Mastering Posterior Screw Fixation for Sacral Fractures and Sacroiliac Dislocations
Key Takeaway
Posterior screw fixation is a cornerstone technique for stabilizing sacral fractures and sacroiliac joint disruptions. This procedure demands a profound understanding of upper sacral morphology, specifically the sacral alar slope and the iliac cortical density (ICD). Utilizing precise fluoroscopic imaging—including inlet, outlet, and true lateral views—surgeons can safely navigate the osseous corridor, avoiding critical neurovascular structures such as the L5 nerve root and iliac vessels.
Comprehensive Introduction and Patho-Epidemiology
The posterior pelvic ring serves as the primary weight-bearing axis of the human skeletal system, functioning as the critical biomechanical keystone that transmits immense axial loads from the spine to the lower extremities. Disruptions to this highly complex osteoligamentous architecture—whether manifesting as sacral fractures, sacroiliac (SI) joint dislocations, or complex fracture-dislocations—drastically compromise the structural integrity and mechanical stability of the pelvis. Historically, the management of these severe injuries was fraught with high morbidity, prolonged immobilization, and dismal functional outcomes. The evolution of operative intervention, particularly the advent of posterior screw fixation, has revolutionized the standard of care, offering robust mechanical stability that permits early mobilization and optimizes functional recovery.
Posterior screw fixation, specifically the insertion of iliosacral screws, has unequivocally established itself as the gold standard for stabilizing injuries of the posterior pelvic ring. The conceptual framework and technical execution of this procedure were originally pioneered by Matta and Saucedo through open techniques, which allowed for direct visualization of the fracture or dislocation, meticulous debridement, and anatomic reduction. Subsequently, Routt and colleagues profoundly advanced the field by introducing and refining percutaneous applications. This minimally invasive paradigm shift significantly diminished the substantial soft tissue morbidity, massive blood loss, and high infection rates historically associated with extensive posterior surgical exposures.
However, the percutaneous technique is unforgiving; it demands an exacting, tridimensional comprehension of pelvic osteology, advanced fluoroscopic interpretation skills, and flawless surgical execution. The upper sacrum presents a highly variable morphological landscape, and the osseous corridors available for safe screw placement are notoriously narrow. The proximity of critical neurovascular structures—namely the L5 and S1 nerve roots, the lumbosacral plexus, and the internal iliac vessels—mandates extreme precision. A deviation of mere millimeters can result in catastrophic iatrogenic injury, leading to permanent neurologic deficits or life-threatening hemorrhage.
Epidemiologically, posterior pelvic ring disruptions exhibit a bimodal distribution. In the younger demographic, these injuries are predominantly the result of high-energy trauma, such as motor vehicle collisions, motorcycle accidents, or falls from significant heights. These patients frequently present with polytrauma, necessitating a multidisciplinary approach to manage concomitant hemodynamic instability, traumatic brain injury, and visceral damage. Conversely, an increasingly prevalent cohort involves the elderly population sustaining fragility fractures of the pelvis (FFP) from low-energy mechanisms, such as ground-level falls. The osteoporotic nature of the bone in this demographic introduces unique biomechanical challenges regarding hardware purchase and fixation failure, often requiring specialized surgical strategies such as cement augmentation or supplemental lumbopelvic fixation.
