Sacroiliac Joint Fractures: Understanding Causes & Treatment
Key Takeaway
Here are the crucial details you must know about Sacroiliac Joint Fractures: Understanding Causes & Treatment. **Fractures sacroiliac joint** are serious posterior pelvic ring injuries, often presenting as fracture-dislocations, involving the inherently unstable articulation between the innominate bones and the sacrum. This critical joint connects the pelvis to the spine. Its stability relies heavily on strong ligamentous structures, and these injuries are associated with diverse morbidities and high-impact trauma.
Introduction and Epidemiology
Pelvic ring disruptions represent a formidable challenge in orthopedic traumatology, characterized by a diverse assortment of morbidities and mortality rates ranging from 0% to 50% depending on the severity of associated injuries. These fractures typically result from high-energy mechanisms such as motor vehicle collisions, motorcycle crashes, and falls from significant heights. Fractures and dislocations of the pelvis involve, in broad terms, injuries to the anterior and posterior structures of the pelvic ring. While injuries to the anterior pelvic ring include symphyseal disruption and pubic body or rami fractures, it is the posterior pelvic ring—comprising iliac wing fractures, sacroiliac joint dislocations, fracture-dislocations, and sacral fractures—that dictates the overall mechanical stability of the pelvis.
The posterior pelvic ring is the primary weight-bearing axis of the human body, transferring axial loads from the spine to the lower extremities. Consequently, the implications and treatment of damage to these structures vary widely across a broad spectrum of injury patterns, combinations of injuries, and degrees of displacement. The Young-Burgess and Tile classification systems remain the standard for categorizing these injuries based on the vector of force (Anteroposterior Compression, Lateral Compression, Vertical Shear) and the resulting mechanical instability. This comprehensive surgical reference focuses on the operative management, specifically Open Reduction and Internal Fixation and percutaneous stabilization, of displaced sacral fractures and severe sacroiliac joint disruptions.
Surgical Anatomy and Biomechanics
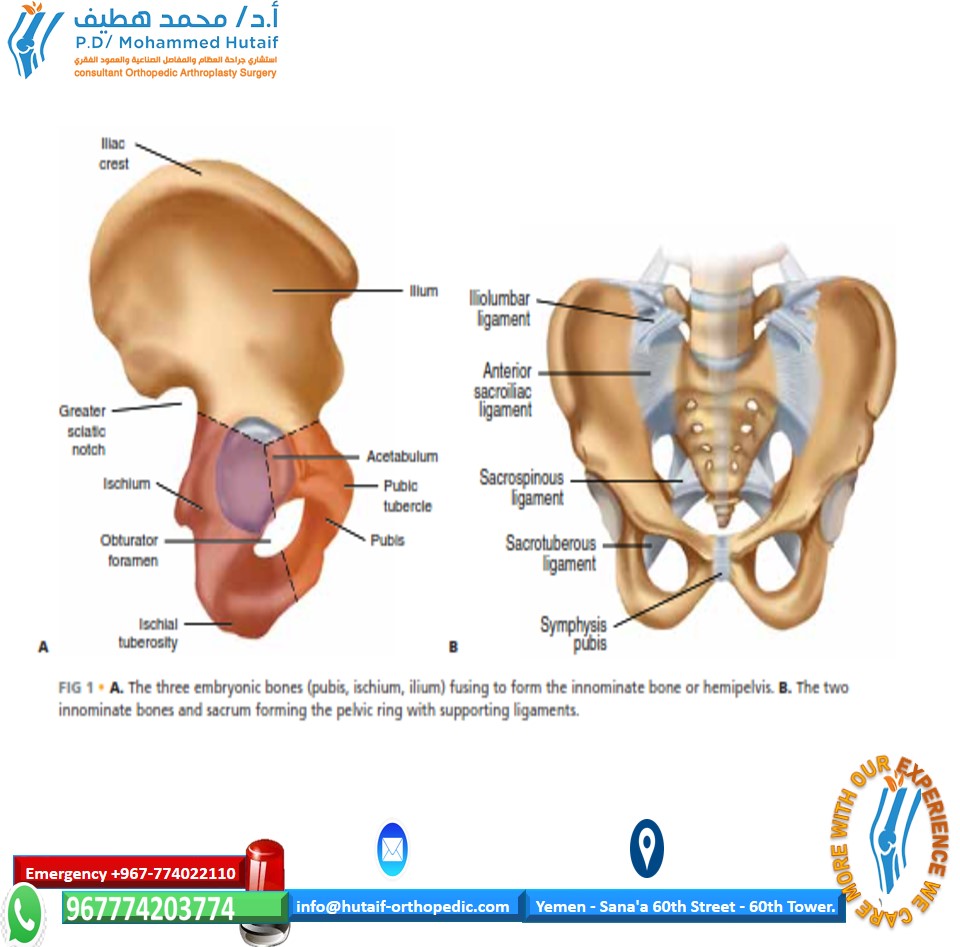
The pelvis is a complex osseoligamentous ring structure composed of the two hemipelves, or innominate bones, and the sacrum. Each innominate bone is formed as the result of the embryologic fusion of three bony elements: the ilium, the pubis, and the ischium. Anteriorly, the two innominate bones are joined at the pubic symphysis, a symphyseal joint that contributes no more than 15% to overall pelvic ring stability. Posteriorly, the innominate bones articulate with the wings, or alae, of the sacrum via the strong sacroiliac joints to complete the ring.
