Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 2)
Key Takeaway
We review everything you need to understand about Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 2). Top-rated Orthopedic Sports Medicine 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 2)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 11 shows the radiograph of an 18-year-old soccer player who reports recurrent lateral foot pain after sustaining an inversion injury. History reveals that 6 months ago he had been treated in a non-weight-bearing cast for a fifth metatarsal fracture. Management should consist of
Explanation
Question 2
Which of the following types of exercise used to increase flexibility is considered most beneficial in increasing joint range of motion?
Explanation
Question 3
The view from an anterosuperior portal of the right shoulder shown in Figure 12 reveals which of the following findings?
Explanation
Question 4
An 18-year-old football player has intense pain and is unable to bear weight on the right knee after being tackled from the front. A posterior knee dislocation is reduced on the field. Because the game took place in a remote location, the patient is not examined in the emergency department until 5 hours after the injury. Examination now shows a grossly swollen knee with moderate ischemia in the lower leg. Posterior tibial and dorsalis pedis pulses are diminished. The best course of action should be to
Explanation
Question 5
A 17-year-old football player is unable to flex the distal interphalangeal (DIP) joint of his ring finger. He states that he injured the finger 6 weeks ago while attempting to tackle another player who pulled free from his grip, but he did not inform his coach at the time of the injury. Current radiographs show an observable fleck of bone volar to the base of the proximal phalanx. Treatment should consist of
Explanation
Question 6
A 48-year-old ski instructor dislocates his nondominant shoulder in a fall. Management consisting of application of a sling for 1 week results in improvement in his pain. Follow-up examination 6 weeks after the injury reveals that the patient continues to have difficulty with shoulder elevation. Management should now include
Explanation
Question 7
Figure 13 shows the MRI scan of a 29-year-old rock climber who reports increasing shoulder pain and weakness. Based on these findings, atrophy will most likely occur in which of the following muscles?
Explanation
Question 8
A 46-year-old man has acute tenderness along the ulnar aspect of the wrist after falling on his outstretched hand while playing basketball. Examination reveals tenderness and mild swelling along the volar ulnar aspect of the wrist. Radiogaphs are shown in Figures 14a through 14c. Management should consist of
Explanation
Question 9
A 32-year-old powerlifter who was performing a dead lift 3 days ago noted a sharp pain in the front of his dominant right arm just after beginning to lower the weight. He now reports pain in the anterior aspect of the arm that worsens when he opens a door. Examination reveals moderate ecchymosis and swelling of the forearm and tenderness in the antecubital fossa. The MRI scans are shown in Figures 15a and 15b. If the injury is left unrepaired, the greatest functional deficit will most likely be the loss of
Explanation
Question 10
Figure 16 shows the lateral radiograph of a patient who is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. If the graft is tensioned at 20 degrees of flexion and the femoral tunnel is created by passing a reamer over the guide wire marked "A," the resulting ligament reconstruction will excessively
Explanation
Question 11
Which of the following nerves is most commonly injured during revision surgery following a Bristow procedure?
Explanation
Question 12
A 17-year-old high school soccer player sustains an anterior cruciate ligament (ACL) tear at the beginning of the season. An MRI scan confirms a complete ACL tear with no meniscal injuries. The patient plans an early return to play and would like to avoid surgery. Therefore, the patient and family should be advised that nonsurgical management consisting of rehabilitative exercises and the use of a functional knee brace will most likely result in
Explanation
Question 13
A patient underwent anterior stabilization of the shoulder 6 months ago, and examination now reveals lack of external rotation beyond 0 degrees. The patient has a normal apprehension sign and normal strength, and the radiographs are normal. Based on these findings, the patient is at greater risk for the development of
Explanation
Question 14
A 13-year-old girl who competes in gymnastics reports the insidious onset of lateral left elbow pain over the past 6 months. She also notes occasional catching episodes in the elbow; however, she denies any history of trauma. Examination reveals tenderness over the lateral epicondyle and extensor muscle origin. The elbow is stable and has full flexion, but lacks 10 degrees of full extension. An AP plain radiograph and an MRI scan are shown in Figures 17a and 17b. Management of the elbow should consist of
Explanation
Question 15
A 25-year-old man injures his shoulder while skiing. Examination reveals increased passive external rotation, pain in the cocked position, and a positive lift-off test. What is the most likely diagnosis?
Explanation
Question 16
A college basketball player is struck in the eye by a player's hand while driving to the basket. Fluorescein evaluation reveals the injury shown in Figure 18. Management should consist of
Explanation
Question 17
In patient selection for meniscal allograft transplantation, which of the following variables has the greatest influence on outcome?
Explanation
Question 18
A 10-year-old boy sustained an injury to the left knee. The radiographic findings shown in Figure 19 are most commonly associated with injury to which of the following structures?
Explanation
Question 19
What is the single most important nutritional factor affecting athletic performance?
Explanation
Question 20
A right-handed 20-year-old college baseball pitcher has had a 6-month history of vague right elbow pain while pitching. Examination reveals full flexion of the elbow and a loss of only a few degrees of full extension. The elbow is stable, but palpation reveals tenderness over the olecranon. Plain radiographs are inconclusive. MRI and CT scans are shown in Figures 20a and 20b. Management should consist of
Explanation
Question 21
What is the most common associated pathology in patients who have suprascapular nerve entrapment secondary to ganglion cysts?
Explanation
Question 22
A 27-year-old runner training for his first marathon reports lateral knee pain after an unusually long training run. He states that the most significant pain occurs while running downhill. Examination of the patient while he is laying on the unaffected side reveals increased pain when manual pressure is applied to the lateral femoral epicondylar area during knee range of motion of 30 degrees to 45 degrees. What is the most likely diagnosis?