Detailed Surgical Anatomy and Biomechanics
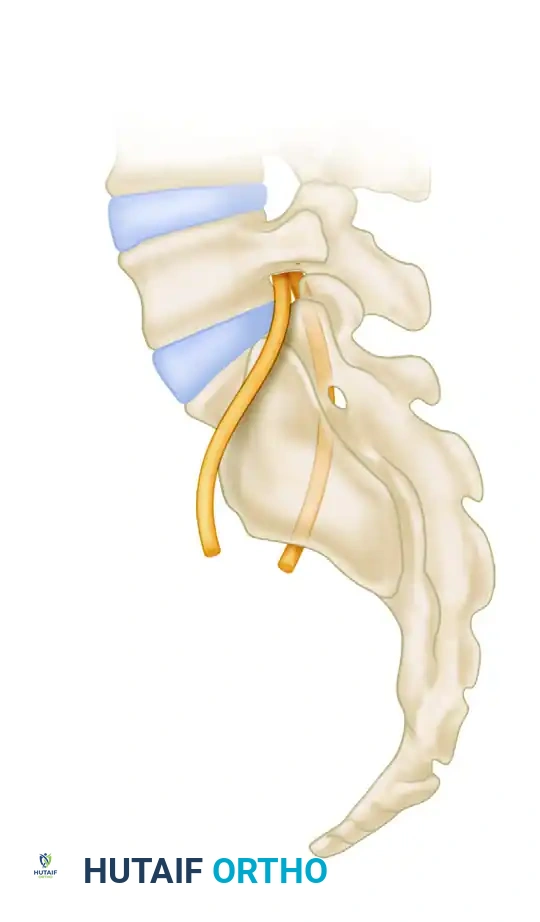
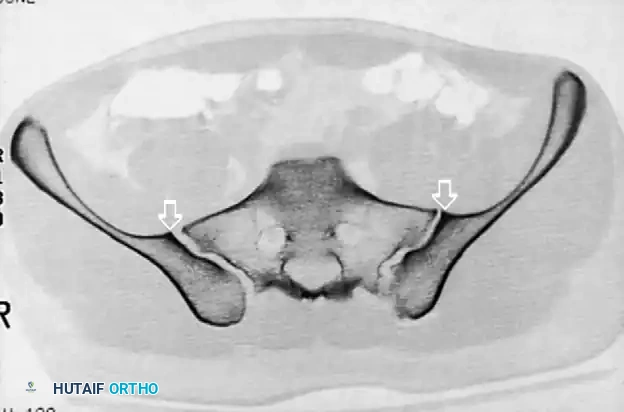
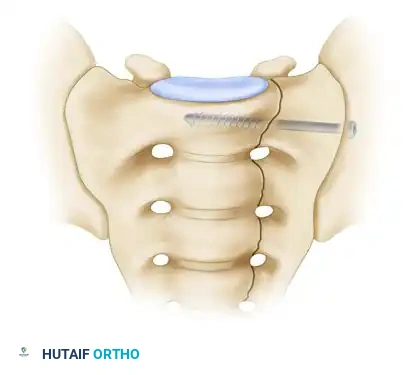
The safe and effective placement of an iliosacral screw is entirely predicated upon a profound understanding of the tridimensional morphology of the upper sacrum. The surgeon must navigate a highly constrained osseous corridor—the "safe zone"—within the S1, and occasionally S2, vertebral bodies. The normal sacral ala is not a simple block of bone; it features a complex, inclined anterosuperior surface known as the sacral alar slope, which extends from proximal-posterior to distal-anterior.
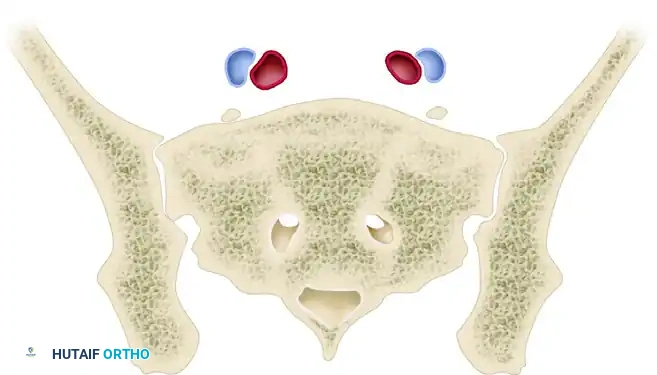
The cortex of the alar slope forms the absolute anterior boundary of the safe zone for the passage of iliosacral screws into the S1 body. Anterior to this slope lie the critical structures of the lumbosacral trunk (specifically the L5 nerve root) and the iliac vessels. Penetration of this anterior cortex during drilling or screw insertion can result in catastrophic hemorrhage or permanent iatrogenic neurologic deficit. The posterior boundary of the safe zone is formed by the anterior cortex of the S1 nerve root foramen and the sacral spinal canal. Therefore, the trajectory of the screw must be perfectly calibrated to pass between the alar slope anteriorly and the neuroforamen posteriorly.