Osseous Architecture and Sacral Dysmorphism
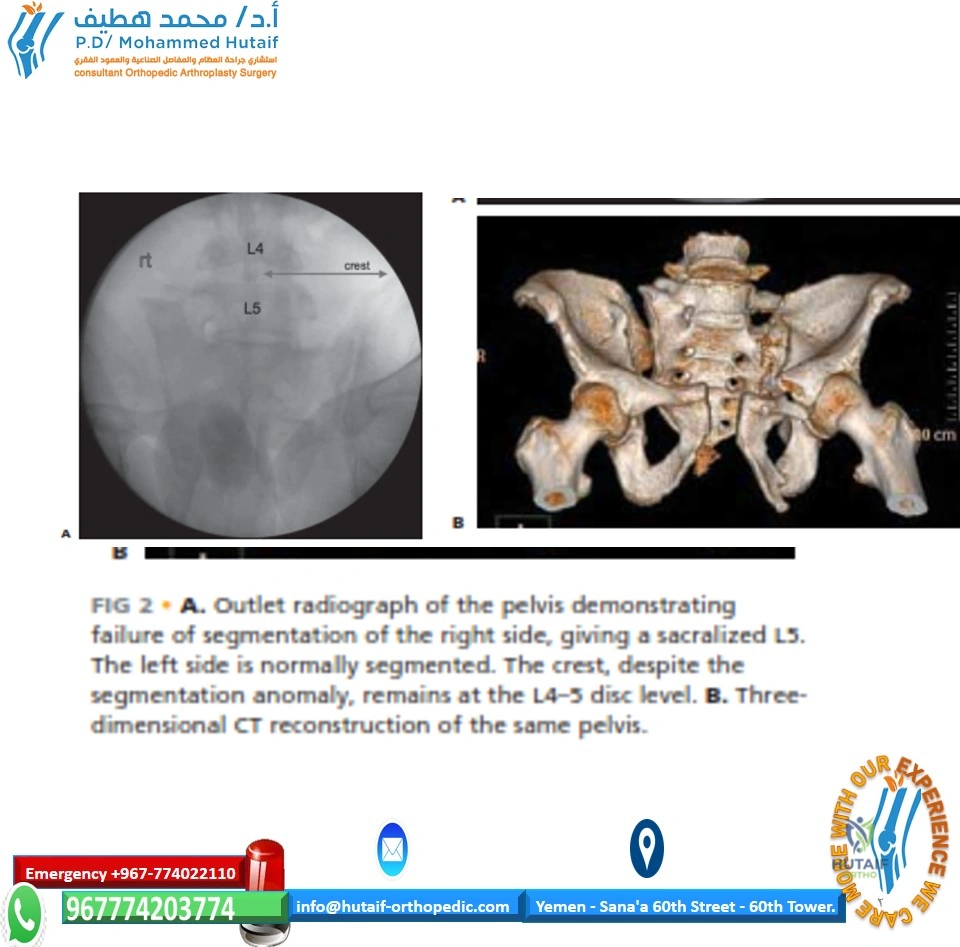
The sacrum represents the terminal structural segment of the spinal column, connecting the appendicular skeleton to the axial trunk. Being wedge-shaped in both the coronal and axial planes, the sacrum forms a keystone articulation with the innominate bones. Because the sacrum is essentially a spinal element, it is highly subject to segmentation abnormalities and dysmorphisms. Most commonly, segmentation anomalies such as a lumbarized S1 and a sacralized L5 will be present.
