Sacral Fractures and Lumbosacral Dislocation: Comprehensive Surgical Management
Key Takeaway
Sacral fractures and lumbosacral dislocations represent complex, high-energy injuries often associated with pelvic ring disruptions. Due to a high initial miss rate, a rigorous clinical index of suspicion is required. Management hinges on accurate classification, such as the Denis and Aihara systems, to dictate operative versus nonoperative care. Surgical intervention is primarily indicated for progressive neurological deficits, unstable fracture-dislocations, and severe sacropelvic deformity, utilizing advanced techniques like triangular osteosynthesis and lumbosacral pedicle screw fixation.
Comprehensive Introduction and Patho-Epidemiology
Sacral fractures and lumbosacral dislocations represent some of the most formidable and technically demanding injuries encountered in orthopedic trauma and spine surgery. Constituting approximately 1% of all spinal fractures, these severe, high-energy injuries are frequently overshadowed by concomitant life-threatening visceral, cranial, or vascular trauma. Because of the complex, multiplanar regional anatomy and the distracting nature of polytrauma, sacral fractures are notoriously difficult to diagnose upon initial clinical presentation. Historically, landmark studies by Lafollete, Levine, and McNiesh have demonstrated that up to 60% of sacral fractures are missed or underappreciated during the primary and secondary trauma surveys, leading to catastrophic delayed neurological presentations and progressive spinopelvic deformity.
The epidemiology of these injuries is inextricably linked to high-velocity trauma. More than 90% of indirect sacral fractures are associated with major pelvic ring disruptions, classifying them as integral components of spinopelvic dissociation syndromes. The most common mechanisms of injury include high-velocity motor vehicle collisions, motorcycle accidents, crush injuries, and falls from significant heights. In the elderly or osteopenic population, however, low-energy falls can result in insufficiency fractures of the sacrum, presenting a distinct pathophysiological entity that mimics the mechanical instability of high-energy trauma but requires a different diagnostic and therapeutic algorithm.
Given the intimate and unforgiving anatomical relationship between the sacrum and the lumbosacral plexus, neurological compromise is a hallmark of these injuries. Between 25% and 50% of high-energy sacral fractures present with an accompanying neurological deficit. The pathophysiology of neural injury ranges from neuropraxia due to transient stretch or contusion, to axonotmesis from direct compression by retropulsed bone fragments, and ultimately neurotmesis resulting from complete transection or severe avulsion of the nerve roots. The specific pattern of neurological deficit is highly dependent on the fracture morphology, the degree of displacement, and the anatomical zone of the sacrum involved.
A high index of clinical suspicion is absolutely mandatory in any polytrauma patient presenting with a pelvic fracture, lower extremity neurological deficits, or unexplained perineal symptoms. A meticulous, protocol-driven neurological examination must be performed and documented as soon as the patient is hemodynamically stable. This assessment must specifically target sacral root dysfunction, evaluating perianal sensation (S2-S4), rectal sphincter tone and voluntary contraction, diminished or absent ankle jerk reflexes (S1), and the presence or absence of the bulbocavernosus reflex. Failure to identify these subtle neurological cues can result in irreversible cauda equina syndrome, condemning the patient to a lifetime of neurogenic bowel, bladder, and sexual dysfunction.
Detailed Surgical Anatomy and Biomechanics
The sacrum functions as the keystone of the pelvic ring, providing the critical biomechanical transition point where the axial load of the spine is transferred to the appendicular skeleton of the lower extremities. Osteologically, the sacrum is formed by the fusion of five sacral vertebrae, creating a robust, kyphotic wedge that articulates superiorly with the L5 vertebra via the lumbosacral intervertebral disc and facet joints, and laterally with the ilia through the sacroiliac (SI) joints. The sacral ala, the thick lateral wings of the upper sacrum, transmit the majority of the axial load. The central sacral canal houses the cauda equina, while the four pairs of anterior and posterior sacral foramina provide egress for the sacral nerve roots. Understanding the Denis classification zones (Zone I: alar; Zone II: foraminal; Zone III: central canal) is critical, as the foraminal region represents the weakest structural point of the sacrum and is highly susceptible to vertical shear forces.