A thorough preoperative evaluation of upper sacral morphological features is absolutely mandatory, as standard anatomy is frequently disrupted by congenital variations. Routt et al. demonstrated that sacral dysplasia occurs in a significant percentage of patients, with some series reporting an incidence of up to 35%. A dysplastic sacrum typically exhibits an atypical, more acute sacral alar slope and a severely constricted osseous corridor. In these cases, the upper sacral segment may be partially lumbarized, or the S1 body may be situated higher relative to the iliac crests. This drastic narrowing of the safe zone often precludes the safe placement of a standard 7.0 mm or 7.3 mm iliosacral screw in the S1 segment, necessitating alternative fixation strategies such as S2 screw placement or posterior tension band plating.

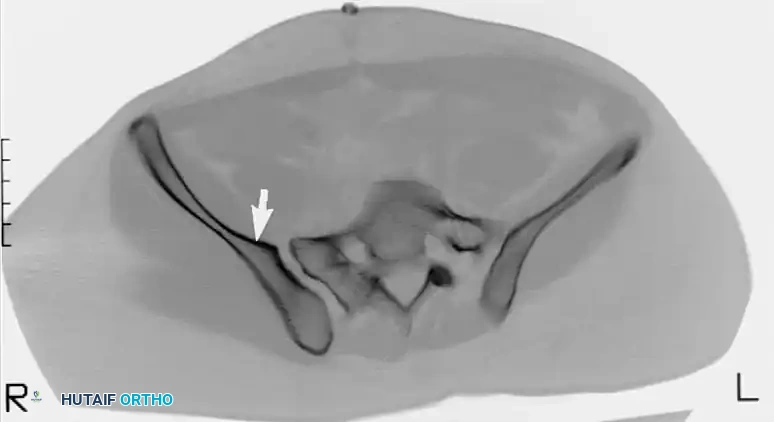
Furthermore, some non-dysplastic sacral alae display an anterior concavity or recession when viewed in the axial plane. A recessed sacral ala creates a highly dangerous anatomical trap for the unwary surgeon. If a standard transverse trajectory is utilized, the drill or screw may inadvertently exit the anterior sacral cortex into the concavity and subsequently re-enter the vertebral body near the midline. This "in-out-in" trajectory directly threatens the L5 nerve root, which courses precisely over this recessed area. Recognition of this morphology on preoperative axial Computed Tomography (CT) is critical to adjusting the starting point and trajectory to remain entirely intraosseous.
Biomechanically, the posterior pelvic ring must withstand immense shear and bending moments. Iliosacral screws provide stability through two distinct mechanical principles depending on the injury pattern. For pure sacroiliac joint dislocations, the screw functions as a lag screw; it is placed perpendicular to the joint surface to generate maximum interfragmentary compression, relying on the friction between the articular surfaces for stability. Conversely, for transforaminal sacral fractures (Denis Zone II), compression can result in iatrogenic crushing of the sacral nerve roots within the foramen. In these instances, a fully threaded screw is utilized as a position screw, placed more transversely to span the fracture without compressing it, often aiming deep into the contralateral sacral ala or S1 body to maximize thread purchase in the densest available bone.
Exhaustive Indications and Contraindications
The decision-making process regarding the implementation of posterior screw fixation requires a meticulous analysis of the patient's physiological status, the specific fracture morphology, and the overall stability of the pelvic ring. The primary indication for iliosacral screw fixation is the presence of an unstable posterior pelvic ring injury that mandates mechanical stabilization to permit mobilization and prevent chronic deformity or pain.
