Open Reduction and Internal Fixation of the Pubic Symphysis and Pelvic Ring

Key Takeaway
Open reduction and internal fixation (ORIF) of the pubic symphysis is a critical procedure for restoring anterior pelvic ring stability in rotationally and vertically unstable pelvic fractures. Utilizing a Pfannenstiel approach, surgeons achieve anatomical reduction via specialized clamps and secure the symphysis with a multi-hole reconstruction plate. For Tile Type C injuries, supplementary posterior ring fixation—such as iliosacral screws or transiliac plating—is mandatory to counteract vertical shear forces and optimize functional outcomes.
Comprehensive Introduction and Patho-Epidemiology
The pelvic ring is a complex, multi-planar osteoligamentous structure that relies synergistically on both anterior and posterior elements to maintain biomechanical stability and facilitate the transfer of axial loads from the spine to the lower extremities. Disruptions of the pubic symphysis and the broader pelvic ring are hallmark presentations of high-energy blunt trauma, most frequently resulting from motor vehicle collisions, motorcycle crashes, pedestrian-versus-auto accidents, and falls from significant heights. These injuries are rarely isolated; they are typically accompanied by a constellation of concomitant life-threatening injuries, including traumatic brain injury, blunt thoracic trauma, hollow viscus rupture, and devastating hemodynamic instability secondary to massive retroperitoneal hemorrhage. The mortality rate for patients presenting with hemodynamically unstable pelvic ring injuries remains staggeringly high, historically reported between 15% and 40%, underscoring the critical nature of rapid, protocol-driven initial management.
Understanding the patho-epidemiology of these injuries requires a firm grasp of the prevailing classification systems, predominantly the Young-Burgess and Tile classifications, which categorize fracture patterns based on the vector of the deforming force and the resultant mechanical instability. Anteroposterior compression (APC) injuries typically result in an external rotation force on the hemipelvis, leading to pubic symphysis diastasis. While an APC I injury involves isolated symphyseal widening less than 2.5 cm with intact posterior ligaments, APC II and APC III injuries represent a progressive failure of the anterior sacroiliac, sacrotuberous, sacrospinous, and ultimately posterior sacroiliac ligaments. Lateral compression (LC) injuries, conversely, drive the hemipelvis inward, often resulting in overlapping pubic rami fractures and varying degrees of posterior sacral crush or ligamentous disruption. Vertical shear (VS) injuries, or Tile Type C patterns, represent the most catastrophic failure of the pelvic ring, characterized by complete osteoligamentous dissociation of the hemipelvis and resultant multi-planar (rotational and vertical) instability.
The historical management of severe pelvic ring disruptions was largely non-operative, relying on prolonged skeletal traction, pelvic slings, and spica casting. However, this paradigm was fraught with profound morbidity, including severe malunion, chronic debilitating pelvic pain, leg length discrepancies, and the myriad complications associated with prolonged recumbency (deep vein thrombosis, pulmonary embolism, decubitus ulcers, and severe deconditioning). The modern era of orthopedic traumatology has witnessed a definitive shift toward early operative intervention. Open reduction and internal fixation (ORIF) of the pubic symphysis, coupled with appropriate posterior ring stabilization, is now universally recognized as the gold standard for restoring the anatomical integrity of the pelvis.
While external fixation and pelvic binders play an indispensable role in the acute resuscitation phase—effectively reducing pelvic volume, promoting the tamponade of venous bleeding, and providing provisional rotational stability—they are biomechanically inadequate as definitive fixation for highly unstable patterns. Specifically, anterior external fixation cannot control the posterior translation or vertical displacement inherent in Tile Type C / Young-Burgess APC III and VS injuries. Consequently, the definitive management of these complex injuries demands a highly sophisticated approach, requiring the surgeon to execute precise anatomical reduction and rigid internal fixation to restore the anterior tension band and the posterior weight-bearing arch, thereby optimizing the patient's potential for functional recovery.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of pelvic anatomy is the absolute prerequisite for safely executing surgical exposures and internal fixation within this anatomically dense and unforgiving region. The osseous pelvic ring is formed by the articulation of the two innominate bones (ilium, ischium, and pubis) with the sacrum posteriorly and with each other anteriorly at the pubic symphysis. The pubic symphysis itself is a non-synovial amphiarthrodial joint, characterized by a fibrocartilaginous interpubic disc interposed between the hyaline cartilage-covered articular surfaces of the pubic bodies. This joint is statically stabilized by a robust ligamentous complex, with the superior pubic ligament and the arcuate (inferior) pubic ligament providing the primary resistance to tensile and shear forces.
The posterior pelvic ring represents the true biomechanical keystone of the pelvis, responsible for transferring the entire axial load of the torso to the appendicular skeleton. The sacroiliac (SI) joints are stabilized by an immensely powerful network of ligaments. The anterior sacroiliac ligaments resist external rotation, while the interosseous and short posterior sacroiliac ligaments are the strongest ligaments in the body, suspending the sacrum between the ilia and resisting vertical shear forces. The accessory pelvic ligaments—the sacrotuberous and sacrospinous ligaments—act as critical secondary stabilizers. The sacrotuberous ligament resists sagittal rotation (flexion) of the sacrum, while the sacrospinous ligament resists external rotation of the hemipelvis. Disruption of these posterior and accessory ligaments is the defining pathophysiological event that transitions a rotationally unstable injury into a vertically unstable one.
The neurovascular anatomy surrounding the surgical approaches to the anterior and posterior pelvic ring is notoriously complex and highly vulnerable to iatrogenic injury. Anteriorly, the surgeon must be acutely aware of the corona mortis—an anatomic variant present in up to 30-40% of patients, representing a vascular anastomosis between the obturator and external iliac systems (either arterial, venous, or both) that crosses the superior pubic ramus. Inadvertent laceration of the corona mortis during a Pfannenstiel or Stoppa approach can result in catastrophic, difficult-to-control hemorrhage. Furthermore, the urogenital structures, specifically the bladder and the membranous urethra, reside immediately posterior to the pubic symphysis in the Space of Retzius. These structures are frequently compromised by the initial trauma and are at high risk during drilling and retractor placement.
Posteriorly, the lumbosacral plexus and the iliac vessels dictate the safe corridors for internal fixation. The L5 nerve root courses directly over the anterior aspect of the sacral ala, making it highly susceptible to injury from anteriorly misdirected iliosacral screws or aggressive anterior plating of the SI joint. The S1 and S2 nerve roots exit through the anterior sacral foramina and are at risk during the placement of trans-sacral implants or during the compression of transforaminal sacral fractures. Biomechanically, the pelvis functions as a closed ring; thus, a single break in the ring is rare and implies plastic deformation of the articulations elsewhere. The anterior structures function primarily as a tie-rod, resisting tension and external rotation, while the posterior structures form a weight-bearing arch. Successful surgical reconstruction mandates the restoration of both the anterior tie-rod and the posterior arch to re-establish the physiological load-sharing capacity of the pelvis.
Exhaustive Indications and Contraindications
The decision-making process regarding the operative management of pelvic ring injuries is highly nuanced, requiring the surgeon to synthesize the patient's hemodynamic status, the biomechanical stability of the fracture pattern, the presence of concomitant injuries, and the patient's baseline physiological reserve. The primary goal of intervention is to restore the anatomical alignment of the pelvic ring to facilitate early mobilization and minimize long-term functional deficits, but this must never supersede the immediate imperative of preserving the patient's life.
Absolute indications for operative intervention include hemodynamically unstable pelvic fractures that fail to respond to initial resuscitation and non-invasive stabilization (e.g., pelvic binder). In these extremis scenarios, emergent external fixation or preperitoneal pelvic packing is indicated as a life-saving damage control measure, with definitive internal fixation delayed until physiological optimization is achieved. For definitive management, absolute indications include pubic symphysis diastasis exceeding 2.5 cm (which signifies failure of the anterior ligamentous complex and often the pelvic floor), vertically unstable fracture patterns (Tile Type C / Young-Burgess VS), open pelvic fractures, and injuries associated with visceral or neurovascular compromise that require concomitant surgical exploration (e.g., bladder rupture requiring laparotomy).
Relative indications encompass a broader spectrum of injuries, most notably the "gray zone" of Young-Burgess APC II injuries. While some APC II injuries with minimal displacement may be managed non-operatively, those demonstrating dynamic instability on stress examination (either clinical or fluoroscopic under anesthesia) or those in patients who require early mobilization to prevent pulmonary complications are best served by ORIF. Furthermore, significant leg length discrepancy (>1.5 cm) or rotational deformity that would severely impair gait biomechanics serves as a strong relative indication for surgical correction. The presence of intractable pain preventing mobilization in lateral compression injuries, despite seemingly minimally displaced rami fractures, is increasingly recognized as an indication for percutaneous fixation.
Contraindications to definitive pelvic ORIF are primarily dictated by the patient's systemic physiological state and the local soft tissue envelope. Severe hemodynamic instability, profound coagulopathy, acidosis, and hypothermia (the "lethal triad") are absolute contraindications to prolonged, definitive surgical exposures; these patients require damage control orthopedics. Local soft tissue compromise, such as massive Morel-Lavallée lesions (closed degloving injuries) over the surgical approach, severe contamination from open bowel injuries, or active superficial infections, strongly contraindicate immediate internal fixation due to the prohibitive risk of deep hardware infection. In such cases, external fixation is maintained until the soft tissue envelope has adequately recovered.
Indications and Contraindications Summary
| Category | Specific Clinical Scenarios | Rationale for Management Decision |
|---|---|---|
| Absolute Indications | Symphyseal diastasis > 2.5 cm; Vertical Shear (Tile Type C); Open pelvic fractures. | Restores anterior tension band; Addresses multi-planar instability; Facilitates necessary debridement. |
| Relative Indications | APC II injuries with dynamic instability; Severe intractable pain in LC injuries; Leg length discrepancy > 1.5 cm. | Prevents delayed displacement; Allows early mobilization; Restores physiological gait mechanics. |
| Absolute Contraindications | Hemodynamic instability (lethal triad); Active local infection; Severe intra-abdominal contamination (e.g., gross fecal spillage). | Risk of intraoperative mortality; Prohibitive risk of deep hardware infection (requires damage control instead). |
| Relative Contraindications | Severe osteopenia/osteoporosis; Non-ambulatory baseline status; Severe closed degloving (Morel-Lavallée) over incision site. | High risk of hardware pull-out; Minimal functional benefit; High risk of wound necrosis and secondary infection. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful pelvic ring reconstruction. The complexity of the three-dimensional anatomy demands a comprehensive imaging protocol. Standard anteroposterior (AP) radiographs provide a general overview of the injury, but they are insufficient for detailed planning. Orthogonal Inlet and Outlet radiographs are mandatory. The Inlet view (directed approximately 25-30 degrees caudally) optimally visualizes the pelvic brim, assessing anterior-posterior translation of the hemipelvis and internal/external rotational deformity. The Outlet view (directed approximately 40-45 degrees cephalad) projects the sacrum en face, allowing for the precise evaluation of vertical displacement of the hemipelvis, sacral foraminal fractures, and superior/inferior translation of the pubic symphysis.
In the modern era, a fine-cut computed tomography (CT) scan with two-dimensional multiplanar reformats (axial, coronal, and sagittal) and three-dimensional surface-rendered reconstructions is an absolute requirement for any patient undergoing definitive pelvic ORIF. The CT scan is invaluable for delineating occult sacral comminution, assessing the exact morphology of sacroiliac joint fracture-dislocations (e.g., crescent fractures), and identifying the presence of intra-articular bone fragments within the hip joint. Furthermore, preoperative templating using digital software allows the surgeon to anticipate the required length and curvature of the symphyseal plate, the optimal trajectory and length of iliosacral screws, and the necessity for specialized reduction tools or supplementary fixation constructs.