The neurological anatomy of the lumbosacral region is highly complex and vulnerable to traumatic disruption. The L5 nerve root courses anteriorly over the sacral ala, making it uniquely susceptible to traction or compression injuries in Zone I fractures or highly displaced sacroiliac joint disruptions. The S1 through S4 nerve roots exit through their respective anterior sacral foramina to form the sacral plexus, which provides motor innervation to the posterior thigh, leg, and foot, as well as critical parasympathetic autonomic innervation to the pelvic viscera. Zone III fractures, which involve the central sacral canal, pose an extreme risk (up to 87%) to the lower sacral roots, frequently resulting in profound sphincter dysfunction and loss of perineal sensation.
Ligamentous stability is paramount in the lumbosacral junction and pelvic ring. The anterior sacroiliac ligaments are relatively thin, but the posterior sacroiliac ligamentous complex is massive and represents the strongest ligamentous structure in the human body, resisting sheer and bending forces. Additionally, the sacrotuberous and sacrospinous ligaments resist rotational forces and vertical displacement of the sacrum relative to the pelvis. The iliolumbar ligaments, anchoring the L5 transverse processes to the iliac crests, play a crucial role in stabilizing the lumbosacral junction. Disruption of these ligaments, as seen in lumbosacral fracture-dislocations, leads to catastrophic multiplanar instability that cannot be managed with conservative measures.
Biomechanically, the lumbosacral junction is subjected to massive shear forces due to the natural lordosis of the lumbar spine and the sacral slope. The L5-S1 articulation must resist the tendency of the L5 vertebra to slide anteriorly. In the setting of a sacral fracture or lumbosacral dislocation, the normal spinopelvic parameters (Pelvic Incidence, Pelvic Tilt, and Sacral Slope) are acutely deranged. U-shaped or H-shaped sacral fractures result in spinopelvic dissociation, where the upper sacrum and axial spine become mechanically uncoupled from the lower sacrum and the pelvic ring. This results in progressive kyphotic deformity of the sacrum, causing anterior translation of the spine, severe sagittal imbalance, and progressive stretching of the cauda equina over the fracture apex.
Exhaustive Indications and Contraindications
The management of sacral fractures and lumbosacral dislocations requires a highly nuanced, individualized approach that meticulously balances the structural stability of the pelvic ring, the patient's neurological status, and the systemic burden of concomitant polytrauma. The overarching goals of treatment are to decompress compromised neural elements, restore spinopelvic alignment, achieve rigid biomechanical stability to allow for early mobilization, and minimize the profound morbidity associated with prolonged bed rest in the critically ill trauma patient.
Nonoperative management is strictly reserved for structurally stable, non-displaced or minimally displaced fractures in neurologically intact patients. This typically includes isolated Zone I fractures, non-displaced Zone II fractures without foraminal compression, and stable gunshot wounds without progressive deficits. The conservative protocol historically involved strict bed rest for 8 to 12 weeks, sometimes supplemented by a hip spica cast or a custom lumbosacral orthosis (LSO) with thigh extensions. However, prolonged recumbency carries a high risk of deep vein thrombosis, pulmonary embolism, decubitus ulcers, and severe deconditioning. Furthermore, surgeons must remain vigilant for delayed neurological deterioration, which can occur as fracture fragments settle or exuberant callus formation compresses adjacent nerve roots.
Operative intervention is definitively indicated in the presence of progressive neurological impairment, confirmed neural compression from retropulsed bone fragments or traumatically herniated discs, severe sacral deformity (such as highly displaced U-shaped spinopelvic dissociation), and intractable chronic pain secondary to nonunion or malunion. Furthermore, any sacral fracture associated with a hemodynamically stable but mechanically unstable pelvic ring disruption (e.g., APC III, VS, or combined mechanism injuries) mandates surgical stabilization to restore the integrity of the posterior pelvic ring. Lumbosacral dislocations (Aihara Types 1-5) are inherently unstable due to the complete disruption of the articular and ligamentous restraints and universally require open reduction and rigid internal fixation.
