Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 4)

Key Takeaway
Looking for accurate information on Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 4)? Top-rated Orthopedic Sports Medicine 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 4)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 15-year-old diver has had persistent, activity-related low back pain for the past 2 months. He denies any history of trauma. Examination reveals that the pain is localized to the lumbosacral junction, and there are no radicular symptoms. The pain is worse with back extension. Neurologic examination is normal, as are AP, lateral, and oblique radiographs of the lumbosacral spine. Further evaluation should include
Explanation
Question 2
A 23-year-old college basketball player reports persistent lateral ankle pain after sustaining an inversion injury 6 months ago. Examination reveals pain over the anterolateral ankle, absence of swelling, and no clinical instability. Management consisting of vigorous physical therapy fails to provide relief, and a intra-articular corticosteroid injection provides only temporary relief. Radiographs obtained at the time of injury and subsequent AP and varus stress views are normal. A recent MRI scan fails to show any abnormalities. Management should now include
Explanation
Question 3
Which of the following tissues used for anterior cruciate ligament (ACL) reconstruction has the highest maximum load to failure?
Explanation
Question 4
Creatine is currently being used by athletes as a dietary supplement in an attempt to enhance performance. What is the physiologic basis for its use?
Explanation
Question 5
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?
Explanation
Question 6
Which of the following methods of meniscal repair has the highest load to failure strength?
Explanation
Question 7
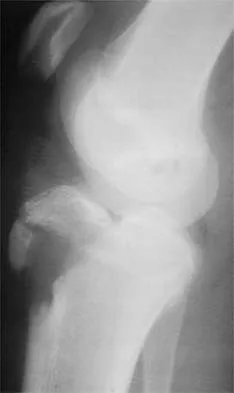
Figure 35 shows the lateral radiograph of a 15-year-old basketball player who felt a dramatic pop in his knee when landing after a lay-up. The patient reports that he cannot bear weight on the injured extremity. Management should consist of
Explanation
Question 8
A 52-year-old man has pain in the sternal area after landing on his right shoulder in a fall from his bicycle. In addition, he reports that he had difficulty swallowing and breathing immediately after the fall, but the symptoms resolved. A CT scan reveals a posterior sternoclavicular dislocation. Initial management should include
Explanation
Question 9
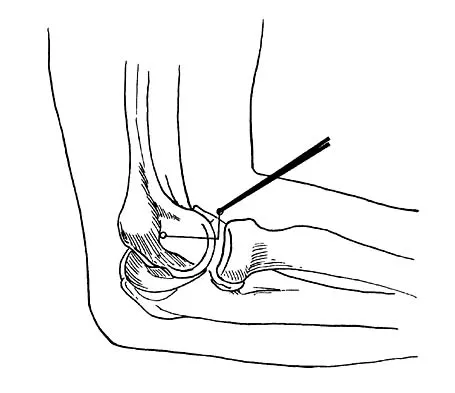
What nerve is at greatest risk of harm from the portal shown in Figure 36?
Explanation
Question 10
In the majority of patients with chronic anterior cruciate ligament (ACL)-deficient knees, analysis of the gait pattern during level walking will most likely reveal which of the following changes?
Explanation
Question 11
Glenohumeral inferior stability in the adducted shoulder position is primarily a function of the
Explanation
Question 12
A 20-year-old football player has repeated episodes of heat cramps during summer training sessions. A deficiency of what electrolyte is most responsible for heat cramps?
Explanation
Question 13
Figure 37 shows the radiograph of a 23-year-old football player who sustained a blow to the anterior aspect of his shoulder. Examination reveals pain and limited rotation. He is unable to flex the arm above the shoulder. Management should include which of the following studies?
Explanation
Question 14
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