Specific indications include completely unstable vertical shear (VS) injuries, severe anteroposterior compression (APC type II and III) injuries with complete disruption of the anterior and posterior sacroiliac ligaments, and lateral compression (LC type II and III) injuries exhibiting rotational or vertical instability. Furthermore, iliosacral screws are indicated for the stabilization of Denis Zone I (alar) and Zone II (transforaminal) sacral fractures, provided that the fracture pattern allows for adequate screw purchase without compromising neural elements. In the context of polytrauma, early percutaneous fixation is highly indicated as it provides rapid skeletal stability, which is a critical component of damage control orthopedics, aiding in pain control, facilitating nursing care, and reducing the systemic inflammatory response.
Contraindications, while fewer, are absolute and must be rigorously respected to prevent catastrophic outcomes. Hemodynamic instability unresuscitable by massive transfusion protocols precludes definitive fixation; these patients require immediate pelvic packing, angioembolization, or the application of a temporary pelvic binder or external fixator. Anatomical contraindications are primarily dictated by the morphology of the sacrum. Severe sacral dysplasia that obliterates the S1 and S2 safe zones is an absolute contraindication to percutaneous iliosacral screw placement.
Additionally, the presence of significant comminution at the intended screw entry site on the outer iliac table, or a fracture pattern that cannot be adequately reduced closed, contraindicates the percutaneous approach, necessitating an open reduction or alternative fixation methods. Active infection or severe soft tissue compromise (e.g., Morel-Lavallée lesions) overlying the intended surgical approach paths also serves as a critical contraindication, requiring soft tissue management prior to definitive internal fixation.
Table of Indications and Contraindications
| Category | Indications for Posterior Screw Fixation | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Injury Pattern | APC II/III, LC II/III, Vertical Shear (VS) injuries | Severe sacral dysplasia obliterating safe zones | Highly comminuted Denis Zone III (central) sacral fractures |
| Fracture Type | Sacroiliac (SI) joint fracture-dislocations | Unreducible posterior ring injuries (for percutaneous) | Osteoporotic fragility fractures (requires augmentation) |
| Sacral Anatomy | Denis Zone I (Alar) and Zone II (Transforaminal) fractures | Transitional vertebrae preventing safe trajectory | Recessed sacral ala (requires highly modified trajectory) |
| Patient Status | Hemodynamically stable polytrauma patients | Hemodynamic instability (requires damage control) | Severe obesity obscuring fluoroscopic visualization |
| Soft Tissue | Intact posterior soft tissue envelope | Active local infection or open contaminated wounds | Overlying Morel-Lavallée lesion (high infection risk) |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of safe and successful posterior pelvic ring fixation. Standard anteroposterior (AP) pelvic radiographs, while useful for initial trauma screening, are entirely insufficient for the definitive planning of iliosacral screw trajectories. A complete radiographic series, encompassing AP, inlet, and outlet views, must be supplemented by fine-cut Computed Tomography (CT) with axial, coronal, and sagittal reformats.
The sacral alar slope, a critical determinant of the anterior safe zone boundary, can be estimated on a true lateral fluoroscopic view of the sacrum by identifying the Iliac Cortical Density (ICD). The ICD demarcates the anterior cortical thickening of the iliac portion of the sacroiliac joint. In the vast majority (approximately 94%) of non-dysplastic upper sacral segments, the ICD coincides perfectly with the alar slope, making it an invaluable radiographic landmark for determining the anterior border of the safe zone during surgery.

Preoperative CT analysis is non-negotiable. The surgeon must utilize the axial and coronal reformats to measure the exact dimensions of the S1 and S2 osseous corridors. This templating determines the maximum safe screw diameter and length. Furthermore, the CT scan is essential to identify sacral dysplasia, transitional lumbosacral vertebrae, and the presence of a recessed sacral ala. If the safe zone measures less than 7.5 mm in any dimension, the placement of a standard 7.0 mm or 7.3 mm screw is fraught with peril, and the surgeon must plan for smaller diameter screws, targeting the S2 corridor, or utilizing an entirely different fixation construct.