Contraindications to surgical intervention must be carefully weighed. Absolute contraindications include profound hemodynamic instability in the acute trauma setting, where damage control orthopedics (e.g., pelvic binders, external fixation, or pre-peritoneal packing) takes precedence over definitive internal fixation. Severe soft tissue compromise, such as massive Morel-Lavallée lesions or open, contaminated wounds over the posterior sacrum, represents a relative contraindication to immediate open posterior approaches due to the unacceptably high risk of deep surgical site infection. In such cases, percutaneous techniques or delayed open reconstruction following soft tissue optimization are preferred.
| Clinical Scenario | Indication for Surgery | Contraindication / Alternative |
|---|---|---|
| Progressive Neurological Deficit | Absolute Indication: Requires emergent decompression and stabilization to salvage nerve root/cauda equina function. | N/A - Life or limb/function-threatening emergency. |
| U-Shaped Sacral Fracture (Spinopelvic Dissociation) | Absolute Indication: Requires lumbopelvic fixation (triangular osteosynthesis) to restore spinopelvic continuity. | Severe posterior soft tissue degloving (Morel-Lavallée) - delay open surgery, consider percutaneous temporary fixation. |
| Non-displaced Zone I Alar Fracture | Not Indicated: Generally heals well with protected weight-bearing. | Surgery contraindicated due to unnecessary risk; manage with mobilization and observation. |
| Hemodynamically Unstable Polytrauma | Contraindicated: Definitive internal fixation is contraindicated. | Utilize damage control: Pelvic binder, anterior external fixator, angiographic embolization. |
| Lumbosacral Dislocation (Aihara Types 1-5) | Absolute Indication: Inherently unstable; requires open reduction, decompression, and rigid lumbopelvic instrumentation. | Poor bone stock (severe osteoporosis) requires specialized techniques (cement augmentation, multi-point fixation). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful surgical execution in complex sacral and lumbosacral trauma. Standard anteroposterior (AP), lateral, pelvic inlet, and pelvic outlet radiographs are mandatory for initial assessment. However, high-resolution computed tomography (CT) with 2D and 3D sagittal and coronal reconstructions is the gold standard for defining fracture morphology, assessing foraminal compromise, and evaluating the integrity of the lumbosacral facet joints. Magnetic resonance imaging (MRI) is strongly recommended for patients with neurological deficits to directly visualize the cauda equina, identify traumatic disc herniations at L5-S1, and assess for epidural hematomas or nerve root avulsions that may not be apparent on CT.
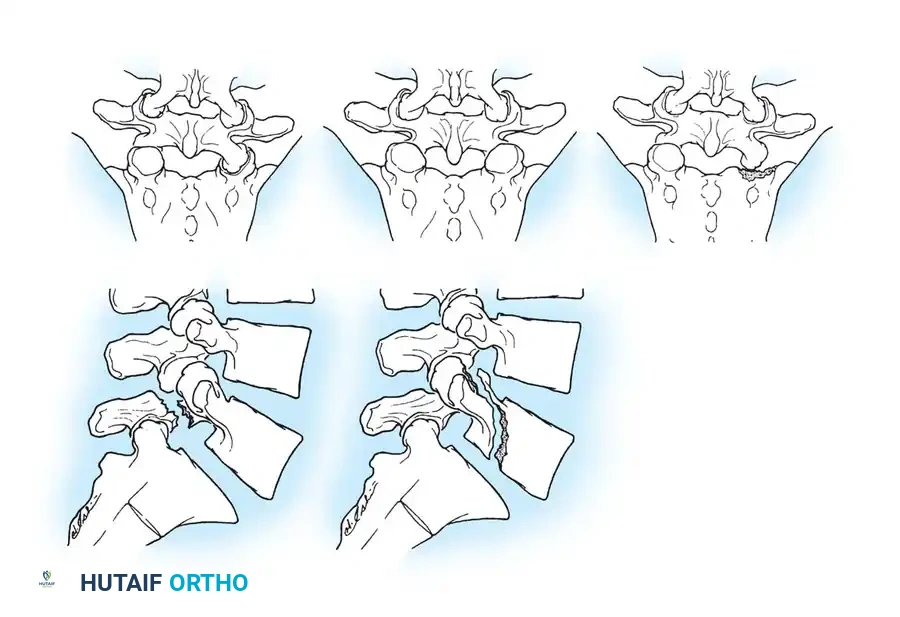
Integration of classification systems is vital during the templating phase. The Schmidek classification aids in understanding the energy vector, while the Denis classification dictates the likelihood of neurological involvement and the necessity for central or foraminal decompression. For lumbosacral dislocations, the Aihara classification guides the surgical strategy.