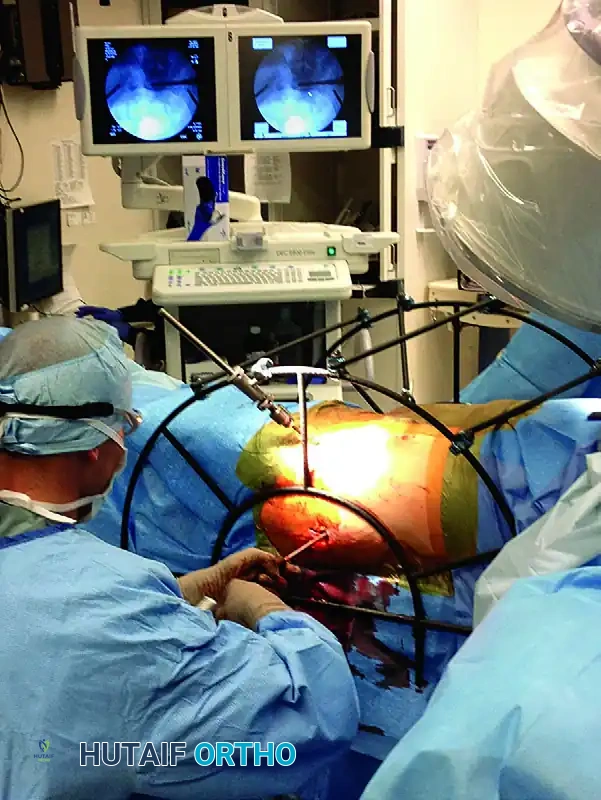
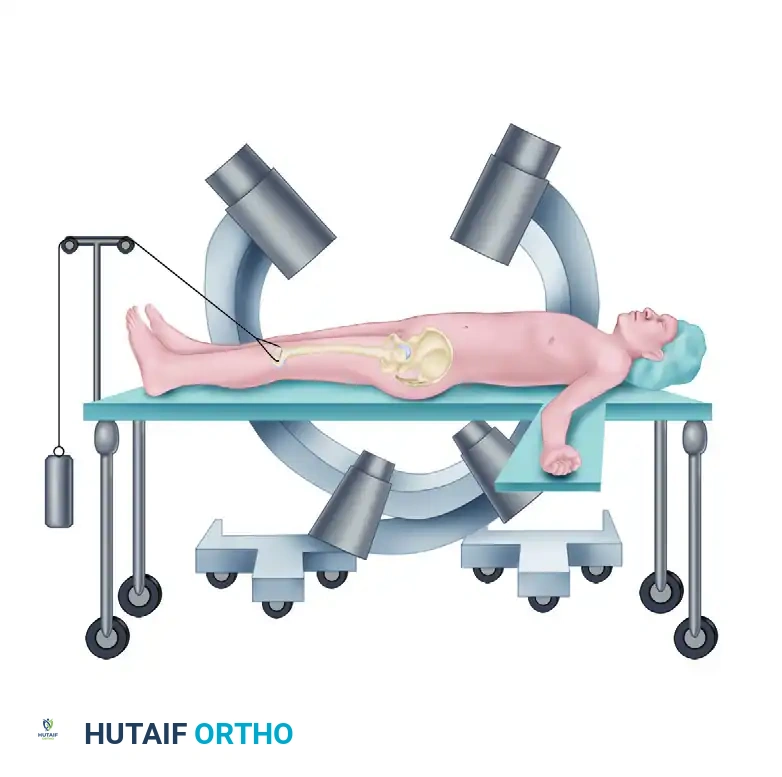
Patient positioning and operating room setup must be executed with exacting precision. The patient is placed strictly supine on a fully radiolucent operating table, typically a Jackson table with a radiolucent flat top. This setup is non-negotiable, as unimpeded intraoperative fluoroscopy is mandatory for confirming both the anterior reduction and the safe trajectory of any posterior pelvic fixation. The C-arm must have free range to swing from a true AP to the requisite steep Inlet and Outlet angles without obstruction from the table base or the pedestal. The bilateral lower extremities should be maintained in internal rotation and slight flexion, often achieved by taping the toes together or using a specialized bump. This maneuver relaxes the iliopsoas musculature and the external rotators of the hip, significantly reducing the deforming forces on the hemipelvis and aiding in the provisional closure of the symphyseal diastasis.