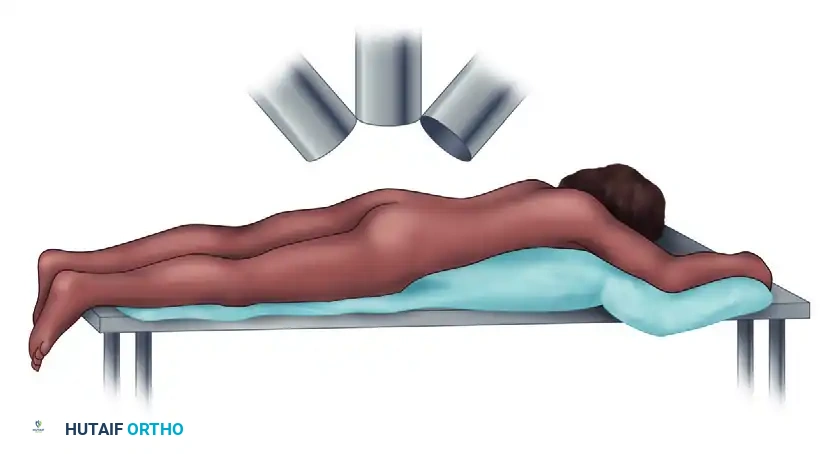
Patient positioning and operating room setup dictate the flow and safety of the procedure. Proper positioning is the foundation of successful posterior pelvic fixation. The procedure can be performed with the patient supine or prone, depending on surgeon preference, associated injuries (e.g., anterior ring fractures requiring simultaneous fixation), and the planned approach (open vs. percutaneous). For the classic Matta and Saucedo open technique, or when purely posterior percutaneous fixation is planned, the prone position is highly advantageous.
The patient is positioned prone on a completely radiolucent operating table, such as a Jackson table or a flat radiolucent board. It is critical to ensure the abdomen is free from compression; this reduces intra-abdominal venous pressure, thereby minimizing epidural and operative site bleeding. All bony prominences must be meticulously padded. The fluoroscopic setup is equally critical. The image intensifier (C-arm) must be positioned to freely rotate and obtain three critical views—Inlet (25-40 degrees caudad), Outlet (40 degrees cephalad), and True Lateral—without moving the patient or the table.

Step-by-Step Surgical Approach and Fixation Technique
The Open Posterior Approach (Matta and Saucedo Technique)
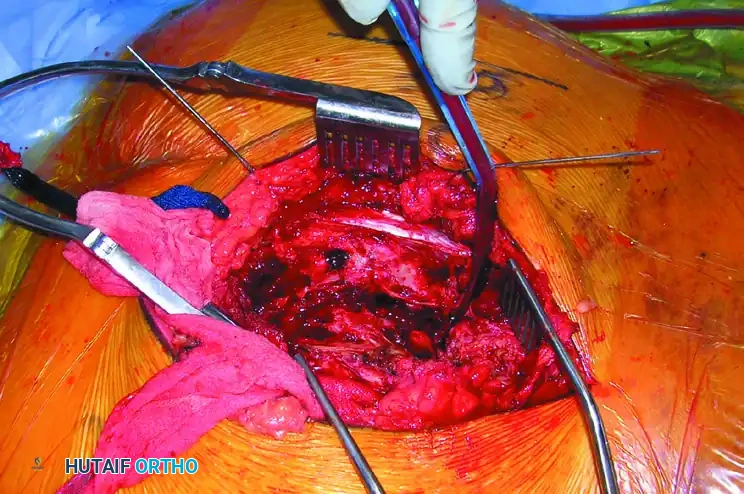
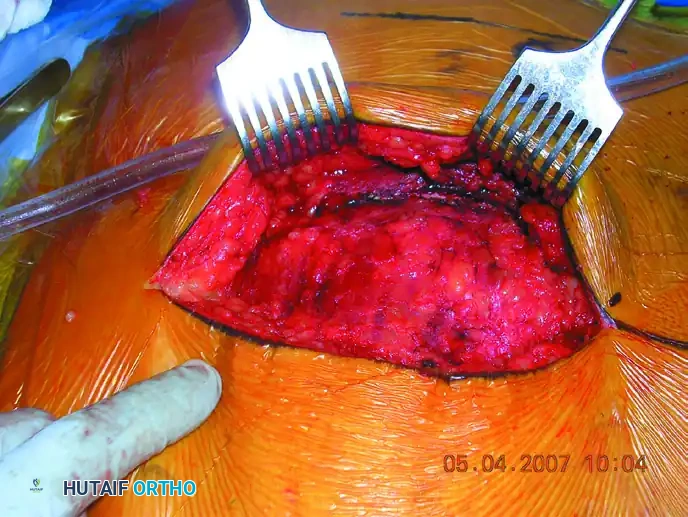
The open approach is primarily indicated when closed reduction of a sacroiliac dislocation or sacral fracture is unachievable, when there is a highly comminuted fracture requiring direct manipulation, or when direct decompression of the sacral nerve roots is clinically mandated. The procedure begins with a standard posterior vertical incision, located approximately 2 cm lateral to the posterior superior iliac spine (PSIS), extending distally. The subcutaneous tissues are incised down to the robust gluteal fascia.