Question 15
A 24-year-old baseball pitcher reports pain over the posterior aspect of his shoulder that occurs only during throwing. He notes that the discomfort is greatest during the late cocking and early acceleration phases. Examination reveals localized tenderness with palpation over the external rotators and posterior glenoid. Radiographs are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
Question 16
What percent of the adult human meniscus is vascularized?
Explanation
Question 17
A 30-year-old man who participates in recreational sports reports the spontaneous onset of intermittent pain and swelling about the right knee. Examination reveals a 3+ effusion, with a range of motion of 10 degrees to 60 degrees. He has mild diffuse tenderness but no instability. MRI scans and an arthroscopic view are shown in Figures 39a through 39c. Management should consist of
Explanation
Question 18
Figure 40 shows the plain radiograph of a 30-year-old woman who has had a long history of standing bilateral anterior knee pain and a sense of patellar instability without frank dislocation. Nonsurgical management consisting of anti-inflammatory drugs and physical therapy has failed to provide relief. Examination reveals full range of motion of both knees, with moderate patellofemoral crepitance. Patellar apprehension and patellar grind tests are positive. The Q-angle measures 20 degrees. Management should now consist of
Explanation
Question 19
A 24-year-old runner who underwent an allograft reconstruction of the anterior cruciate ligament (ACL) 3 years ago now reports anterior knee pain. Examination reveals no swelling or effusion, and the patient has full motion. A Lachman test and a pivot-shift test are negative. Palpation reveals tenderness on the patellar tendon and at the inferior pole of the patella. AP and lateral radiographs are shown in Figures 41a and 41b. Management should consist of
Explanation
Question 20
What is the most common mechanism of injury that produces turf toe?
Explanation
Question 21
A 68-year-old man embarks on a 24-week strength training program. He trains at 80% of his single repetition maximum for both the upper and lower extremities. Which of the following changes can be anticipated?
Explanation
Question 22
A 26-year-old ballet dancer reports posterolateral ankle pain, especially with maximal plantar flexion. Examination reveals maximal tenderness just posterior to the lateral malleolus, and symptoms are heightened with forced passive plantar flexion. Radiographs are shown in Figures 42a and 42b. What is the most likely cause of the patient's symptoms?
Explanation
Question 23
A 23-year-old soccer player sustains a grade III complete posterior cruciate ligament (PCL) tear after colliding with another player. In reconstructing the PCL, it is optimal to reconstruct the
Explanation
Question 24
Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show
Explanation
Question 25
A 10-year-old soccer player has bilateral heel pain and reports that the pain is worse during and immediately after sports. Examination reveals that the calcaneal tuberosities are painful to palpation bilaterally. What is the most likely diagnosis?
Explanation
Question 26
A 22-year-old collegiate baseball pitcher presents with posterior shoulder pain during the late cocking phase of throwing. Physical examination demonstrates a 20-degree glenohumeral internal rotation deficit (GIRD) compared to the contralateral shoulder.
What is the primary pathomechanical cause of this patient's internal impingement?