Explanation
Question 23
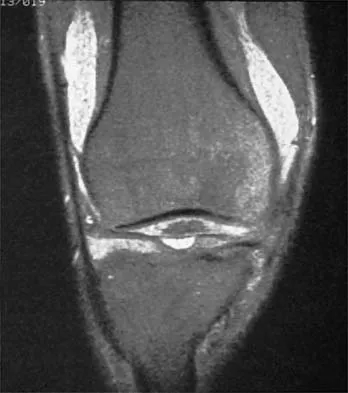
A 30-year-old woman who runs approximately 30 miles a week has had right hip and groin pain for the past 3 weeks. Examination reveals an antalgic gait, limited motion of the right hip, and pain, especially with internal and external rotation. Plain radiographs are normal, and an MRI scan is shown in Figure 21. Management should consist of
Explanation
Question 24
Which of the following primary prognostic factors best predicts the outcome of the knee lesion shown in Figure 22?
Explanation
Question 25
Figures 23a and 23b show the AP and lateral radiographs of the elbow of a 30-year-old professional pitcher. The pathology shown in these studies is most consistent with which of the following conditions?
Explanation
Question 26
A 19-year-old collegiate female soccer player tears her ACL and elects to undergo reconstruction using a bone-patellar tendon-bone (BTB) autograft. Which of the following is the most common postoperative complication specific to this graft choice?
Explanation
Question 27
A 50-year-old active man presents with acute medial joint line pain after a deep squat. MRI reveals a medial meniscus posterior root tear with 3 mm of extrusion. To prevent rapid joint degeneration, which of the following is the most appropriate management?
Explanation
Question 28
A 22-year-old rugby player with recurrent anterior shoulder instability and 25% glenoid bone loss undergoes a Latarjet procedure. Which nerve is at greatest risk of iatrogenic injury during the coracoid preparation and transfer?
Explanation
Question 29
A 45-year-old man falls onto his outstretched arm and subsequently demonstrates weakness in internal rotation. Physical examination reveals a positive lift-off test and increased passive external rotation compared to the contralateral shoulder. Which structure is most likely injured?
Explanation
Question 30
A 28-year-old male presents with a dashboard injury and a positive posterior drawer test at 90 degrees of flexion. Radiographs reveal a displaced bony avulsion fragment from the posterior tibia. What is the recommended optimal treatment?
Explanation
Question 31
A 17-year-old female undergoes medial patellofemoral ligament (MPFL) reconstruction for recurrent lateral patellar dislocations. If the femoral tunnel is placed too proximal and anterior to Schöttle's point, what is the expected clinical consequence?
Explanation
Question 32
A 25-year-old hockey player undergoes hip arthroscopy with femoral neck osteochondroplasty for a cam-type femoroacetabular impingement. Resection of more than what percentage of the femoral neck diameter significantly increases the risk of an iatrogenic postoperative fracture?
Explanation
Question 33
A 21-year-old collegiate baseball pitcher elects to undergo ulnar collateral ligament (UCL) reconstruction after failing conservative management. Which nerve must be carefully protected, and potentially transposed, during this procedure?
Explanation
Question 34
A 24-year-old wide receiver sustains an external rotation injury to his ankle. He exhibits tenderness over the anterior inferior tibiofibular ligament (AITFL) and has a positive external rotation stress test. Which imaging modality is most sensitive for detecting subtle syndesmotic diastasis?
Explanation
Question 35
A 19-year-old cyclist sustains a midshaft clavicle fracture after a high-speed crash. Which of the following findings is an absolute indication for operative fixation?
Explanation
Question 36
A 35-year-old recreational basketball player opts for a percutaneous Achilles tendon repair following an acute rupture. Injury to which nerve is the most frequently cited complication of this specific minimally invasive technique?
Explanation
Question 37
A 14-year-old male gymnast presents with lateral elbow pain and catching. MRI shows an unstable osteochondritis dissecans (OCD) lesion of the capitellum with an intra-articular loose body. What is the most appropriate definitive management?
Explanation
Question 38
A 22-year-old distance runner undergoes intracompartmental pressure testing for suspected chronic exertional compartment syndrome. According to the Pedowitz criteria, which of the following measurements confirms the diagnosis?
Explanation
Question 39
A 30-year-old male sustains a spontaneously reduced knee dislocation during a football game. His pedal pulses are palpable, but his ankle-brachial index (ABI) is 0.8. What is the most appropriate next step in management?
Explanation
Question 40
A 42-year-old recreational weightlifter fails conservative treatment for a type II SLAP tear. Given his age demographic, what is the generally preferred surgical intervention to achieve reliable pain relief and return to function?
Explanation
Question 41
A 45-year-old man undergoes a single-incision anterior approach for an acute distal biceps tendon repair. During the drilling of the posterior radial cortex for a cortical button, which nerve is at the greatest risk of injury?
Explanation
Question 42
A 19-year-old female cross-country runner with 8 months of amenorrhea sustains a femoral neck stress fracture. What is the primary underlying physiological mechanism driving her decreased bone mineral density as part of the female athlete triad?
Explanation
Question 43
A 42-year-old male sustains a complete 3-tendon proximal hamstring avulsion retracted 4 cm. During the surgical approach for repair, which nerve located immediately lateral to the ischial tuberosity must be explicitly identified and protected?
Explanation
Question 44
A 60-year-old male with an irreparable massive posterosuperior rotator cuff tear undergoes a superior capsule reconstruction (SCR) to restore glenohumeral kinematics. