Radiographic Evaluation of Pelvic Fractures | Orthopaedic Guide

Key Takeaway
The radiographic evaluation of pelvic fractures requires a systematic approach to identify life-threatening instability. Standard protocols mandate an anteroposterior pelvis radiograph, supplemented by 40-degree caudal inlet and 40-degree cephalad outlet views. These projections accurately delineate rotational deformity, anteroposterior translation, and vertical displacement. Advanced assessment includes dynamic stress testing and computed tomography to guide emergent damage control and definitive surgical fixation in the polytraumatized patient.
Comprehensive Introduction and Patho-Epidemiology
Pelvic ring disruptions represent some of the most mechanically and physiologically challenging injuries encountered in orthopaedic trauma surgery. These complex fractures are typically the result of high-energy mechanisms, including motor vehicle collisions, motorcycle crashes, pedestrian-versus-auto incidents, crush injuries, and falls from significant heights. The initial assessment and management of these polytraumatized patients demand a highly coordinated, multidisciplinary approach. The orthopaedic surgeon plays an indispensable, central role in this acute phase, tasked with rapidly identifying mechanical instability, executing damage control orthopaedics, and mitigating catastrophic, life-threatening retroperitoneal hemorrhage.
The epidemiological profile of pelvic ring injuries traditionally demonstrates a bimodal distribution. The first peak occurs in young, healthy individuals (predominantly males in their second to fourth decades of life) who sustain severe, high-velocity trauma. These patients often present with concomitant injuries, including traumatic brain injuries, blunt thoracic trauma, and solid organ lacerations, which complicate the clinical picture and elevate the mortality rate. The second peak is increasingly observed in the geriatric population, where low-energy mechanisms, such as a simple fall from a standing height, can result in devastating fragility fractures of the pelvic ring due to underlying osteopenia or osteoporosis. As the global population ages, the incidence of these lateral compression-type fragility fractures is rising exponentially, presenting unique challenges regarding fixation strategies in poor-quality bone.
The absolute foundation of initial assessment in the trauma bay relies on a rigorous, standardized radiographic evaluation. Accurate, immediate interpretation of pelvic radiographs dictates the resuscitation pathway, determining whether the patient requires immediate pelvic binding, pre-peritoneal pelvic packing, angioembolization, or urgent application of an external fixator. The Advanced Trauma Life Support (ATLS) protocol mandates an anteroposterior (AP) radiograph of the pelvis as a primary screening adjunct during the primary survey of any blunt polytrauma patient. However, the AP view alone is often insufficient for a comprehensive understanding of complex ring disruptions.
A profound understanding of the patho-anatomy revealed on these initial radiographs is essential for formulating a definitive surgical reconstruction plan. The surgeon must rapidly synthesize radiographic data to classify the injury pattern, predict the associated ligamentous damage, and anticipate the vectors of instability. Failure to recognize subtle radiographic signs of instability can lead to catastrophic intraoperative complications, progressive deformity, chronic debilitating pain, and severe functional impairment. Therefore, mastery of pelvic radiographic interpretation is a non-negotiable skill for the practicing orthopaedic trauma surgeon.
Detailed Surgical Anatomy and Biomechanics
The pelvic ring is a complex, basin-shaped osteoligamentous structure that serves as the critical mechanical linkage between the axial skeleton and the appendicular skeleton of the lower extremities. Anatomically, it is composed of the sacrum posteriorly and the two innominate bones (ilium, ischium, and pubis) laterally and anteriorly. These osseous structures are united by a robust network of ligaments that confer exceptional stability to the ring. The biomechanical integrity of the pelvis relies heavily on the "posterior tension band," a dense complex of ligaments that resists the immense shear and rotational forces generated during upright posture and ambulation.