Explanation
Question 27
A 26-year-old male sustains an isolated posterior cruciate ligament (PCL) rupture in a motorcycle accident and fails nonoperative management. A single-bundle PCL reconstruction is planned.
To correctly recreate the anterolateral (AL) bundle, the femoral tunnel should be placed at which of the following locations?

Explanation
Question 28
During surgical reconstruction of a multiligament knee injury, the surgeon isolates the fibular collateral ligament (FCL) to recreate its native anatomy.
Where is the correct anatomical location of the native FCL femoral attachment?
Explanation
Question 29
A 45-year-old female experiences a sudden pop in the back of her knee while squatting. MRI reveals a posterior root tear of the medial meniscus with 4 mm of meniscal extrusion.
Biomechanical studies demonstrate that this specific injury pattern alters tibiofemoral contact pressures equivalent to which of the following?

Explanation
Question 30
A 30-year-old cyclist sustains a Type V acromioclavicular (AC) joint injury. During open reduction and reconstruction, the surgeon focuses on restoring the primary restraint to superior clavicular translation.
Which ligament acts as this primary restraint?
Explanation
Question 31
A 22-year-old hockey player undergoes hip arthroscopy for symptomatic femoroacetabular impingement (FAI). Radiographs show an alpha angle of 65 degrees.
To address the cam deformity, osteochondroplasty is most commonly performed in which region of the femoral head-neck junction?

Explanation
Question 32
A 17-year-old female presents with her first episode of lateral patellar dislocation. An MRI confirms rupture of the medial patellofemoral ligament (MPFL).
Where is the native femoral footprint of the MPFL located in relation to the medial epicondyle and adductor tubercle?

Explanation
Question 33
A 25-year-old professional tennis player undergoes arthroscopic repair of a Type II superior labrum anterior-posterior (SLAP) lesion.
What is the most commonly reported complication following this specific procedure in overhead athletes?

Explanation
Question 34
A 13-year-old gymnast complains of vague, activity-related anterior knee pain. Imaging reveals an osteochondritis dissecans (OCD) lesion with intact overlying cartilage.
What is the most common anatomical location for this pathology in the knee?

Explanation
Question 35
A 20-year-old collegiate javelin thrower is evaluated for medial elbow pain. The moving valgus stress test is highly positive at 90 degrees of flexion.
Which specific structure is the primary restraint to valgus stress at this angle of elbow flexion?

Explanation
Question 36
A 32-year-old powerlifter feels a tearing sensation in his chest while attempting a maximal bench press. Examination reveals an asymmetric chest wall and weakness in internal rotation.
Which anatomical segment of the involved muscle is most frequently ruptured, and where does it insert on the humerus?

Explanation
Question 37
A 19-year-old soccer player is scheduled for ACL reconstruction. The surgeon discusses autograft choices, including bone-patellar tendon-bone (BTB) and hamstring.
In comparative studies, what complication is significantly more common with BTB autograft than with hamstring autograft?

Explanation
Question 38
Following an arthroscopic repair of a full-thickness supraspinatus tear, the tendon undergoes a complex biological healing process.
How does the healed tendon-to-bone interface typically present histologically?

Explanation
Question 39
A 24-year-old rugby player sustains an external rotation injury to the ankle. Examination reveals tenderness over the anterior syndesmosis, and radiographs demonstrate widening of the tibiofibular clear space.
Which ligament provides the greatest absolute resistance to diastasis of the distal tibiofibular syndesmosis?