Preparation and draping must be extensive, anticipating the need for multiple surgical approaches and the application of skeletal traction. The abdomen is prepped from the costal margins down to the mid-thighs bilaterally, ensuring the area distal to the pubic tubercles and the bilateral greater trochanters are widely accessible. A Foley catheter must be inserted by the urology or trauma team prior to draping to decompress the bladder, which minimizes its volume in the Space of Retzius and aids in the intraoperative identification of the urethra by palpation. If a concomitant urethral injury is suspected (evidenced by blood at the meatus or a high-riding prostate), a retrograde urethrogram must be performed, and suprapubic catheterization may be required prior to definitive orthopedic intervention.
Step-by-Step Surgical Approach and Fixation Technique
The Pfannenstiel Approach to the Anterior Ring
The Pfannenstiel approach is the workhorse incision for accessing the pubic symphysis and the medial aspect of the superior pubic rami. It provides excellent, extensile exposure while minimizing morbidity to the abdominal wall musculature. The skin incision is a transverse curvilinear line placed approximately 2 cm superior to the pubic symphysis, extending laterally toward the external inguinal rings. Following the incision, the subcutaneous tissues are sharply divided to expose the rectus abdominis fascia. Hemostasis must be meticulously maintained, particularly concerning the superficial epigastric vessels.
The anterior rectus sheath is incised transversely, mirroring the skin incision. The fascial flaps are mobilized superiorly and inferiorly to expose the underlying rectus abdominis muscle bellies. The linea alba is identified, and the rectus abdominis is incised longitudinally exactly at the decussation of the fibers. It is a critical surgical tenet that the rectus heads must not be transected from their insertion on the pubis. Transection severely compromises the dynamic stability of the abdominal wall and drastically increases the risk of postoperative ventral hernia. Once the rectus muscles are retracted laterally, the surgeon enters the Space of Retzius (the prevesical space). The prevesical fat is carefully mobilized using blunt dissection, and the bladder is gently retracted posteriorly.
⚠️ Surgical Warning
The bladder and urethra are highly vulnerable during this exposure, particularly if a concomitant urologic injury is present or if the anatomy is distorted by severe hematoma. Always use a malleable retractor placed deep into the space of Retzius to physically shield the bladder during drilling, tapping, and screw placement.
Reduction Techniques for the Pubic Symphysis
Achieving an anatomical reduction of the pubic symphysis requires a combination of manual traction, specialized clamps, and a profound understanding of the multiplanar deforming forces. Narrow, sharp Hohmann retractors are placed underneath the rectus muscle bellies and over the superior pubic rami to fully expose the symphyseal articulation. The fibrocartilaginous disc is often avulsed or lacerated; any interposed soft tissue or loose cartilage that blocks reduction must be meticulously debrided.
Provisional reduction is typically achieved using a Weber pointed reduction clamp. The tines of the clamp are placed anteriorly onto the body of the pubis on either side of the symphysis.

It is absolutely critical that the points of the reduction clamp are placed at the exact same horizontal (axial) level on the pubic body. As the clamp is closed, this symmetrical placement ensures that any sagittal plane rotation (flexion/extension of the hemipelvis) is simultaneously reduced. Asymmetric placement will inevitably lead to a malreduction in the sagittal plane, manifesting as a step-off at the superior articular surface.
In fractures with severe cephalad displacement of the hemipelvis (vertical shear), simple clamp reduction is entirely insufficient. The surgeon must apply longitudinal skeletal traction to the ipsilateral distal femur (via a distal femoral traction pin) to bring the hemipelvis down to the correct axial level prior to attempting anterior compression. In severe cases, or in patients with osteoporotic bone where pointed clamps may cut out and cause further iatrogenic fracture, the Jungbluth technique is employed. This involves placing a 4.5-mm cortical screw anteriorly on each side of the symphysis to act as anchor points for a specialized pelvic reduction forceps. To prevent screw pull-out on the displaced side, a small plate and nut construct can be utilized over the screw head, providing a massive mechanical advantage and allowing the surgeon to forcefully manipulate the hemipelvis into anatomical alignment.