Identifying sacral dysmorphism is a critical prerequisite for safe surgical intervention, particularly for iliosacral screw placement. The only definitive method to ascertain which segmentation defect is present is to count down from the first thoracic vertebra, identified by transverse processes inclined cephalad. As a general radiographic rule of thumb, the top of the iliac crest is usually at the same level as the L4-L5 disc space. Dysmorphic sacra typically present with upper sacral segments that are not recessed within the pelvis, acute alar slopes, and non-circular, irregularly shaped upper sacral neural foramina. These morphologic variations drastically alter the radiographic landmarks and the available osseous "safe zones" required to safely place iliosacral screws.
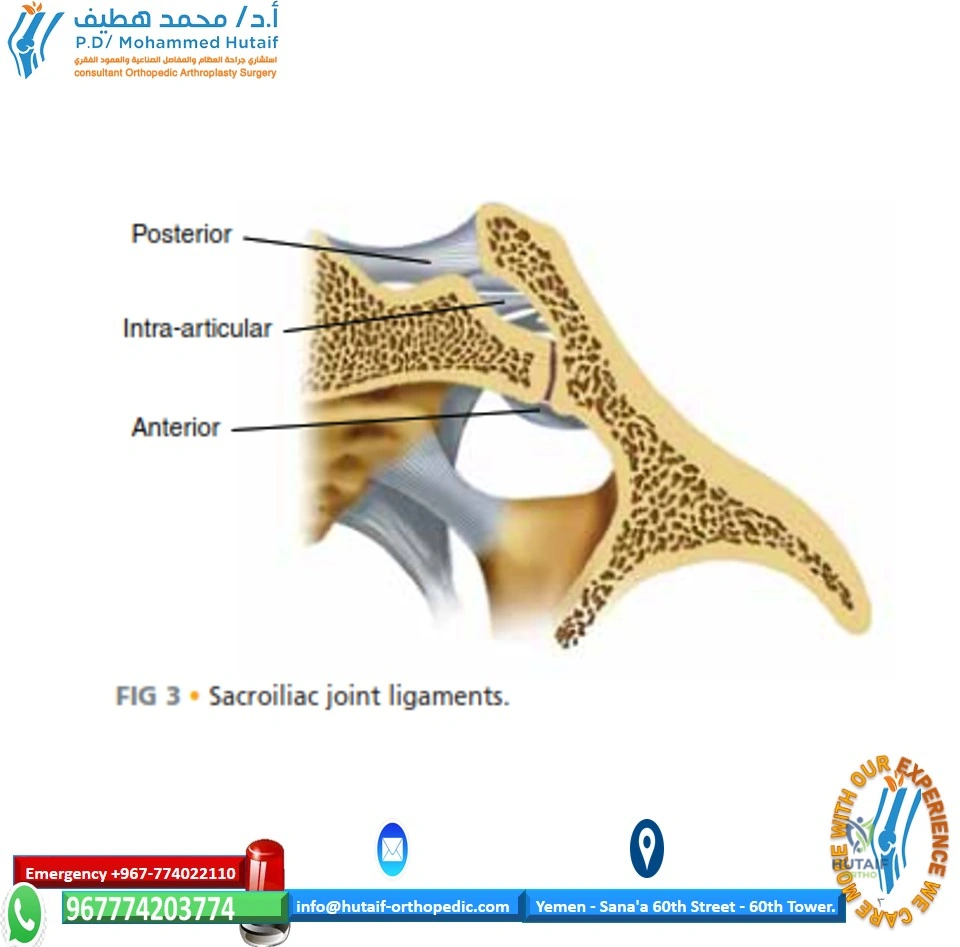
Ligamentous Support and Biomechanical Stability
By virtue of its keystone shape and spatial orientation, the osseous sacroiliac joint is inherently unstable. The maintenance of posterior pelvic ring integrity is wholly dependent on the robust support provided by the surrounding ligamentous structures. The interosseous sacroiliac ligaments are the strongest ligaments in the body and are the primary stabilizers against anteroposterior translation.