The posterior portion of the gluteal musculature is sharply reflected from the posterior iliac wing. To achieve adequate exposure of the posterior sacroiliac ligaments and the sacrum itself, the origin of the gluteus maximus must be carefully detached from the sacrum. This deep exposure allows the surgeon to visualize the posterior sacral lamina and access the greater sciatic notch.
Exposing the greater sciatic notch is a critical step; it permits the surgeon to digitally palpate the anterior aspect of the SI joint, providing tactile feedback to evaluate the accuracy of the reduction. For sacral fractures, the multifidus muscles are elevated to expose the fracture of the posterior sacral lamina. Reduction is typically achieved by placing pointed Weber or Jungbluth reduction forceps from the sacrum (via a carefully placed drill hole in the posterior iliac spine) to the iliac wing. The joint is compressed while simultaneously palpating through the greater sciatic notch and directly observing the posterior joint line to confirm an anatomic reduction.
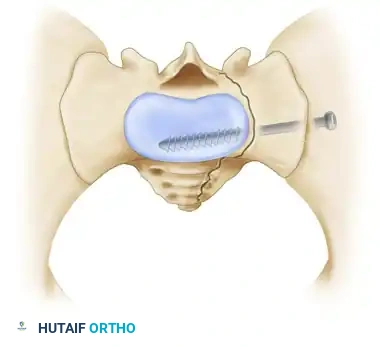
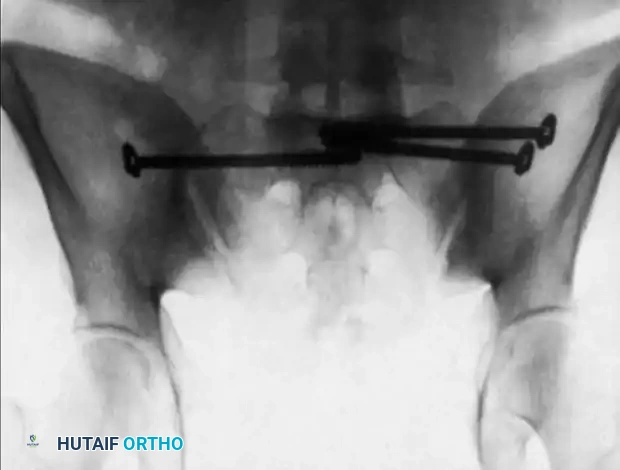
Once reduction is achieved and provisionally held, screw insertion commences. Under continuous image intensifier control, a guide wire is inserted perpendicular to the iliac wing, directed across the sacroiliac joint into the sacral ala, targeting the dense bone in the center of the S1 vertebral body.
The surgeon must carefully target the drill bit and subsequent screws by alternating between AP, inlet, outlet, and lateral fluoroscopic projections. Typically, one or two fully threaded or partially threaded 7.0 mm or 7.3 mm cannulated screws are inserted into the S1 vertebral body from the lateral surface of the iliac wing. If comminution or instability persists despite screw fixation, a 3.5-mm or 4.5-mm reconstruction plate may be applied across the posterior sacrum from ilium to ilium as a tension band.

