Proximal Femoral Atypical Cartilaginous Tumor/Low-Grade Chondrosarcoma: A Diagnostic Imaging Case Study

Key Takeaway
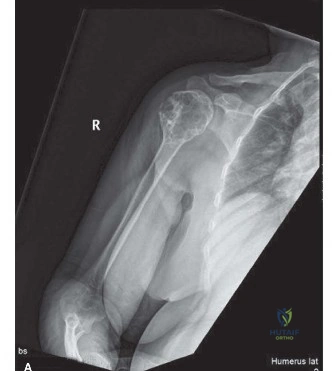
Proximal femoral chondrosarcoma diagnosis integrates patient history, physical exam, and key imaging. Radiographs, CT, and MRI reveal characteristic expansile intramedullary lytic lesions with "rings and arcs" calcifications and significant endosteal scalloping, crucial for identifying this low-grade cartilaginous tumor.
A 62-year-old presents with 8 months of dull, progressive left hip pain and nocturnal symptoms. Examination reveals a dynamic Trendelenburg sign and a palpable mass in the proximal vastus lateralis. Based on these radiographs, what is your differential diagnosis and how do you differentiate the most likely pathology from an enchondroma?
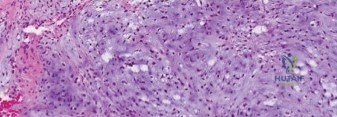
Candidate: The primary differential for an intramedullary cartilaginous lesion in this age group includes an Atypical Cartilaginous Tumor (ACT)/Grade 1 Chondrosarcoma versus a benign enchondroma. I would differentiate them based on clinical symptoms (nocturnal pain suggests ACT), lesion size (>5cm suggests ACT), and the degree of endosteal scalloping, with >2/3 cortical thickness strongly favoring an ACT.
Focusing only on the "rings and arcs" calcification. All chondroid lesions show this; it is not a differentiator. A poor candidate also fails to mention the clinical significance of nocturnal pain or the critical importance of quantifying endosteal scalloping as a marker for biological activity.
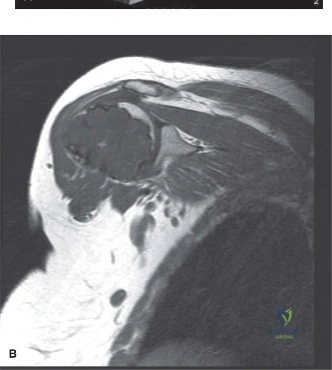
Structure your answer: 1. Clinical (Nocturnal pain is the key red flag). 2. Radiographic (Size >5cm, endosteal scalloping >2/3 of cortical thickness, and cortical remodeling/thickening). 3. Advanced Imaging (MRI showing peritumoral edema, which is a marker of activity). Explicitly state that these findings warrant a biopsy to exclude an ACT before proceeding with management.
The imaging confirms an ACT of the proximal femur. You decide to perform intralesional curettage. How do you assess the risk of pathologic fracture, and what specific steps in your surgical technique mitigate the complications associated with this lesion?
Candidate: I would use the Mirels' criteria to quantify fracture risk; this patient scores 10, indicating high risk. To mitigate complications, I would perform an extended intralesional curettage using a high-speed burr to reach healthy bone, apply local adjuvants like phenol or argon beam coagulation, and stabilize the femur with a cephalomedullary nail, which provides load-sharing fixation and allows the PMMA cement to act as a structural and adjuvant support.
Suggesting a plate for fixation. A plate acts as a stress riser in a proximal femoral lesion; a load-sharing device (cephalomedullary nail) is mandatory. Failing to mention "extended" curettage (burring) leads to higher recurrence rates due to microscopic tumor persistence.
Articulate the "Extended Curettage" principle: 1. Mechanical clearance (curettes). 2. Extended clearance (High-speed burr to remove permeative disease). 3. Adjuvant therapy (Thermal/Chemical necrosis). 4. Load-sharing stabilization (Cephalomedullary nail). Mentioning the use of PMMA as both a structural spacer and a source of exothermic (thermal) adjuvant therapy demonstrates high-level surgical planning.
You are performing the curettage. What are the specific risks regarding the biopsy track, and how do you handle the cortical window to minimize the risk of a post-operative fracture?
Candidate: The biopsy track must be considered contaminated tissue and should be excised in continuity with the surgical approach. For the cortical window, I must avoid sharp, angular corners, which create stress risers. I would use a high-speed burr to round the corners of the window and ensure that the prophylactic cephalomedullary nail spans the entire bone to neutralize the stress created by the cortical defect.
Forgetting to excise the biopsy track. Examiners consider this a critical oncologic error. Also, failing to recognize that a rectangular window, even if filled with cement, is an iatrogenic fracture risk if the construct is not robust.
Combine oncologic and biomechanical principles: "The biopsy tract is a zone of contamination that must be resected." Then explain the biomechanics: "Rounded corners on the cortical window reduce stress concentration factors. The cephalomedullary nail transforms a high-risk stress riser into a load-sharing construct, allowing for early mobilization."