With axial loading, the natural tendency is for each hemipelvis to externally rotate and translate in a cephalad and posterior direction. The pelvic ligaments are structured and positioned to resist these specific deforming forces. The sacrotuberous ligaments resist sheer and flexion, while the sacrospinous ligaments resist external rotation. Disruption of these posterior tension band structures results in profound rotational and vertical instability.
Neurovascular Relationships
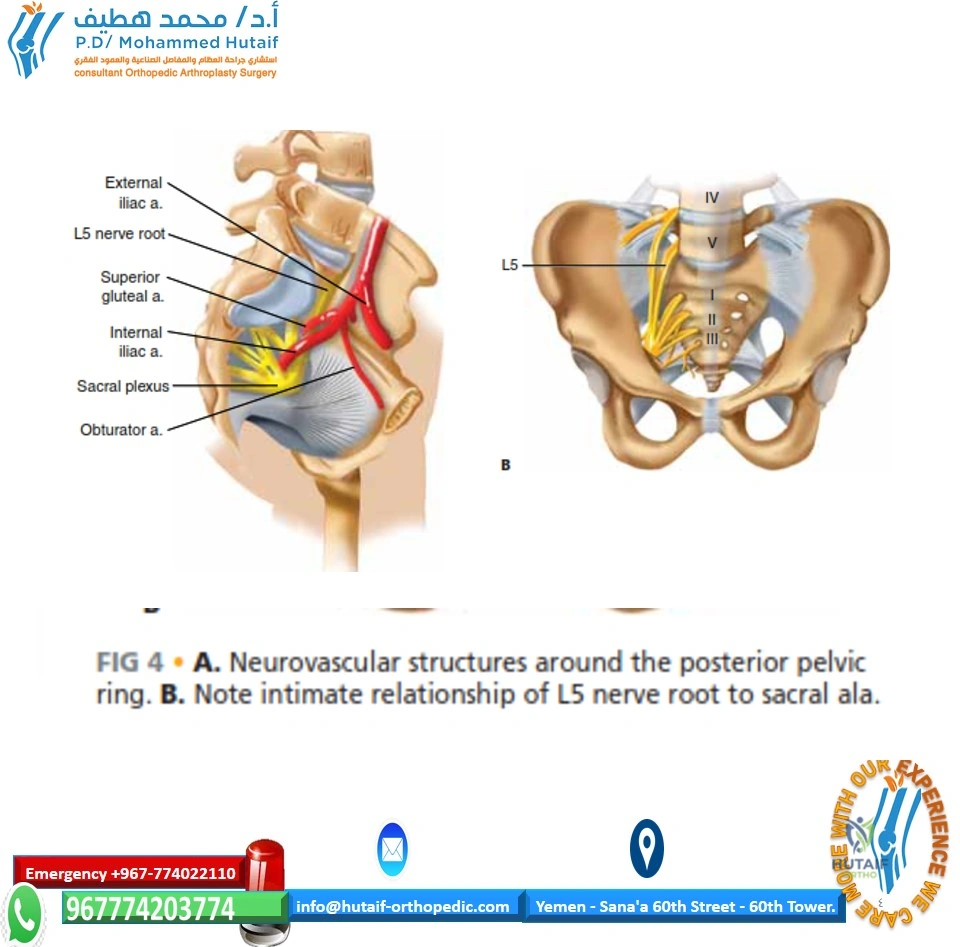
The neurovascular anatomy surrounding the posterior pelvic ring is unforgiving. Anterior to the pubic bodies and symphysis lies the bladder, separated only by a thin layer of fat and the potential space of Retzius. Posteriorly, the intimate relationship of the L5 nerve root to the superior aspect of the sacral ala as it courses to join the lumbosacral plexus is a key anatomic feature that must be vigilantly respected during reduction and stabilization of posterior pelvic ring injuries. Furthermore, the superior gluteal neurovascular bundle exits the pelvis through the greater sciatic notch, immediately adjacent to the inferior margin of the sacroiliac joint, making it highly susceptible to iatrogenic injury during posterior approaches or clamp placement.