Internal Fixation of the Pubic Symphysis
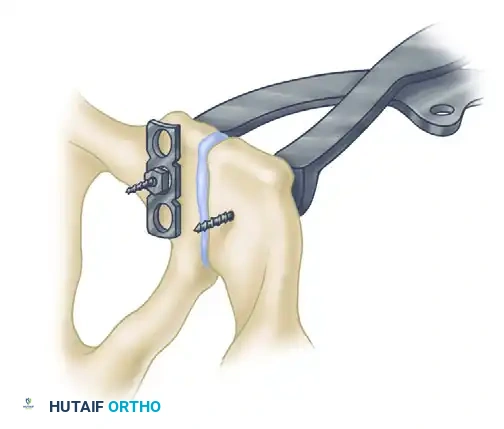
Once a satisfactory anatomical reduction is achieved and provisionally held with clamps, definitive internal fixation is applied. The standard implant is a multi-hole (typically a four- to six-hole) curved 3.5-mm pelvic reconstruction plate. The plate must be meticulously contoured using bending irons to perfectly match the superior surface of the pubic symphysis and the adjacent rami. An improperly contoured plate will cause loss of reduction as the screws are tightened, pulling the bone to the plate rather than securing the bone in its anatomical position.
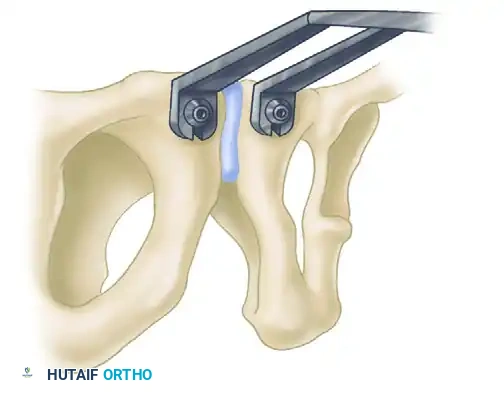
The plate is positioned on the superior surface of the symphysis. The initial drill holes are placed eccentrically away from the fracture line. As the 3.5-mm cortical screws are seated, this eccentric placement yields a small amount of dynamic compression across the symphyseal articulation, significantly enhancing the biomechanical stability of the construct. For highly unstable Tile Type C injuries where posterior fixation is anatomically impossible, medically contraindicated, or deemed insufficient, a double plate construct (one superior, one anterior) may be applied to maximize stiffness and resist orthogonal deforming forces.
Management of the Posterior Pelvic Ring
Definitive posterior fixation is an absolute requirement to regain vertical stability in Tile Type C injuries. External fixation alone is strictly contraindicated as definitive treatment for vertically unstable pelvic fractures because it simply cannot control posterior translation or vertical shear forces. The choice of posterior fixation is dictated by the specific anatomical location of the disruption.
For sacral fractures and sacroiliac joint disruptions, fluoroscopically-directed percutaneous iliosacral (IS) screw fixation is the workhorse technique. Screws are passed from the outer table of the ilium, across the SI joint, and into the dense bone of the sacral body (S1 and occasionally S2). Safe placement requires an intimate understanding of upper sacral anatomy and flawless radiographic technique, utilizing the exact Inlet (25 degrees) and Outlet (42 degrees) views described by Routt to avoid penetration into the sacral foramina or the spinal canal.