The posterior ligamentous complex is the primary stabilizer of the pelvic ring. It consists of the anterior sacroiliac ligaments, the interosseous sacroiliac ligaments (the strongest ligaments in the human body), and the posterior sacroiliac ligaments. Additionally, the sacrotuberous and sacrospinous ligaments act to resist rotational forces and vertical shear stresses, anchoring the sacrum to the ischium. Disruption of this posterior complex is the hallmark of vertical instability and necessitates robust surgical fixation. Anteriorly, the symphysis pubis is stabilized by the superior and arcuate pubic ligaments, which primarily resist external rotation and tension forces. While the anterior structures contribute to approximately 40% of the ring's stiffness, the posterior structures provide the remaining 60% and are paramount for weight-bearing stability.
Biomechanically, the pelvis functions as an arch, transferring the weight of the trunk from the sacrum across the sacroiliac joints, through the ilia, and down into the acetabula and bilateral femurs. When the patient is seated, the force vector shifts, transferring weight from the sacrum through the ilia to the ischial tuberosities. Unstable pelvic fractures disrupt this arch, leading to pathological motion under physiologic loads. The specific radiographic projections utilized in clinical practice are meticulously designed to profile these distinct anatomical structures and their biomechanical relationships.
The AP view provides a global assessment of the pelvic arch, allowing for the evaluation of the symphysis pubis, the iliopectineal and ilioischial lines, the radiographic U (teardrop), and the sacroiliac joints. The 40-degree caudal inlet view provides an axial perspective, essential for visualizing the pelvic brim and identifying rotational deformity or anteroposterior translation. The 40-degree cephalad outlet view provides a true orthogonal projection of the sacrum and anterior ring, critical for assessing vertical displacement and transforaminal sacral fractures. A deep, three-dimensional spatial awareness of these radiographic landmarks is required to mentally reconstruct the injury and plan safe, effective screw trajectories during surgical intervention.
Exhaustive Indications and Contraindications
The decision-making process regarding imaging modalities and acute interventions in pelvic trauma must be swift and precise. While the AP pelvis radiograph is universally indicated for all blunt polytrauma patients according to ATLS protocols, the indications for supplementary imaging and dynamic testing require careful clinical judgment. High-resolution multi-detector Computed Tomography (CT) with multiplanar reconstructions has largely supplanted dynamic stress testing in modern trauma centers, providing exquisite osseous detail without the risks associated with manual manipulation of an unstable pelvis.
Dynamic stress testing, specifically the push-pull maneuver under fluoroscopic guidance, remains a valuable tool in specific, equivocal scenarios. It is primarily indicated when differentiating between an Anteroposterior Compression Type I (AP-I) and Type II (AP-II) injury, or when assessing the stability of a seemingly isolated pubic ramus fracture in a patient with intractable pain. By applying controlled, alternating cephalad and caudal forces to the lower extremities, the surgeon can unmask occult vertical or rotational instability. If more than 1 cm of cephalad displacement is observed, the posterior tension band is completely disrupted, confirming vertical instability and altering the surgical plan to include robust posterior fixation.
However, the contraindications to dynamic stress testing are strict and must be respected to prevent iatrogenic catastrophe. The push-pull test is absolutely contraindicated in hemodynamically unstable patients, as manual manipulation can disrupt fragile retroperitoneal hematomas and precipitate lethal hemorrhage. Furthermore, it is strictly contraindicated in the presence of Zone II (transforaminal) or Zone III (central) sacral fractures. Dynamic manipulation of these fracture patterns carries an unacceptably high risk of shearing the sacral nerve roots, leading to irreversible bowel, bladder, and sexual dysfunction.