Percutaneous Iliosacral Screw Fixation
Percutaneous fixation relies entirely on flawless fluoroscopic imaging and is predicated on achieving an anatomic or near-anatomic closed reduction prior to any drilling. Malreduction distorts radiographic landmarks, making the superimposition of the greater sciatic notches and both ICDs on the true lateral image impossible, thereby rendering percutaneous targeting unsafe. Reduction is achieved via skeletal traction, pelvic binders, or percutaneous joy-sticks (Schanz pins placed in the iliac crests).
The fluoroscopic targeting sequence is rigid. First, a perfect true lateral view of the sacrum is obtained. The greater sciatic notches must be perfectly superimposed. The ICD is identified, and the guide wire starting point is mapped on the lateral ilium. The guide wire is advanced through the ilium and into the sacral ala.
The C-arm is then switched to the Inlet View. In this projection, the surgeon confirms that the wire is posterior to the anterior sacral cortex (alar slope) and anterior to the spinal canal.

Following inlet confirmation, the C-arm is switched to the Outlet View. This projection is critical to confirm that the wire is superior to the S1 neuroforamen and inferior to the S1 superior endplate. Only when the guide wire is confirmed to be entirely intraosseous in all three planes (Lateral, Inlet, Outlet) is the cannulated drill bit advanced over the wire.
The depth is measured, the near cortex is tapped if the bone is particularly dense, and the appropriate length cannulated screw is inserted. The use of heavy washers is highly recommended, especially in osteoporotic bone, to prevent the screw head from sinking through the thin outer iliac cortex, which would result in a catastrophic loss of compression and fixation failure.
Complications, Incidence Rates, and Salvage Management
Despite advances in fluoroscopic imaging and surgical technique, posterior screw fixation of the pelvic ring carries a significant risk profile. The most devastating complication is iatrogenic nerve injury, most commonly affecting the L5 or S1 nerve roots. This typically occurs due to cortical breach during drilling or screw insertion. The incidence of neurologic injury in the literature ranges from 2% to 8%, heavily dependent on the surgeon's experience and the complexity of the sacral morphology.
A specific and highly dangerous mechanism of L5 nerve root injury is the "In-Out-In" phenomenon. If the surgeon fails to recognize a recessed sacral ala on preoperative CT, or relies solely on inlet and outlet views without confirming the trajectory on a true lateral view referencing the ICD, the screw may exit the anterior cortex of the sacrum, traverse the concavity of the ala, and re-enter the vertebral body. This extraosseous trajectory directly impales, stretches, or compresses the L5 nerve root as it courses over the sacral ala.

Vascular injury, while less common than neurologic injury, is potentially lethal. Penetration of the anterior sacral cortex can lacerate the internal iliac artery or vein, or the superior gluteal vessels. Fixation failure is another significant complication, occurring in 5% to 15% of cases. It is most frequently observed in cases of severe vertical shear instability where a single S1 screw is utilized, in highly comminuted transforaminal fractures, or in severely osteoporotic bone.
Salvage management for fixation failure or severe comminution often requires escalation of the fixation construct. If an iliosacral screw fails, the surgeon may need to utilize bi-segmental fixation (placing screws in both the S1 and S2 corridors). In cases of profound spinopelvic dissociation (e.g., U-type sacral fractures) or when local sacral bone quality is abysmal, lumbopelvic fixation (pedicle screws in L4/L5 connected to iliac screws) provides the ultimate biomechanical salvage, bypassing the fractured sacrum entirely to transfer loads directly from the lumbar spine to the intact ilium.