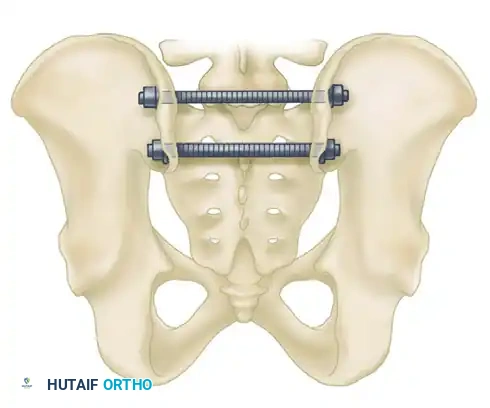
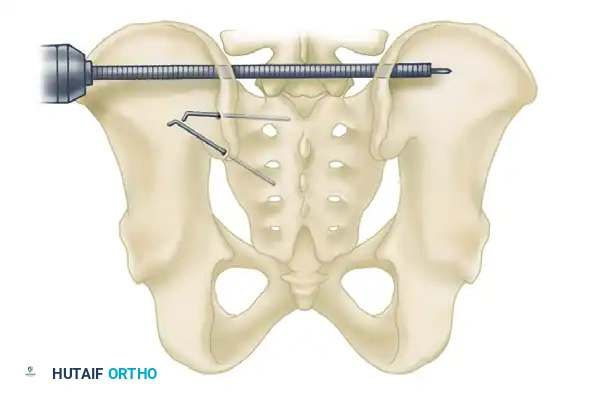
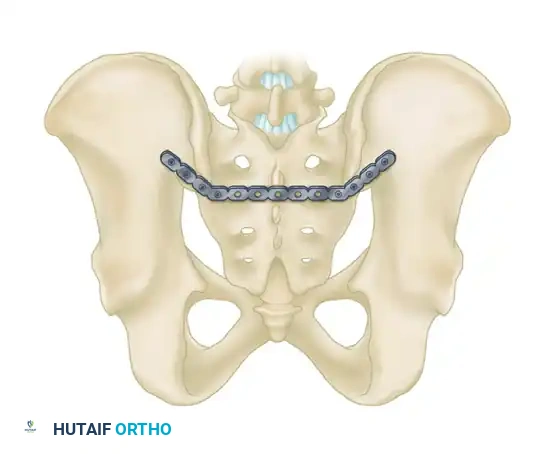
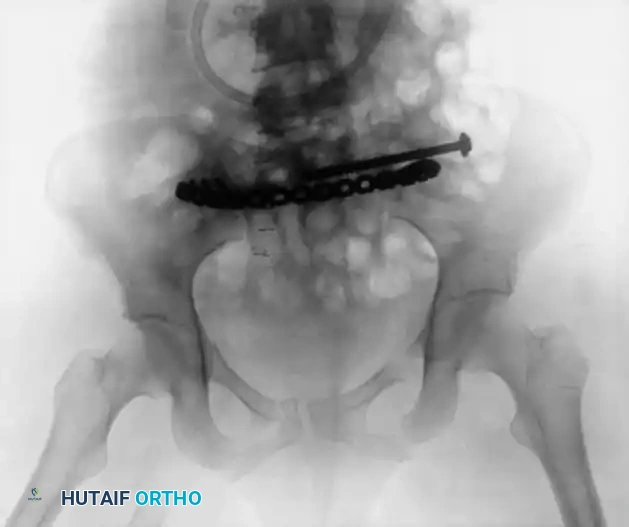
For highly unstable sacral disruptions or comminuted transforaminal fractures where IS screws lack adequate bony purchase, transiliac fixation is utilized. A large Steinmann pin or threaded transiliac rod (8 to 10 mm) is drilled from the outer aspect of one ilium, through the posterior elements of the sacrum, and out the opposite ilium. Alternatively, a reconstruction plate can be contoured and applied posteriorly between the two posterior superior iliac spines (PSIS), acting as a tension band against anterior pelvic opening.
For pure SI joint dislocations or crescent fractures, anterior plating provides direct visualization of the joint. Accessed via an anterior retroperitoneal approach, two or more orthogonal plates are placed across the anterior aspect of the SI joint. This avoids the neurological risks associated with posterior IS screws but requires extensive vascular mobilization.
Obtaining a closed reduction of a vertically displaced posterior ring is notoriously difficult. Advanced percutaneous reduction frames, such as those developed by Starr and Reinert, allow multi-vector, directed forces to be applied to the hemipelvis via Schanz pins placed in the ilium, facilitating precise alignment prior to percutaneous screw insertion without the morbidity of a massive open posterior approach.