Templating screw trajectories is a critical component of pre-operative planning, particularly when considering percutaneous iliosacral screws or lumbopelvic fixation. The surgeon must scrutinize the axial and sagittal CT slices to identify sacral dysmorphism—characterized by upper sacral segments that are not recessed within the pelvis, acute alar slopes, and non-circular, narrowed upper sacral neural foramina. In dysmorphic sacra, the safe osseous corridor for an S1 iliosacral screw is obliquely oriented and significantly narrowed, often necessitating the use of S2 screws or alternative lumbopelvic constructs. For lumbopelvic fixation, the trajectories for S2-alar-iliac (S2AI) screws or traditional iliac screws must be templated to ensure adequate length and diameter without breaching the sciatic notch or the acetabulum.
Patient positioning is dictated by the chosen surgical approach but most commonly involves the prone position on a radiolucent Jackson spinal table. This setup allows for continuous biplanar fluoroscopy, which is non-negotiable for these procedures. The abdomen must hang completely free to reduce intra-abdominal venous pressure, thereby minimizing epidural bleeding (Batson's plexus) during decompression. Careful padding of all bony prominences and the eyes is mandatory. Intraoperative neuromonitoring, including somatosensory evoked potentials (SSEPs), motor evoked potentials (MEPs), and spontaneous/triggered electromyography (EMG) of the lower extremities and anal sphincter, is highly recommended to provide real-time feedback during fracture reduction and screw placement.
Step-by-Step Surgical Approach and Fixation Technique
Operative management of these injuries is technically demanding and should be exclusively performed by surgeons with advanced training in spinal or pelvic trauma. The choice of approach—anterior, posterior, or percutaneous—depends entirely on the fracture pattern, the location of neural compression, and the required biomechanical construct.
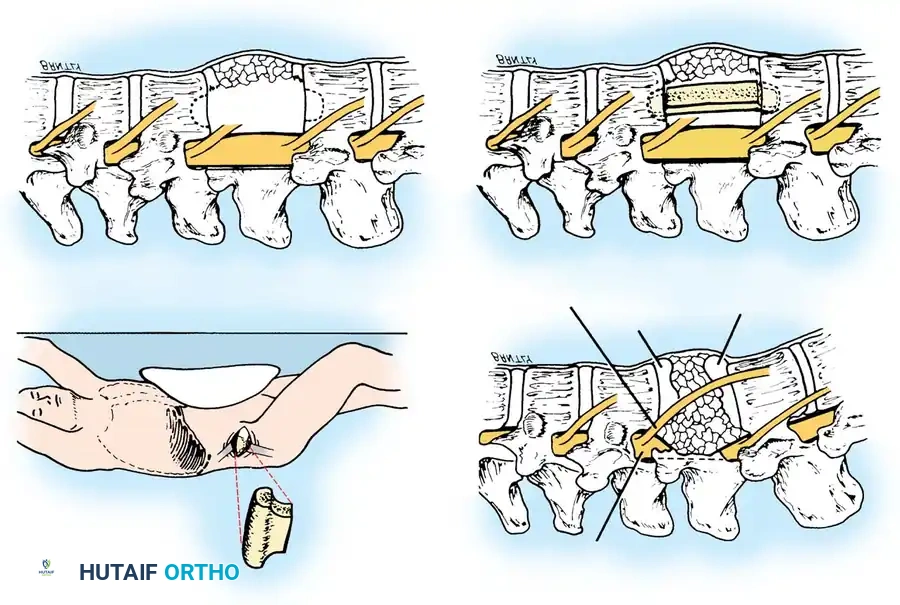
Anterior Decompression and Strut Graft Fusion
For complex burst fractures or fracture-dislocations extending from the lower lumbar spine toward the lumbosacral junction, an anterior retroperitoneal approach provides direct access for decompression of the thecal sac and anterior column reconstruction.