Indications and Contraindications
The decision to proceed with operative management of sacroiliac joint disruptions and sacral fractures hinges on the hemodynamic status of the patient, the degree of mechanical instability, and the presence of neurologic compromise. The primary goal of intervention is to restore the anatomic volume of the pelvis, stabilize the posterior weight-bearing axis, and permit early mobilization.
Operative vs Non Operative Management
| Clinical Scenario | Management Strategy | Rationale and Key Considerations |
|---|---|---|
| Hemodynamic Instability | Emergent Operative / Damage Control | Application of pelvic binder or external fixator; pre-peritoneal packing or angioembolization for hemorrhage control prior to definitive internal fixation. |
| APC II and APC III Injuries | Operative | Disruption of anterior and posterior ligaments leads to rotational (and vertical in APC III) instability requiring anterior plating and posterior SI fixation. |
| Vertical Shear Injuries | Operative | Complete osteoligamentous disruption requires rigid posterior fixation (ilioscacral screws, transiliac-transsacral screws, or spinopelvic fixation) to resist vertical displacement. |
| Sacral Fracture with Neurologic Deficit | Operative | Decompression of the sacral foramina or central canal may be indicated alongside stabilization, particularly in Denis Zone II and III fractures. |
| Open Pelvic Fractures | Operative | Requires emergent irrigation, debridement, and stabilization; often necessitates diverting colostomy to prevent sepsis. |
| LC I Injuries (Stable) | Non-Operative | Intact posterior tension band; typically managed with protected weight-bearing and aggressive physical therapy. |
| Severe Medical Comorbidities | Non-Operative | Prohibitive surgical risk may necessitate non-operative management even in the setting of displacement, accepting malunion. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is paramount for successful outcomes in pelvic ring reconstruction. The standard radiographic trauma series includes Anteroposterior, Inlet, and Outlet views of the pelvis. The Inlet view optimally evaluates anteroposterior translation and internal/external rotational deformity, while the Outlet view assesses vertical displacement and cephalad migration of the hemipelvis.
However, plain radiography is insufficient for definitive preoperative planning. High-resolution Computed Tomography with 2D multiplanar reconstructions (axial, coronal, and sagittal) and 3D surface rendering is mandatory. CT imaging allows for precise characterization of sacral comminution, identification of impacted fracture margins, assessment of the neural foramina, and critical evaluation of upper sacral segment dysmorphism to map safe corridors for hardware placement.
Patient Positioning and Operating Room Setup
Positioning is dictated by the chosen surgical approach, which in turn is driven by the fracture pattern.
Supine Positioning:
For percutaneous iliosacral screw fixation, anterior approaches to the sacroiliac joint, and symphyseal plating, the patient is positioned supine on a completely radiolucent Jackson table or a flat carbon-fiber table. A bump may be placed under the lumbosacral junction to facilitate access. The C-arm fluoroscope must have unimpeded access to swing between AP, Inlet, Outlet, and true lateral views of the sacrum. The patient's arms should be positioned across the chest to allow the C-arm to arc over the torso for steep Inlet views.
Prone Positioning:
When a direct posterior approach to the sacrum or sacroiliac joint is required—such as for tension band plating, direct decompression of sacral nerve roots, or application of spinopelvic fixation (triangular osteosynthesis)—the patient is positioned prone. Chest rolls or a specialized prone frame are utilized to allow the abdomen to hang free, reducing intra-abdominal pressure and consequently decreasing epidural venous bleeding. The C-arm is positioned to enter from the side of the table, ensuring the ability to obtain orthogonal views of the posterior ring.
Detailed Surgical Approach and Technique
Surgical management of posterior pelvic ring disruptions requires a nuanced understanding of various approaches and fixation strategies. The choice of technique depends on the specific injury morphology, the presence of comminution, and the surgeon's experience.
Percutaneous Iliosacral Screw Fixation
Percutaneous iliosacral screw fixation has become the workhorse technique for stabilizing sacroiliac joint disruptions and sacral fractures. It offers the advantage of minimal soft tissue dissection, thereby reducing the risk of wound complications and infection.