Explanation
Question 40
A 40-year-old male is brought to the trauma bay after a high-speed skiing collision. His knee is grossly deformed with a prominent "dimple sign" over the medial joint line.
What does this specific clinical finding indicate regarding the injury?
Explanation
Question 41
A 22-year-old soccer player undergoes an anatomic single-bundle anterior cruciate ligament (ACL) reconstruction. Which of the following is the most likely consequence of placing the femoral tunnel too far anteriorly (shallow) in the intercondylar notch?
Explanation
Question 42
A 17-year-old female presents with recurrent lateral patellar dislocations. Imaging shows a TT-TG distance of 14 mm, normal patellar height, and a torn medial patellofemoral ligament (MPFL). She undergoes isolated MPFL reconstruction. Where is the anatomic femoral attachment of the MPFL located?
Explanation
Question 43
A 28-year-old bodybuilder feels a pop in his anterior axilla while performing a heavy bench press. Examination reveals loss of the anterior axillary fold and weakness in internal rotation. Which segment of the pectoralis major tendon is under the most tension and most likely to rupture first during the eccentric phase of a bench press?
Explanation
Question 44
A 55-year-old physically active man reports a popping sensation in his posterior knee while squatting, followed by acute posteromedial joint line pain. MRI reveals a medial meniscus posterior root tear.
Biomechanical studies demonstrate that an un-repaired complete posterior root tear alters knee joint contact pressures most similarly to which of the following?
Explanation
Question 45
A 21-year-old collegiate baseball pitcher presents with vague posterior shoulder pain and a decrease in pitching velocity. Examination reveals 15 degrees of internal rotation and 120 degrees of external rotation in the dominant arm, compared to 60 degrees of internal rotation and 90 degrees of external rotation in the non-dominant arm. Which of the following is the most appropriate initial management?
Explanation
Question 46
A 45-year-old recreational tennis player has persistent deep shoulder pain. MRI shows an isolated Type II Superior Labrum Anterior Posterior (SLAP) tear. He undergoes arthroscopic evaluation. What is the most reliable predictor of failure if a primary SLAP repair is performed in this patient instead of a biceps tenodesis?
Explanation
Question 47
A 20-year-old rugby player presents with his third anterior shoulder dislocation. A CT scan with 3D reconstruction is obtained.
Measurements indicate a 25% anterior glenoid bone loss. What is the most appropriate surgical intervention to minimize the risk of recurrent instability?
Explanation
Question 48
A 19-year-old collegiate swimmer presents with insidious onset bilateral shoulder pain. Physical examination demonstrates a 2+ sulcus sign bilaterally, apprehension at end-range abduction/external rotation without a distinct subluxation event, and generalized ligamentous laxity. What is the most appropriate initial management?
Explanation
Question 49
When comparing bone-patellar tendon-bone (BTB) autograft to hamstring autograft for anterior cruciate ligament (ACL) reconstruction, BTB autograft is associated with a statistically higher incidence of which of the following postoperative complications?
Explanation
Question 50
A 22-year-old collegiate baseball pitcher is diagnosed with a Type II superior labrum anterior and posterior (SLAP) tear. During which phase of throwing does the 'peel-back' mechanism place maximal strain on the biceps anchor?
Explanation
Question 51
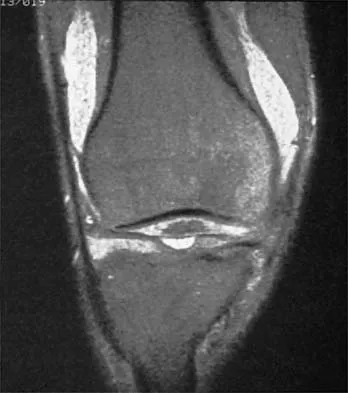
A 50-year-old moderately active female feels a 'pop' in her posterior knee while squatting. An MRI is obtained as seen in the figure.
It demonstrates a medial meniscus posterior root tear with 4 mm of extrusion and minimal osteoarthritis. What is the most appropriate surgical management?
Explanation
Question 52
A 24-year-old competitive rugby player sustains his third anterior shoulder dislocation. A pre-operative CT scan demonstrates 28% anterior glenoid bone loss. Which of the following surgical interventions is most appropriate?
Explanation
Question 53
A 12-year-old boy presents with vague anterior knee pain. Radiographs demonstrate a 1.5 cm osteochondritis dissecans (OCD) lesion of the medial femoral condyle.
MRI reveals no fluid behind the lesion, and his physes are wide open. What is the recommended initial management?
Explanation
Question 54
A 10-year-old skeletally immature female soccer player sustains an anterior cruciate ligament (ACL) tear. She is Tanner stage 1 with significant growth remaining. Which of the following surgical techniques has the lowest risk of causing a growth arrest?
Explanation
Question 55