Table: Indications and Contraindications for Pelvic Imaging and Acute Interventions
| Modality / Intervention | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| AP Pelvis Radiograph | All blunt polytrauma; suspected pelvic injury; ATLS primary survey. | None in the acute trauma setting. | Pregnancy (weigh risk vs. benefit). |
| Inlet / Outlet Radiographs | Further characterization of ring disruption; intraoperative assessment of reduction and hardware placement. | None. | Hemodynamic instability delaying transfer to OR/CT. |
| CT Pelvis (with IV contrast) | Detailed preoperative planning; assessment of posterior ring/sacrum; identification of arterial blush. | None. | Severe contrast allergy; profound renal failure (weigh life-saving benefit). |
| Dynamic Stress Testing (Push-Pull) | Equivocal static radiographs; differentiating AP-I vs AP-II; assessing occult instability. | Hemodynamic instability; Zone II/III sacral fractures; active hemorrhage. | Severe ipsilateral lower extremity trauma (femur/tibia fractures). |
| Pelvic Binder / Sheet | Suspected "open book" or unstable pelvic fracture with hemodynamic instability. | None (life-saving). | Lateral compression injuries with severe internal rotation (may exacerbate deformity). |
| Pelvic C-Clamp | Hemodynamically unstable posterior ring disruption (Vertical Shear, AP-III). | Comminuted ilium fractures; transforaminal sacral fractures. | Pediatric patients (due to size constraints and bone quality). |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for pelvic ring reconstructions is a meticulous process that begins with the integration of radiographic and CT data to classify the injury accurately. The Young-Burgess classification system, which categorizes injuries based on the vector of the deforming force (Anteroposterior Compression, Lateral Compression, Vertical Shear, and Combined Mechanical), is highly predictive of associated resuscitation requirements and mortality. Conversely, the Tile/OTA classification focuses on the morphological stability of the posterior ring, guiding the specific biomechanical requirements of the surgical fixation.
Templating is performed using digital software on the preoperative CT scans and standardized radiographs. For anterior ring disruptions, the surgeon must measure the symphyseal diastasis and template the appropriate multi-hole symphyseal plate, ensuring adequate screw purchase in the dense bone of the pubic bodies. For posterior ring injuries, templating is critical for determining the safe corridors for percutaneous iliosacral screws. The surgeon utilizes axial, coronal, and sagittal CT reconstructions to measure the dimensions of the S1 and S2 vertebral bodies, assessing for sacral dysmorphism. Dysmorphic sacra present with acute alar slopes, non-recessed anterior sacral cortices, and narrowed osseous corridors, necessitating modified screw trajectories to avoid the L5 nerve root anteriorly and the sacral neuroforamina inferiorly.
Patient positioning is dictated by the specific injury pattern and the planned surgical approach. For isolated anterior ring fixation (e.g., AP-II injuries), the patient is positioned supine on a radiolucent Jackson table. A bump may be placed under the lumbosacral junction to accentuate the pelvic inlet. The lower extremities must be draped free to allow for intraoperative manipulation and the application of traction. For combined anterior and posterior percutaneous fixation, the supine position is also preferred, allowing simultaneous access to the symphysis pubis and the posterior iliosacral corridors under fluoroscopic guidance.
In cases requiring direct open reduction of the posterior ring (e.g., severe sacral comminution, large crescent fractures, or delayed presentations), the patient may be positioned prone. Prone positioning provides excellent exposure for posterior tension band plating or direct visualization of the sacral neuroforamina for decompression. However, prone positioning complicates airway management and limits access to the anterior ring, often necessitating a staged procedure or intraoperative repositioning, which significantly increases surgical time and physiological stress on the polytraumatized patient.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of pelvic ring disruptions is heavily dependent on the specific injury pattern identified during the radiographic evaluation. The following case studies illustrate the step-by-step surgical approaches and fixation techniques for distinct Young-Burgess classifications.
Case 1: Young-Burgess Anteroposterior Compression Type II (AP II)
An AP II injury is characterized by an "open book" pelvis resulting from a direct anterior-to-posterior force. This causes symphyseal diastasis (>2.5 cm) and disruption of the anterior sacroiliac, sacrotuberous, and sacrospinous ligaments. The posterior sacroiliac ligaments remain intact, preventing vertical translation but allowing rotational instability.