The patient is placed in the lateral decubitus position. A standard retroperitoneal approach is utilized, mobilizing the great vessels (aorta/vena cava or iliac vessels depending on the level) medially. Orientation is facilitated by identifying the psoas muscle and tracing the lumbosacral plexus. Following a thorough discectomy above and below the fractured segment, a corpectomy is performed. Retropulsed bone fragments compressing the thecal sac are meticulously resected using a high-speed burr, Kerrison rongeurs, and reverse-angle curettes until the dura is completely decompressed from pedicle to pedicle. For reconstruction, a tricortical iliac crest strut graft or a titanium mesh cage filled with autograft is impacted into the defect. The graft must be carefully countersunk into the intact vertebral endplates above and below to prevent dislodgement and ensure immediate biomechanical stability, often supplemented by an anterior plate or dual-rod construct.
Posterior Lumbosacral Decompression and Pedicle Screw Fixation
Highly unstable sacral fractures (e.g., spinopelvic dissociation) and lumbosacral dislocations (Aihara Types 1-5) are most effectively managed via a posterior approach, allowing for direct neural decompression, open reduction, and robust lumbopelvic fixation.
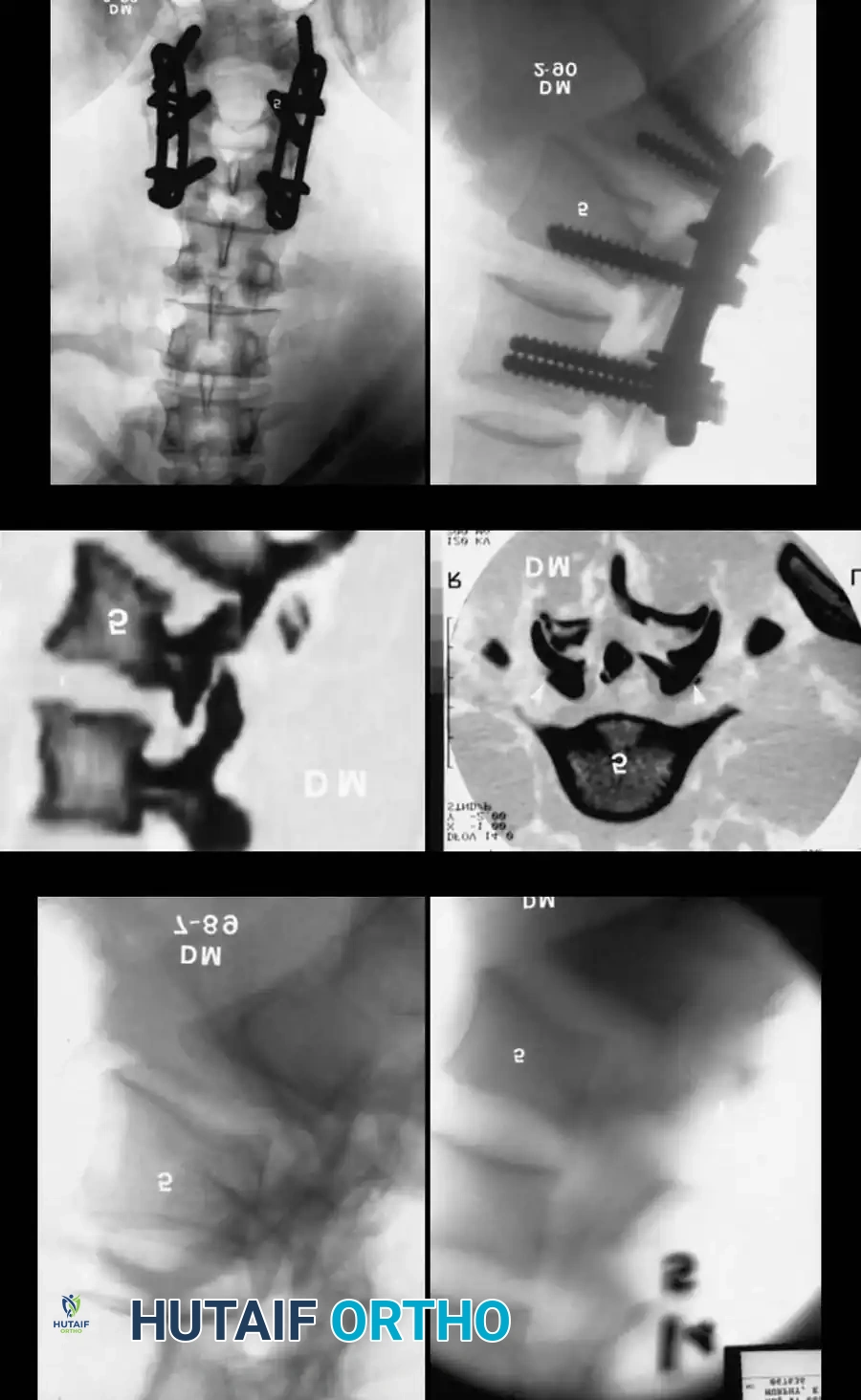
Following prone positioning, a midline longitudinal incision is made, and subperiosteal dissection exposes the posterior elements from L4 down to the sacrum and bilateral posterior superior iliac spines (PSIS). A wide sacral laminectomy is performed to explore the lower lumbar and sacral nerve roots, evacuate epidural hematomas, and remove compressive osseous fragments. This direct visualization is critical before any reduction maneuvers are attempted. Pedicle screws are placed in L4 and L5. For pelvic anchoring, S2-alar-iliac (S2AI) screws or traditional iliac screws are inserted. S2AI screws