A 45-year-old woman sustains a posterior root tear of the medial meniscus. Biomechanically, this injury alters the joint contact pressures to be most equivalent to which of the following scenarios?
Explanation
Question 56
A 22-year-old rugby player undergoes a Latarjet procedure for recurrent anterior shoulder instability with 25% glenoid bone loss. Postoperatively, he presents with an inability to actively flex his elbow or supinate his forearm. Which nerve is most likely injured?
Explanation
Question 57
During medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar instability, the femoral attachment must be accurately positioned. Which of the following describes the correct radiographic landmark (Schöttle's point) for the femoral footprint on a true lateral view?
Explanation
Question 58
A 28-year-old male is brought to the emergency department after a high-velocity knee dislocation. His knee is reduced, but the ankle-brachial index (ABI) is 0.8. Which of the following is the most appropriate next step in management?
Explanation
Question 59
A 26-year-old athlete presents with a symptomatic 4.0 cm² osteochondral defect of the medial femoral condyle with 5 mm of subchondral bone loss. Nonoperative management has failed. Which of the following is the most appropriate surgical intervention?
Explanation
Question 60
A 25-year-old hockey player presents with anterior hip pain exacerbated by hip flexion, adduction, and internal rotation. Radiographs reveal a crossover sign and an alpha angle of 65 degrees. What is the most likely combination of pathomorphologies?
Explanation
Question 61
A 32-year-old weightlifter feels a "pop" in his anterior chest while performing a heavy bench press. Examination reveals ecchymosis and loss of the anterior axillary fold. If surgical repair is planned, which portion of the pectoralis major tendon is most commonly ruptured and requires mobilization?
Explanation
Question 62
A 21-year-old runner complains of bilateral anterolateral leg pain that reliably begins 15 minutes into a run and resolves 30 minutes after rest. Nonoperative measures have failed. What is the gold standard diagnostic test for this condition?
Explanation
Question 63
A 40-year-old male sustains an acute Achilles tendon rupture. When discussing surgical versus nonoperative management with a functional rehabilitation protocol, the patient should be informed that surgical repair provides which of the following advantages?
Explanation
Question 64
A 20-year-old collegiate baseball pitcher presents with medial elbow pain and decreased pitching velocity. The moving valgus stress test is positive. MRI confirms a full-thickness tear of the anterior bundle of the ulnar collateral ligament (UCL). During reconstruction, where must the graft be secured on the ulna to recreate the native anterior bundle insertion?
Explanation
Question 65
A 60-year-old male presents with a massive, irreparable posterosuperior rotator cuff tear. He has an intact subscapularis, no glenohumeral arthritis (Hamada grade 1), but demonstrates a positive hornblower's sign. Which of the following joint-preserving procedures is most indicated to restore active external rotation?
Explanation
Question 66
A 45-year-old water skier sustains a hyperflexion injury of the hip with the knee extended. He has severe posterior thigh pain and a palpable defect at the ischial tuberosity. MRI shows a complete 3-tendon proximal hamstring avulsion with 4 cm of retraction. What is the most appropriate management?
Explanation
Question 67
A 48-year-old recreational tennis player presents with vague anterior shoulder pain. An MRI arthrogram reveals a Type II SLAP tear. He has failed 6 months of nonoperative management. What is the currently recommended surgical intervention for this specific demographic?
Explanation
Question 68
A 30-year-old male sustains a severe varus and hyperextension injury to his knee. Examination reveals a positive dial test (increased external rotation) at 30 degrees of knee flexion, but the external rotation normalizes to match the contralateral knee at 90 degrees of flexion. What is the primary injured structure?
Explanation
Question 69
A 22-year-old rugby player undergoes an open Latarjet procedure for recurrent anterior shoulder instability. Postoperatively, he presents with numbness over the lateral aspect of his forearm and weakness in elbow flexion. Which nerve is most likely injured?
Explanation
Question 70
During clinical examination of a multiligamentous knee injury, the dial test is performed. At 30 degrees of knee flexion, the primary restraint to external rotation of the tibia is the:
Explanation
Question 71
A 30-year-old weightlifter suffers a complete rupture of the pectoralis major tendon. Regarding the normal anatomy of the pectoralis major footprint on the humerus, the sternal head inserts:
Explanation
Question 72
If a femoral tunnel is placed too anteriorly (high in the notch in extension) during an anterior cruciate ligament (ACL) reconstruction, what is the resulting biomechanical effect on the graft?
Explanation
Question 73
The peel-back mechanism responsible for Type II SLAP lesions in overhead-throwing athletes occurs maximally in which shoulder position?
Explanation
Question 74
Following hip arthroscopy for femoroacetabular impingement utilizing a perineal traction post, the patient reports severe numbness in the groin and scrotum. Neuropraxia of which nerve is the most likely cause?
Explanation
Question 75
Biomechanical studies show that a complete, unrepaired tear of the posterior root of the medial meniscus alters knee contact mechanics equivalent to:
Explanation
Question 76
During ulnar collateral ligament (UCL) reconstruction of the elbow, the graft is typically anchored to the anatomic footprints. The anterior bundle of the UCL originates from the anteroinferior medial epicondyle and inserts onto the:
Explanation
Question 77
During anatomical reconstruction of the coracoclavicular (CC) ligaments for a high-grade acromioclavicular joint separation, proper graft placement requires knowledge of the native footprint. The conoid ligament footprint on the clavicle is located:
Explanation
Question 78
A 22-year-old soccer player sustains a non-contact knee injury. Radiographs show an elliptic bone fragment adjacent to the lateral tibial plateau. What structure is typically attached to this avulsed fragment?
Explanation
Question 79
A 21-year-old collegiate rugby player presents with recurrent anterior shoulder instability. CT scan demonstrates 28% anterior glenoid bone loss. What is the most appropriate definitive surgical management?
Explanation
Question 80
A 48-year-old female experiences a pop in her posterior knee while deep squatting. MRI reveals a medial meniscus posterior root tear with 3 mm of extrusion. What is the primary biomechanical consequence if this injury is left untreated?
Explanation
Question 81
When performing a single-bundle posterior cruciate ligament (PCL) reconstruction, which native bundle is recreated to restore primary restraint against posterior tibial translation in flexion?
Explanation
Question 82
A 22-year-old baseball pitcher presents with medial elbow pain and decreased velocity. Pain is most severe during the late cocking and early acceleration phases of throwing. Which bundle of the ulnar collateral ligament (UCL) is most likely injured and serves as the primary restraint to valgus stress at 90 degrees of flexion?
Explanation
Question 83
A 32-year-old weightlifter felt a tearing sensation in his anterior axilla while performing a heavy bench press. Exam reveals loss of the anterior axillary fold. He undergoes surgical repair. During anatomic repair, what is the correct orientation of the sternocostal head insertion on the humerus relative to the clavicular head?
Explanation
Question 84
A 28-year-old female undergoes hip arthroscopy for femoroacetabular impingement. Postoperatively, she reports profound numbness in the perineal region and labia. Which nerve was most likely injured due to intraoperative traction on the perineal post?
Explanation
Question 85
A 17-year-old female experiences recurrent lateral patellar instability and is scheduled for a medial patellofemoral ligament (MPFL) reconstruction. Where is the exact anatomical location of the femoral origin of the MPFL (Schottle's point)?
Explanation
Question 86
A 24-year-old football player sustained a direct blow to the anteromedial aspect of his knee. Physical examination reveals increased external tibial rotation of 15 degrees compared to the contralateral side at 30 degrees of knee flexion, but symmetrical external rotation at 90 degrees. What is the most likely injury pattern?
Explanation
Question 87
A 25-year-old athlete undergoes an arthroscopic microfracture for a 1.5 cm^2 full-thickness chondral defect on the medial femoral condyle. What is the predominant type of collagen in the reparative tissue generated by this procedure?
Explanation
Question 88
A 30-year-old overhead athlete undergoes an arthroscopic Type II SLAP repair. Six months postoperatively, he complains of persistent pain and a significant loss of external rotation. What is the most common iatrogenic cause of this complication?
Explanation
Question 89
A 19-year-old female collegiate runner presents with an anterior tibial stress fracture and reports irregular menstrual cycles for the past year. Dual-energy x-ray absorptiometry reveals low bone mineral density. What is the primary underlying physiological mechanism for her condition (Relative Energy Deficiency in Sport)?
Explanation
None