Surgical Technique: The patient is positioned supine. A Pfannenstiel approach is utilized, making a transverse incision 2 fingerbreadths superior to the symphysis pubis. The rectus abdominis fascia is incised longitudinally in the midline, and the rectus muscles are mobilized laterally. The retropubic space (Space of Retzius) is bluntly dissected. A Jungbluth pelvic reduction forceps is applied using 4.5mm cortical screws placed into the superior pubic rami on either side of the diastasis. The forceps are slowly compressed to anatomically reduce the symphysis. A multi-hole (typically 4 to 6 holes) symphyseal plate is contoured to the anterior superior aspect of the pubic ring. Alternating fully threaded 3.5mm or 4.5mm cortical screws are placed to stabilize the diastasis.


Postoperative AP, inlet, and outlet views confirm anatomic reduction of the anterior ring and restoration of pelvic volume, ensuring the hardware is appropriately positioned without intra-articular penetration.
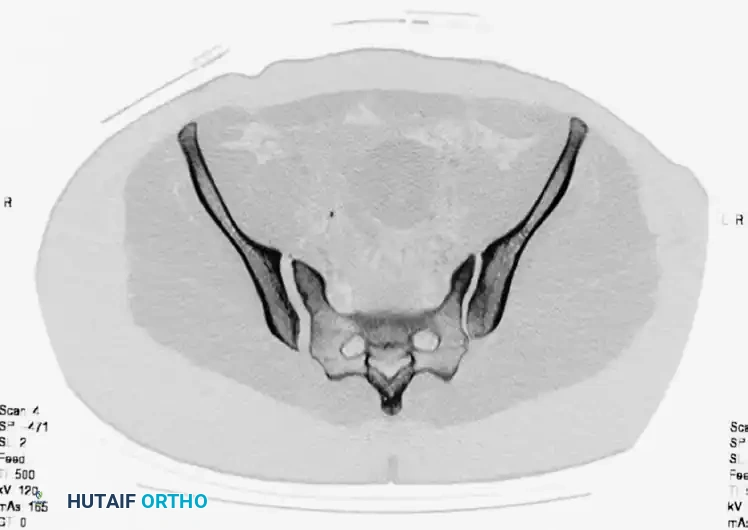
Case 2: Young-Burgess Lateral Compression Type II (LC II)
An LC II injury results from a lateral force vector, characterized by anterior transverse pubic rami fractures combined with a posterior iliac wing fracture (often a "crescent fracture" extending into the SI joint). The hemipelvis is internally rotated.



A preoperative CT scan is mandatory to assess the size of the crescent fragment and the integrity of the SI joint articulation, which dictates the surgical approach.

Surgical Technique: For a large crescent fragment, a posterior approach to the ilium is utilized with the patient in the lateral decubitus or prone position. An incision is made along the posterior iliac crest. The gluteal musculature is elevated subperiosteally to expose the fracture site. The internal rotation deformity is corrected using a Schanz pin placed in the intact ilium as a joystick. The crescent fracture is anatomically reduced and stabilized using a 3.5-mm reconstruction plate applied to the outer table of the ilium. Lag screws are placed perpendicularly across the fracture line between the inner and outer iliac cortical tables to provide absolute stability.

Postoperative films demonstrate restoration of the posterior pelvic ring contour and appropriate hardware placement.