are increasingly preferred as they remain in-line with the lumbar pedicle screws, minimizing the need for complex rod bending and offset connectors, and they require less soft tissue dissection over the PSIS, reducing wound breakdown risks. Reduction is achieved using a combination of rod contouring, distraction/compression techniques, and direct manipulation of the L5 vertebral body, always under direct visualization of the L5 and S1 nerve roots to prevent iatrogenic traction injuries. This construct, especially when combined with transverse iliosacral screws, creates "triangular osteosynthesis," providing unparalleled multiplanar stability.
Percutaneous Iliosacral Screw Fixation
In select cases of U-shaped sacral fractures or isolated sacroiliac disruptions without significant displacement or neurological deficit, minimally invasive percutaneous techniques offer excellent biomechanical stability with minimal soft tissue morbidity.
This technique relies on absolute mastery of pelvic fluoroscopy. The patient is positioned supine or prone. Under strict fluoroscopic guidance using precise pelvic inlet, pelvic outlet, and true lateral sacral views, a guidewire is advanced from the lateral ilium, across the SI joint, and into the S1 or S2 vertebral body. The inlet view ensures the wire remains within the anterior-posterior confines of the sacral body, while the outlet view confirms the superior-inferior trajectory, avoiding the sacral foramina and the L5-S1 disc space. The lateral view confirms the depth of penetration. Once the trajectory is verified, a cannulated, partially threaded cancellous screw (typically 7.0mm or 7.3mm) is inserted to provide compression across the fracture or SI joint. While highly effective, this technique does not allow for direct neural decompression and is contraindicated in cases of severe sacral dysmorphism where the osseous corridor is too narrow for safe screw passage.
