, and fixation is achieved using anterior SI joint plating (via an anterior approach) or posterior tension band plating. Due to the high risk of wound complications and infection, open posterior approaches are utilized sparingly.
Percutaneous Fixation Techniques
Iliosacral Screw Fixation
Percutaneous iliosacral screw fixation is the gold standard for stabilizing the posterior pelvic ring. It requires meticulous fluoroscopic technique.
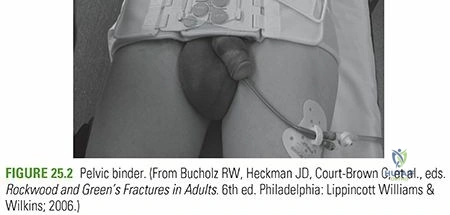
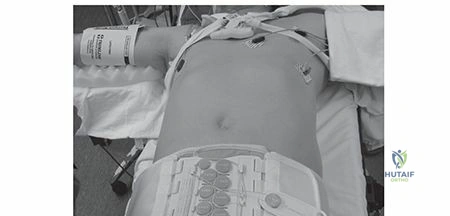
1. Reduction: Closed reduction is achieved via skeletal traction, internal rotation of the limbs, or the use of a pelvic binder.
2. Trajectory Planning: The surgeon must evaluate the preoperative CT for sacral dysmorphism (present in up to 30% of patients), which alters the safe corridor for S1 screws, often necessitating an S2 trajectory or an oblique "transiliac-transsacral" screw.
3. Guidewire Placement: A guidewire is advanced from the lateral ilium under continuous alternating fluoroscopy.
* Lateral View: Ensures the wire is within the sacral alar slope, avoiding the L5 nerve root anteriorly and the sacral neuroforamina posteriorly.
* Inlet View: Ensures the wire remains within the sacral body, avoiding anterior breach into the pelvis or posterior breach into the spinal canal.
* Outlet View: Ensures the wire is superior to the S1 foramen and inferior to the S1 endplate.
4. Fixation: Once the guidewire is perfectly positioned, a cannulated drill is used, followed by the insertion of a 7.0 mm or 7.3 mm partially threaded (for compression) or fully threaded (for position) cannulated screw.
Anterior Subcutaneous Internal Fixation (INFIX)
For anterior ring instability, particularly in obese patients where external fixators are poorly tolerated, the INFIX technique is an option. Pedicle screws are placed into the supra-acetabular corridor (dense bone column extending from the anterior inferior iliac spine toward the sciatic notch). A subcutaneous rod is tunneled through the bikini line, connecting the bilateral screws. This provides a biomechanically robust anterior tension band without the complications of percutaneous pins.
Retrograde Superior Pubic Ramus Screws
For pubic root or ramus fractures, a retrograde medullary screw can be placed percutaneously. The entry point is the pubic tubercle. Under fluoroscopic guidance (Inlet, Outlet, and Obturator Oblique views), a guidewire is passed through the superior pubic ramus, across the acetabular dome, and into the posterior ilium, followed by a fully threaded cannulated screw.
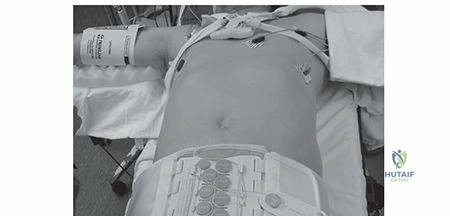
Damage Control and External Fixation
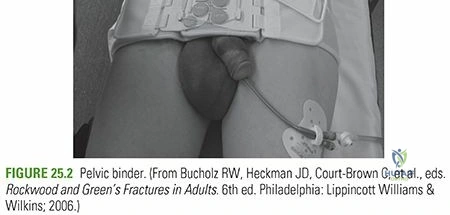
In the hemodynamically unstable patient, rapid mechanical stabilization is required. A pelvic binder centered over the greater trochanters is the first line of treatment. If the patient requires laparotomy or prolonged ICU resuscitation, an external fixator is applied.
* Iliac Crest Pins: Rapidly placed but biomechanically inferior. Pins are inserted between the inner and outer tables of the anterior iliac crest.
* Supra-acetabular Pins: Biomechanically superior. Pins are placed through the AIIS, directed toward the posterior superior iliac spine (PSIS). This provides excellent control of the posterior ring and does not interfere with subsequent abdominal surgery.
Complications and Management
Pelvic ring injuries are associated with a profound complication profile due to the high-energy nature of the trauma and the complex regional anatomy.
| Complication | Incidence | Etiology and Risk Factors | Management and Salvage Strategy |
|---|---|---|---|
| Acute Hemorrhage | 10 - 40% | Venous plexus disruption (80%); Arterial injury (20%, e.g., superior gluteal artery). | Pelvic binder, massive transfusion protocol, preperitoneal pelvic packing, angioembolization. |
| Neurologic Injury | 10 - 15% | L5 or S1 nerve root traction/compression from sacral fractures or vertical shear. | Decompression if fracture fragments impinge neuroforamina; iatrogenic screw breach requires immediate removal/revision. |
| Urogenital Injury | 5 - 15% | Bladder rupture, urethral avulsion (highly associated with severe anterior ring displacement). | Suprapubic catheterization, retrograde urethrogram prior to Foley placement, delayed urologic reconstruction. |
| Surgical Site Infection | 2 - 10% | Open posterior approaches, Morel-Lavallée lesions, obesity, prolonged operative time. | Aggressive serial debridement, negative pressure wound therapy, retention of hardware if stable, hardware removal if ununited/loose. |
| Venous Thromboembolism | 5 - 20% | Endothelial injury, venous stasis from immobility, hypercoagulable state of trauma. | Mechanical prophylaxis immediately; chemical prophylaxis (LMWH) within 24 hours of hemostasis. IVC filter if anticoagulation contraindicated. |
| Malunion / Nonunion | 3 - 5% | Inadequate initial reduction, unrecognized posterior instability, premature weight-bearing. | Complex reconstructive osteotomies, revision internal fixation, autologous bone grafting for nonunions. |
Special attention must be given to the Morel-Lavallée lesion, a closed deg
Clinical & Radiographic Imaging