Technique:
1. Fluoroscopic Setup: Obtain perfect Inlet, Outlet, and Lateral views of the sacrum. The Lateral view must superimpose the greater sciatic notches to identify the alar slope and the anterior sacral cortex.
2. Incision and Guidewire Placement: A stab incision is made over the lateral gluteal region. A guide pin is advanced through the gluteal musculature to the outer table of the ilium.
3. Trajectory: On the Lateral view, the pin is directed into the safe zone of the S1 or S2 vertebral body, remaining inferior to the iliac cortical density (alar slope) and anterior to the neural foramina. On the Inlet view, the pin must remain within the sacral body, avoiding anterior cortical breach into the pelvis. On the Outlet view, the pin must remain parallel to the superior endplate of S1, avoiding the S1 neuroforamen inferiorly and the L5-S1 disc space superiorly.
4. Drilling and Fixation: Once the guidewire is confirmed in all three planes, a cannulated drill is used to breach the outer iliac cortex. A partially threaded 7.0mm or 7.3mm cannulated cancellous screw with a washer is inserted to provide compression across the SI joint. For sacral fractures, fully threaded screws may be utilized to act as a position screw and prevent over-compression of the neural foramina.
Anterior Approach to the Sacroiliac Joint
The anterior approach is primarily indicated for sacroiliac joint dislocations or fracture-dislocations (e.g., crescent fractures) where percutaneous reduction is unachievable or when there is anterior sacral comminution that precludes safe iliosacral screw placement.
Technique:
1. Incision: The lateral window of the ilioinguinal approach is utilized. An incision is made along the anterior two-thirds of the iliac crest, extending toward the Anterior Superior Iliac Spine (ASIS).
2. Dissection: The abdominal musculature is elevated off the iliac crest. The iliacus muscle is subperiosteally elevated from the inner table of the ilium, proceeding medially toward the sacroiliac joint.
3. Neurovascular Protection: The L5 nerve root courses over the sacral ala just medial to the SI joint; meticulous retraction is required. The iliolumbar artery may need to be ligated to mobilize the soft tissues adequately.
4. Reduction and Plating: Jungbluth clamps or a pelvic reduction frame can be applied using Schanz pins placed in the iliac crest and the dense bone of the sacral ala. Once anatomic reduction is achieved, orthogonal plating is performed across the anterior aspect of the SI joint using specialized pelvic reconstruction plates.
Posterior Approach and Spinopelvic Fixation
Direct posterior approaches are reserved for highly comminuted sacral fractures, vertical shear injuries with profound instability, or cases requiring open nerve root decompression.
Technique:
1. Incision: A longitudinal midline or paramedian incision is made over the sacrum and posterior ilium.
2. Dissection: The gluteus maximus is split in line with its fibers or elevated from its origin on the posterior ilium and sacrum. The multifidus and erector spinae muscles are retracted medially.
3. Direct Reduction: The posterior superior iliac spine (PSIS) and the sacral lamina are exposed. Direct visualization allows for the removal of interposed soft tissue or bone fragments from the SI joint or sacral fracture site.
4. Fixation Options:
* Tension Band Plating: Plates are placed across the posterior ilium to the sacrum, acting as a tension band against anterior opening.
* Transiliac-Transsacral Screws: For highly unstable U-type or H-type sacral fractures, screws are passed from one ilium, through the sacral body, and into the contralateral ilium, providing superior biomechanical strength.
* Spinopelvic Fixation (Triangular Osteosynthesis): In cases of severe vertical instability (spinopelvic dissociation), pedicle screws are placed in the L4 and/or L5 vertebrae and connected via rods to long iliac screws placed down the gluteal pillar. This construct bypasses the comminuted sacrum entirely, bridging the intact axial spine directly to the stable innominate bones.
Complications and Management
The surgical management of sacroiliac joint fractures and sacral disruptions carries a high complication profile due to the high-energy nature of the trauma, the complex regional anatomy, and the demanding surgical techniques required.
