High-Energy Pelvic Ring Injury: A Comprehensive Case Study of APC III with Vertical Shear
Key Takeaway
An APC III pelvic ring injury is an unstable, high-energy trauma with complete pubic symphysis and posterior sacroiliac complex disruption, often with vertical shear. Diagnosis involves clinical assessment for instability, initial AP, Inlet, Outlet radiographs, and CT scans to define specific fracture patterns like sacral involvement and displacement, especially in hemodynamically unstable cases.
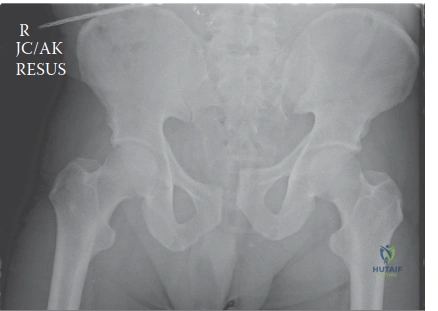
A 38-year-old male is brought to your trauma unit following a high-energy MVC. He is hypotensive and tachycardic. On the primary survey, you suspect an unstable pelvic ring injury. Based on the radiographic imaging provided, describe your findings and the immediate priorities for management.
Candidate: The X-ray shows a symphyseal diastasis and right sacroiliac joint disruption with cephalad migration. I would classify this as a Young-Burgess APC III injury with a vertical shear component. My priorities are to stabilize the pelvis with a binder, resuscitate the patient according to ATLS protocols, and obtain urgent CT imaging to assess for arterial bleeding and associated visceral injuries.
Candidates often fail to explicitly mention the "Damage Control" mindset. A poor answer focuses solely on the fracture pattern without discussing the patient's physiological status (hemodynamics). Missing the "open pelvic fracture" implications or failing to mention that you must STOP mechanical testing once the injury is recognized is a major error in an FRCS-level exam.
A high-scoring answer follows a structured approach: 1. Assessment: "This is a hemodynamically unstable patient with a combined mechanism injury (APC III + Vertical Shear)." 2. Immediate Action: Confirm correct application of the pelvic binder (over the greater trochanters, not the iliac crests). 3. Physiology: Acknowledge that the pelvic binder is a temporary resuscitative tool to reduce pelvic volume. 4. Urgency: Highlight the need for a multidisciplinary approach (Interventional Radiology for embolization vs. surgical packing) and immediately mandate a rectal/urethral assessment to rule out an open pelvic fracture, which is an orthopaedic emergency.
You mentioned the possibility of an open pelvic fracture. What are the clinical indicators for this, and why does this change your surgical management plan so dramatically?
Candidate: Indicators include blood at the urethral meatus, a high-riding prostate, or blood on rectal examination. It changes management because these patients require fecal diversion (colostomy) and aggressive surgical debridement of the pelvic space to prevent catastrophic pelvic sepsis, which has a very high mortality rate.
Forgetting that "open" doesn't just mean a skin wound—it means communication between the pelvic fracture site and the outside environment (rectum, vagina, or perineum). Candidates often fail to mention the need for general surgery input or that antibiotics and tetanus prophylaxis must be prioritized.
The candidate must define the "open" pelvic fracture as a communication between the pelvic space and a contaminated body cavity. Key management steps: 1. Multidisciplinary: General Surgery for colostomy; Urology for urethral injury management. 2. Orthopaedic: Early debridement is mandatory. 3. Prognosis: Acknowledge that this carries a significantly higher risk of osteomyelitis and systemic sepsis, moving the case from a standard trauma to an urgent, potentially life-saving surgical intervention.
Regarding definitive fixation of the posterior pelvic ring in this patient, given the vertical shear component and the comminution, what is your preferred construct and why?
Candidate: I would use trans-iliac trans-sacral (TITS) screw fixation. The fully threaded screws engage the dense bone of the contralateral ilium, which provides superior biomechanical stability against vertical shear forces compared to unilateral iliosacral screws.
Suggesting a single iliosacral screw. The examiner is looking for the recognition that standard unilateral screws are insufficient for vertical shear. Failing to mention the specific advantage of the fully threaded screw and the contralateral purchase is a technical oversight.
Structure your answer around the biomechanical necessity: 1. Anatomy: Mention the vertical instability and the potential for late displacement. 2. Construct: Advocate for TITS (Trans-iliac Trans-sacral) screws. 3. Rationale: Explain that these screws act as "internal splints," creating a tension band effect that resists vertical shear, noting that fully threaded screws are critical here to provide stable purchase in the dense bone of both ilia.