Complications, Incidence Rates, and Salvage Management
The operative management of pelvic ring disruptions is associated with a formidable complication profile, reflecting both the severity of the initial high-energy trauma and the technical demands of the surgical reconstruction. Complications can be broadly categorized into early (hemorrhagic, infectious, thromboembolic) and late (hardware failure, malunion, nonunion, chronic pain, and sexual/urologic dysfunction). Anticipating these complications and employing rigorous mitigation strategies is paramount for optimizing patient outcomes.
Infection is a devastating complication, particularly following open posterior approaches, where the soft tissue envelope is frequently compromised by closed degloving injuries (Morel-Lavallée lesions) or severe contusions. Superficial infection rates range from 3% to 10%, while deep infections requiring hardware removal and serial debridement occur in 1% to 5% of cases. The risk is exponentially higher in the presence of an open fracture or a concomitant hollow viscus injury. Meticulous soft tissue handling, the use of closed suction drains in the Space of Retzius, and delaying definitive internal fixation until the soft tissue envelope is viable are critical preventative measures. If a deep infection occurs, aggressive irrigation and debridement, targeted intravenous antibiotic therapy, and retention of stable hardware until bony union is achieved represent the standard salvage protocol.
Neurological injury, either traumatic or iatrogenic, represents a profound source of long-term morbidity. The L5 nerve root is particularly vulnerable during the placement of anterior SI joint plates or misdirected iliosacral screws, while the S1 and S2 nerve roots can be injured by screws entering the sacral foramina or by over-compression of transforaminal sacral fractures. Iatrogenic nerve injury rates have been reported as high as 5% to 10% in complex posterior ring reconstructions. Intraoperative neuromonitoring (somatosensory evoked potentials and spontaneous electromyography) is increasingly utilized to mitigate this risk. Salvage management for iatrogenic injury involves immediate return to the operating room for hardware removal or repositioning, though neurological recovery is often incomplete.
Hardware failure and loss of reduction are typically the result of inadequate initial fixation, failure to recognize and stabilize posterior instability, or patient non-compliance with weight-bearing restrictions. Anterior symphyseal plate breakage or screw pull-out occurs in up to 10% to 15% of cases, often secondary to the physiological micromotion that occurs at the symphysis during normal gait. While asymptomatic hardware failure does not necessitate intervention, symptomatic loss of reduction or nonunion requires revision surgery, often involving bone grafting, the application of orthogonal dual-plate constructs, and augmentation of the posterior ring fixation.
Complications and Salvage Strategies
| Complication | Estimated Incidence | Primary Prevention | Salvage Management |
|---|---|---|---|
| Deep Surgical Site Infection | 1% - 5% (Higher in open/Morel-Lavallée) | Delay ORIF until soft tissues heal; meticulous hemostasis; prophylactic antibiotics. | Serial I&D; targeted IV antibiotics; retain stable hardware until union; suppressive therapy. |
| Iatrogenic Neurologic Injury (L5/S1) | 2% - 10% | Flawless fluoroscopic technique (Inlet/Outlet); intraoperative neuromonitoring. | Immediate hardware removal/repositioning; neuropathic pain management; AFO for foot drop. |
| Hardware Failure / Loss of Reduction | 5% - 15% | Rigid posterior fixation for Tile C; eccentric plate compression; strict NWB protocols. | Revision ORIF with dual plating; autologous bone grafting; supplementary spinopelvic fixation. |
| Deep Vein Thrombosis / PE | 10% - 20% (Without prophylaxis) | Early mobilization; mechanical prophylaxis; LMWH starting 24-48h post-op. | Therapeutic anticoagulation; IVC filter placement if anticoagulation is contraindicated. |
| Urologic / Sexual Dysfunction | 10% - 30% (Largely due to initial trauma) | Protect Space of Retzius with malleable retractors; avoid excessive traction on neurovascular bundles. | Urological consultation; phosphodiesterase inhibitors; urethral reconstruction if strictured. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following pelvic