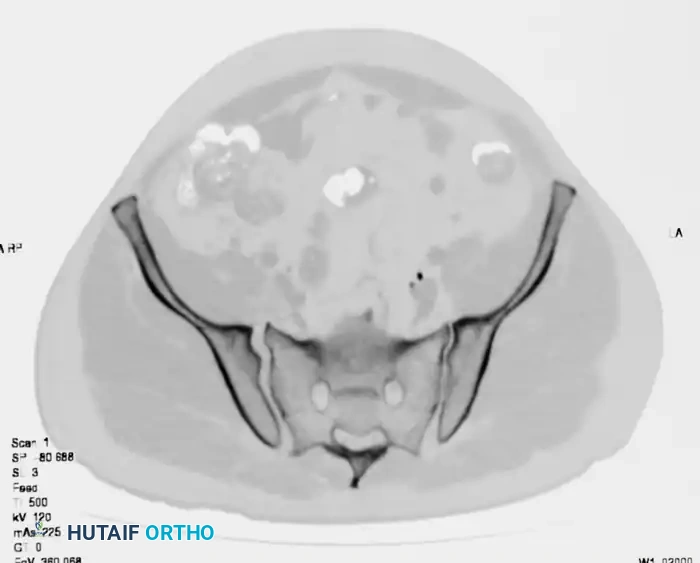
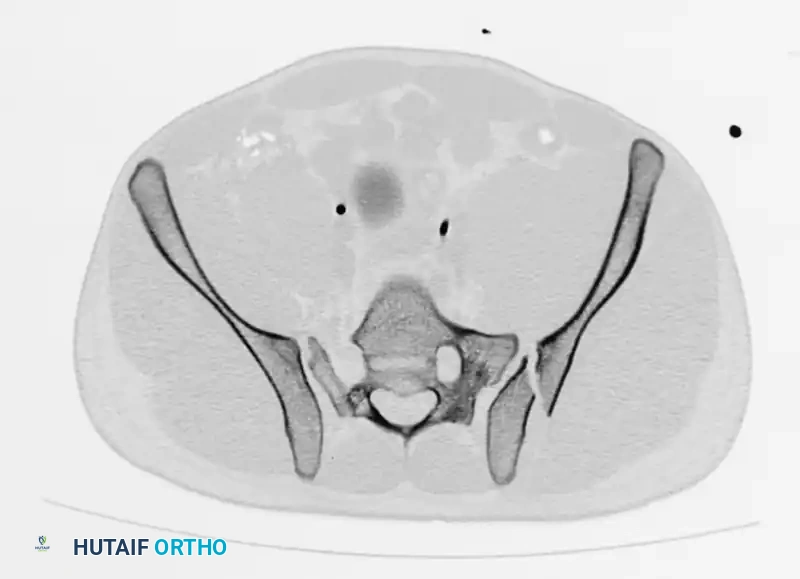
Case 3: Young-Burgess Anteroposterior Compression Type III (AP III)
An AP III injury is a completely unstable pelvic ring disruption involving complete disruption of the symphysis pubis and both the anterior and posterior sacroiliac ligamentous complexes. The hemipelvis is both rotationally and vertically unstable.


Axial CT imaging confirms the complete dissociation of the sacroiliac articulation, highlighting the profound instability of the posterior tension band.

Surgical Technique: AP III injuries require robust anterior and posterior fixation. The patient is positioned supine. Anteriorly, a symphyseal plate is applied via a Pfannenstiel approach as described above. Posteriorly, percutaneous iliosacral screws are utilized. Under strict fluoroscopic guidance (utilizing precise AP, Inlet, and Outlet views), a guide pin is advanced from the lateral aspect of the ilium, across the SI joint, and into the S1 vertebral body. The trajectory is confirmed on all three views to ensure it remains within the osseous corridor, avoiding the sacral canal and neuroforamina. A 7.0mm or 7.3mm cannulated, partially threaded screw is then advanced over the wire to compress the SI joint. In cases of severe vertical instability, a second screw in S1 or an additional screw in S2 may be required.
Complications, Incidence Rates, and Salvage Management
The surgical management of pelvic ring disruptions carries a high complication profile due to the severity of the initial trauma, the complex regional anatomy, and the demanding nature of the surgical interventions. Recognizing and managing these complications is as critical as the initial fixation. Hemorrhage is the most immediate life-threatening complication, with venous bleeding from the presacral plexus accounting for the vast majority of cases. Arterial bleeding, typically from the superior gluteal or internal pudendal arteries, occurs in up to 15% of severe disruptions and requires urgent angioembolization.