Complications, Incidence Rates, and Salvage Management
The surgical management of sacral fractures and lumbosacral dislocations is fraught with potential complications, stemming from both the severity of the initial trauma and the technical complexity of the reconstructive procedures. Surgeons must be hyper-vigilant during the intraoperative, early postoperative, and late postoperative phases to mitigate these risks.
Intraoperative hemorrhage is a significant concern, particularly during posterior sacral exposures and decompressions. The presacral venous plexus and branches of the superior gluteal artery are highly vulnerable. Massive bleeding can obscure the surgical field and lead to rapid hemodynamic collapse. Meticulous hemostasis using bipolar electrocautery, bone wax, and hemostatic matrix agents is essential. Iatrogenic nerve injury is another devastating intraoperative complication, occurring in up to 5-10% of complex reductions. Over-distraction of the lumbosacral junction or aberrant screw placement can irreversibly damage the L5 or sacral nerve roots. Utilization of intraoperative 3D fluoroscopy (O-arm) or navigation, combined with continuous neuromonitoring, significantly reduces the incidence of hardware misplacement.
Early postoperative complications are dominated by wound healing issues and surgical site infections (SSI). The posterior midline approach over the sacrum is notorious for wound breakdown due to the thin soft tissue envelope, poor local vascularity, and proximity to the perianal region. Infection rates in open posterior spinopelvic reconstructions can approach 10-15%. Prevention relies on meticulous soft tissue handling, minimizing dead space, utilizing subfascial drains, and occasionally employing prophylactic negative pressure wound therapy (incisional VAC). Venous thromboembolism (VTE) is exceptionally common in this polytrauma population; aggressive mechanical and pharmacological prophylaxis must be initiated as soon as it is deemed safe from an epidural hematoma standpoint.
Late complications include hardware failure, loss of reduction, and nonunion. Lumbopelvic constructs are subjected to massive cantilever forces. If osseous fusion does not occur, hardware breakage (typically rod fracture at the lumbosacral junction or screw pullout) is inevitable. Salvage management for nonunion or hardware failure requires revision surgery, often involving extension of the fusion construct, aggressive decortication, and enhancement with robust autograft or bone morphogenetic protein (rhBMP-2).
| Complication | Estimated Incidence | Avoidance Strategy / Salvage Management |
|---|---|---|
| Surgical Site Infection (SSI) | 10 - 15% | Avoidance: Meticulous closure, avoid operating through Morel-Lavallée lesions, incisional VAC. Salvage: Aggressive serial debridement, retention of stable hardware, targeted IV antibiotics, plastic surgery flap coverage. |
| Iatrogenic Nerve Injury | 5 - 10% | Avoidance: Intraoperative neuromonitoring, 3D navigation, direct visualization during reduction. Salvage: Immediate removal/redirection of aberrant hardware, high-dose corticosteroids (controversial). |
| Hardware Failure / Nonunion | 5 - 12% | Avoidance: Rigid triangular osteosynthesis, meticulous bone grafting, strict adherence to post-op weight-bearing restrictions. Salvage: Revision instrumentation, extension of fusion, biological augmentation (autograft/rhBMP-2). |
| Deep Vein Thrombosis / PE | 15 - 20% | Avoidance: Early mobilization, mechanical prophylaxis, LMWH once epidural bleeding risk has passed. Salvage: Therapeutic anticoagulation, IVC filter if anticoagulation is contraindicated. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation of a patient with a complex sacral fracture or lumbosacral dislocation is a prolonged, multidisciplinary endeavor that must be carefully tailored to the rigidity of the surgical construct, the patient's neurological status, and the presence of associated polytrauma. A standardized, phased approach ensures the protection of the surgical repair while maximizing functional recovery.