Common Surgical Complications
| Complication | Incidence | Prevention and Salvage Strategy |
|---|---|---|
| Iatrogenic Neurologic Injury (L5/S1) | 5% - 10% | Prevention: Meticulous fluoroscopic imaging; understanding sacral dysmorphism; use of neuromonitoring (EMG/SSEP). Salvage: Immediate removal or repositioning of aberrant hardware; open decompression if hematoma or bone fragment is compressing the root. |
| Surgical Site Infection | 2% - 15% | Prevention: Minimize posterior soft tissue stripping; optimize patient nutrition; meticulous hemostasis to prevent Morel-Lavallée lesion infection. Salvage: Aggressive serial irrigation and debridement; targeted intravenous antibiotics; retention of hardware until union if stable. |
| Hemorrhage / Vascular Injury | 1% - 5% | Prevention: Avoid plunging drills anterior to the sacrum (internal iliac vessels) or inferior to the SI joint (superior gluteal artery). Salvage: Pelvic packing; emergent interventional radiology for angioembolization. |
| Hardware Failure / Loss of Reduction | 5% - 12% | Prevention: Recognize severe instability patterns preoperatively; utilize supplemental fixation (e.g., spinopelvic constructs for vertical shear). Salvage: Revision open reduction and internal fixation with augmented constructs; bone grafting for nonunion. |
| Malunion / Pelvic Asymmetry | 10% - 20% | Prevention: Precise intraoperative fluoroscopy; use of intraoperative 3D imaging (O-arm) if available. Salvage: Corrective pelvic osteotomies (highly complex, reserved for severe symptomatic deformity). |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation of patients with operatively treated posterior pelvic ring injuries must be carefully tailored to the specific fracture pattern, the rigidity of the internal fixation, and the patient's overall polytrauma burden.
Weight-Bearing Restrictions:
For the majority of operatively treated sacroiliac joint disruptions and sacral fractures, patients are restricted to toe-touch weight-bearing (TTWB) or non-weight-bearing (NWB) on the affected side for a minimum of 6 to 12 weeks. In cases of bilateral posterior ring injuries or spinopelvic fixation, patients may be restricted to bed-to-chair transfers to avoid catastrophic hardware failure.
Deep Vein Thrombosis (DVT) Prophylaxis:
Pelvic trauma patients are at an exceptionally high risk for venous thromboembolism. Chemical prophylaxis (e.g., Low Molecular Weight Heparin or direct oral anticoagulants) should be initiated as soon as it is deemed surgically and neurologically safe, typically within 24 to 48 hours postoperatively, and continued for 4 to 6 weeks. Mechanical prophylaxis with sequential compression devices should be utilized continuously while the patient is immobile.
Physical Therapy Progression:
Early physical therapy focuses on upper extremity conditioning, contralateral lower extremity strengthening, and safe transfer techniques. Once radiographic evidence of early consolidation is observed (typically around the 6 to 8-week mark), progressive weight-bearing is initiated. Full weight-bearing and advanced gait training are usually achieved by 3 to 4 months postoperatively, though maximum medical improvement may take up to 12 to 18 months.
Summary of Key Literature and Guidelines
The evolution of pelvic ring reconstruction is heavily grounded in landmark biomechanical and clinical studies. The classification of pelvic ring injuries by Young and Burgess remains the cornerstone for understanding the mechanism of injury and predicting the resulting instability patterns. Their work dictates the necessity of posterior stabilization in rotationally and vertically unstable patterns.
Routt et al. pioneered the widespread adoption of percutaneous iliosacral screw fixation, delineating the critical radiographic landmarks and the concept of sacral dysmorphism. Their extensive literature on the "safe zones" of the upper sacral segments has drastically reduced the incidence of iatrogenic neurologic injury and remains essential reading for all orthopedic trauma surgeons.
Current guidelines from the Orthopaedic Trauma Association (OTA) and the AO Foundation emphasize a multidisciplinary approach to pelvic trauma. The integration of advanced imaging modalities, such as intraoperative 3D fluoroscopy and navigation, is increasingly recommended to enhance the safety and accuracy of posterior ring fixation. Furthermore, recent literature highlights the superiority of spinopelvic fixation (triangular osteosynthesis) in the management of highly comminuted, vertically unstable sacral fractures, demonstrating significantly lower rates of mechanical failure compared to traditional iliosacral screws alone. Adherence to these established principles and continuous engagement with emerging technologies are imperative for optimizing clinical outcomes in this challenging patient population.
Clinical & Radiographic Imaging