Neurologic injury is a profound complication, often occurring at the time of injury but occasionally resulting from iatrogenic hardware placement. The L5 nerve root, which courses over the sacral ala, is highly susceptible to injury during the placement of percutaneous iliosacral screws if the starting point is too anterior or superior. The S1 and S2 nerve roots are at risk from transforaminal sacral fractures or errant screw trajectories breaching the neuroforamina. Iatrogenic nerve injuries mandate immediate radiographic evaluation (CT scan) and urgent hardware removal or revision if a breach is confirmed.
Infection rates following pelvic surgery vary significantly based on the approach and the presence of open fractures. Anterior approaches (Pfannenstiel) have a relatively low deep infection rate (1-3%), whereas posterior approaches, particularly in the presence of severe soft tissue degloving (Morel-Lavallée lesions), can have infection rates exceeding 10%. Management of deep infections requires aggressive surgical debridement, targeted intravenous antibiotic therapy, and often the retention of hardware until bony union is achieved, provided the fixation remains stable.
Hardware failure, nonunion, and malunion are late complications resulting from inadequate mechanical stabilization or patient non-compliance with weight-bearing restrictions. Loss of reduction is most commonly seen in vertically unstable injuries (Vertical Shear or AP III) where the posterior fixation is insufficient to counteract the massive shear forces of weight-bearing. Salvage management for pelvic nonunion or malunion is incredibly challenging, often requiring extensile exposures, complex osteotomies to correct deformity, and massive structural bone grafting combined with rigid lumbopelvic fixation constructs.
Table: Complications, Incidence, and Management Strategies
| Complication | Estimated Incidence | Primary Management Strategy | Salvage / Secondary Intervention |
|---|---|---|---|
| Venous Hemorrhage | 80-90% of bleeding | Pelvic binder, volume resuscitation, Pre-peritoneal packing. | Massive transfusion protocol, damage control surgery. |
| Arterial Hemorrhage | 10-15% of bleeding | Angiography with selective embolization. | Open surgical ligation (rarely successful). |
| Neurologic Injury (L5/S1) | 10-15% (injury related) | Observation, gabapentinoids, AFO for foot drop. | Immediate hardware removal if iatrogenic breach confirmed on CT. |
| Deep Surgical Infection | 2-10% (varies by approach) | Aggressive I&D, culture-directed IV antibiotics. | Hardware removal (only if unstable or post-union), wound VAC. |
| Venous Thromboembolism | Up to 60% (without prophylaxis) | LMWH, SCDs, early mobilization when feasible. | Therapeutic anticoagulation, IVC filter (if anticoagulation contraindicated). |
| Hardware Failure / Malunion | 5-10% | Strict adherence to NWB protocols post-op. | Complex revision ORIF, osteotomies, lumbopelvic fixation. |
Phased Post-Operative Rehabilitation Protocols
Following definitive surgical stabilization of pelvic ring injuries, a strict, evidence-based postoperative protocol is essential to prevent hardware failure, minimize complications, and ensure optimal functional recovery. The rehabilitation protocol must be highly individualized, taking into account the patient's specific injury pattern, the mechanical robustness of the surgical fixation, and the presence of concomitant polytrauma injuries. Communication between the orthopaedic surgeon and the physical therapy team must be unambiguous regarding weight-bearing restrictions and range-of-motion limitations.
Weight-bearing status is the most critical component of the early rehabilitation phase. For patients with stable fixation of rotationally unstable but vertically stable injuries (e.g., an AP II injury treated with robust anterior symphyseal plating), touch-down weight-bearing (TDWB) or flat-foot weight-bearing (FFWB) on the affected side may be permitted immediately. This allows for early mobilization and transfer training while protecting the anterior hardware from excessive physiologic loads. Conversely, for patients with highly unstable or complex fixation (e.g., AP III or Vertical Shear injuries treated with percutaneous iliosacral screws), strict non-weight-bearing (NWB) or TDWB is absolutely mandated for a minimum of 8 to 12 weeks. Premature weight-bearing in these patients invariably leads to catastrophic failure of the posterior ring fixation and recurrent vertical displacement.