The immediate postoperative phase (0 to 2 weeks) focuses on wound healing, pain control, and the prevention of systemic complications. Patients treated with robust internal fixation, such as triangular osteosynthesis or rigid lumbopelvic constructs, benefit immensely from early mobilization. Depending on the stability achieved, patients may be allowed to sit up and transfer to a chair within the first few days. However, weight-bearing on the affected side (or bilaterally in U-shaped fractures) is strictly prohibited. DVT prophylaxis is critical during this phase, and meticulous wound care is paramount, especially for posterior sacral incisions.
The intermediate phase (2 to 8 weeks) involves progressive physical therapy focused on upper extremity strengthening, core stabilization (within the limits of any applied orthosis), and safe transfer techniques. Radiographic monitoring with AP and lateral plain films is performed at 2, 6, and 12 weeks to assess for hardware failure, loss of reduction, and early signs of callus formation. Weight-bearing status remains highly restricted. Patients managed nonoperatively or with less rigid percutaneous constructs require strict adherence to non-weight-bearing precautions, as premature loading can lead to catastrophic displacement and secondary neurological injury.
The late phase (8 to 12+ weeks) marks the transition to weight-bearing, contingent upon radiographic evidence of bridging trabecular bone across the fracture site or fusion mass. Progression from toe-touch weight-bearing to partial, and eventually full weight-bearing, is advanced over several weeks under the guidance of a physical therapist. Gait training, advanced core strengthening, and the restoration of normal spinopelvic kinematics are the primary goals.
Neurological rehabilitation runs concurrently and is often the most challenging aspect of recovery. The prognosis for motor and sensory recovery in radicular injuries (e.g., L5 or S1) is fair to good following adequate decompression. However, the recovery of autonomic function—specifically bowel, bladder, and sexual function—is notoriously poor when the lower sacral roots (S2-S4) are injured. Patients with neurogenic bladders require early urological consultation, initiation of clean intermittent catheterization (CIC) protocols, and pharmacological management (e.g., anticholinergics). Extensive psychological support and preoperative counseling regarding these life-altering autonomic deficits are essential components of comprehensive patient care.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the surgical management of sacral fractures and lumbosacral dislocations is deeply rooted in several landmark anatomical, biomechanical, and clinical studies that have shaped modern orthopedic trauma protocols.
The foundational work by Denis et al. revolutionized the understanding of sacral fractures by categorizing them into three distinct anatomical zones based on the vertical location of the fracture line. This classification system remains the most highly predictive tool for anticipating neurological injury, establishing that Zone III (central canal) fractures carry an 87% risk of severe neurological deficits, including cauda equina syndrome, thereby guiding the absolute indications for central decompression.
Aihara et al. provided a critical framework for lumbosacral dislocations, a rare but devastating subset of injuries. By reviewing 50 reported cases and categorizing them into five distinct types based on facet and vertebral body involvement, Aihara definitively concluded that conservative treatment is universally ineffective due to the inherent, multiplanar instability of the disrupted lumbosacral junction. This established the modern clinical guideline that all Aihara Type 1-5 injuries mandate open reduction and rigid internal lumbopelvic fixation.
From a biomechanical perspective, the concept of "triangular osteosynthesis" introduced by Schildhauer et al. represents a paradigm shift in the stabilization of highly unstable, vertically sheared sacral fractures and spinopelvic dissociations. Through rigorous cadaveric testing, Schildhauer demonstrated that combining vertical lumbopelvic fixation (pedicle screws to iliac screws) with horizontal transverse iliosacral screws provides significantly greater multiplanar stability and higher load-to-failure rates compared to traditional iliosacral screws alone, allowing for earlier mobilization of critically ill polytrauma patients.
Finally, the advancement of minimally invasive techniques was championed by Nork et al., who published extensive series on the percutaneous stabilization of complex U-shaped sacral fractures. Nork demonstrated that with strict adherence to fluoroscopic protocols (inlet, outlet, and lateral views), percutaneous iliosacral screws could reliably stabilize these fractures in situ. While this technique minimizes soft tissue morbidity and blood loss, clinical guidelines emphasize that it is generally reserved for patients with acceptable spinopelvic alignment and without progressive neurological deficits requiring direct open decompression.