Table of Complications and Management Strategies
| Complication | Estimated Incidence | Primary Etiology | Prevention and Salvage Management |
|---|---|---|---|
| L5 Nerve Root Injury | 2% - 5% | "In-Out-In" trajectory; anterior cortical breach | Pre-op CT analysis for recessed ala; strict adherence to lateral ICD imaging. Salvage: Immediate screw removal. |
| S1 Nerve Root Injury | 1% - 4% | Inferior trajectory breaching the S1 neuroforamen | Strict Outlet view confirmation before drilling. Salvage: Immediate hardware revision; possible foraminotomy. |
| Vascular Hemorrhage | < 1% | Anterior cortical breach lacerating iliac vessels | Avoid over-penetration of the anterior alar slope. Salvage: Emergent laparotomy/packing or angioembolization. |
| Fixation Failure / Loosening | 5% - 15% | Osteoporosis; inadequate screw length; vertical shear | Use washers; utilize fully threaded screws for positioning; bi-segmental S1/S2 screws. Salvage: Lumbopelvic fixation. |
| Surgical Site Infection | 1% (Perc) - 10% (Open) | Extensive soft tissue stripping; Morel-Lavallée | Prefer percutaneous techniques; meticulous debridement of degloving injuries. Salvage: I&D, targeted IV antibiotics. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following posterior pelvic ring fixation is a delicate balance between protecting the mechanical integrity of the surgical construct and preventing the myriad complications associated with prolonged recumbency. The protocol must be individualized, heavily influenced by the fracture pattern (e.g., rotationally unstable vs. vertically unstable), bone quality, and the presence of concomitant appendicular or axial injuries.
In the immediate postoperative phase (0 to 2 weeks), the primary goals are pain control, mobilization out of bed, and the prevention of venous thromboembolism (VTE). Pelvic trauma carries an exceptionally high risk of deep vein thrombosis and pulmonary embolism. Chemical prophylaxis, typically with Low Molecular Weight Heparin (LMWH), should be initiated as soon as it is surgically safe—often within 24 hours postoperatively, provided there is no ongoing hemorrhage or epidural hematoma risk. Weight-bearing is strictly limited. For purely rotationally unstable injuries fixed robustly, toe-touch weight-bearing (TTWB) on the affected side may be permitted. However, for vertically unstable injuries or in osteoporotic patients, strict non-weight-bearing (NWB) on the affected side is mandated.
During the intermediate phase (2 to 6 weeks), physical therapy focuses on active and active-assisted range of motion of the bilateral hips, knees, and ankles to prevent contractures. Core strengthening and upper extremity conditioning are critical to assist with walker or crutch mobilization. Radiographic follow-up with AP, inlet, and outlet views is performed at 2 weeks and 6 weeks to meticulously monitor for any insidious loss of reduction, hardware migration, or haloing around the screws indicative of loosening.
In the late phase (6 to 12 weeks and beyond), clinical and radiographic evidence of fracture consolidation dictates the progression of weight-bearing. Once bridging callus is visualized or the SI joint appears stable, patients are gradually transitioned from TTWB to partial weight-bearing, and eventually to full weight-bearing. Gait training, proprioceptive exercises, and abductor strengthening become the focal points of therapy. CT scanning may be utilized postoperatively at any phase if there is any clinical suspicion of neurologic irritation, delayed union, or hardware failure that is not clearly delineated on plain radiographs.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management of posterior pelvic ring injuries is built upon a foundation of landmark biomechanical and clinical research. The transition from prolonged bed rest to operative stabilization was spearheaded by the early works of Tile and Pennal, who classified pelvic ring injuries based on the vector of force and resulting instability, establishing the rationale for mechanical fixation. The Young-Burgess classification further refined this by correlating the mechanism of injury (APC, LC, VS) with associated resuscitation needs and fixation strategies.
The surgical techniques discussed in this chapter are deeply rooted in the pioneering efforts of Matta and Saucedo, whose 1989 publication detailed the open reduction and internal fixation of the pelvic ring, proving that anatomic reduction significantly correlated with improved long-term functional outcomes. However, the paradigm shifted dramatically with Routt, Simonian, and Mills in the mid-1990s. Their exhaustive anatomical studies defined the "safe zones" of the upper sacrum and established the rigid fluoroscopic protocols—specifically the utilization of the inlet, outlet, and true lateral views with the ICD—that made percutaneous iliosacral screw fixation reproducible and safe.
Current clinical guidelines, supported by the Orthopaedic Trauma Association (OTA) and AO Foundation, strongly advocate for the percutaneous approach whenever