Deep Vein Thrombosis (DVT) prophylaxis is paramount in this patient population. Pelvic trauma patients are at an exceptionally high risk for venous thromboembolism due to endothelial injury, venous stasis from immobility, and the hypercoagulable state induced by severe trauma. Chemical prophylaxis, typically utilizing Low Molecular Weight Heparin (LMWH), should be initiated as soon as operative bleeding is controlled and the patient is cleared by the trauma and neurosurgical teams. This chemical prophylaxis is generally continued for 4 to 6 weeks post-injury. Mechanical prophylaxis, including sequential compression devices (SCDs), should be utilized continuously while the patient remains immobile in bed.
Routine postoperative radiographic surveillance is critical to monitor the maintenance of reduction and the progression of bony healing. Standard AP, inlet, and outlet views should be obtained at standardized intervals: typically at 2 weeks post-op to assess for early loss of reduction or hardware back-out, at 6 weeks post-op to evaluate early callus formation and maintain alignment, and at 12 weeks post-op to confirm clinical and radiographic union prior to advancing the patient to full weight-bearing.
Pitfall: Failure to obtain true orthogonal inlet and outlet views can mask subtle loss of reduction or hardware failure. A poorly angled radiograph can artificially foreshorten the posterior ring, hiding vertical migration of the hemipelvis or back-out of an iliosacral screw. The surgeon must insist on high-quality, perfectly angled projections at every follow-up visit to accurately assess the biomechanical integrity of the healing pelvic ring.
Summary of Landmark Literature and Clinical Guidelines
The modern approach to the radiographic evaluation and surgical management of pelvic ring disruptions is built upon a foundation of landmark orthopaedic literature. A comprehensive understanding of these foundational texts is essential for the academic orthopaedic surgeon. The concepts of the pelvic inlet and outlet radiographic projections were originally detailed by Pennal et al., who revolutionized the spatial understanding of pelvic deformities. Their work established that the AP radiograph alone was insufficient for detecting the rotational and vertical translation components of complex ring injuries, cementing the inlet and outlet views as mandatory components of the pelvic trauma series.
The classification of pelvic ring injuries was fundamentally advanced by the work of Young and Burgess. Their mechanistic classification system correlated the vector of the deforming force (Anteroposterior Compression, Lateral Compression, Vertical Shear) with specific patterns of ligamentous disruption and predictable resuscitation requirements. This system remains the gold standard for acute clinical communication, as it directly links the radiographic appearance of the fracture to the patient's physiological status and risk of massive hemorrhage. Concurrently, the work of Marvin Tile, later adapted by the Orthopaedic Trauma Association (OTA), provided a morphological, stability-based classification system. The Tile/OTA system categorizes injuries into rotationally and vertically stable (Type A), rotationally unstable but vertically stable (Type B), and rotationally and vertically unstable (Type C), directly guiding the biomechanical requirements of surgical fixation.
Clinical guidelines promulgated by the Orthopaedic Trauma Association and the American College of Surgeons Committee on Trauma emphasize the necessity of rapid, standardized radiographic evaluation in the trauma bay. Current guidelines strongly advocate for the early application of pelvic binders in hemodynamically unstable patients with suspected open-book or vertically unstable fracture patterns, guided by the initial AP radiograph. Furthermore, the literature increasingly supports the use of high-resolution CT scanning with 3D reconstructions as the definitive modality for preoperative templating, particularly for the safe placement of percutaneous posterior ring fixation.
Long-term outcome studies, notably those by Matta and others, have consistently demonstrated that anatomical reduction of the pelvic ring correlates directly with improved functional outcomes and decreased rates of chronic pain. These studies underscore the critical importance of meticulous radiographic evaluation, precise surgical execution, and rigorous postoperative surveillance. As surgical techniques and imaging modalities continue to evolve, the foundational principles established by this landmark literature remain the guiding light for achieving optimal outcomes in the management of devastating pelvic ring disruptions.
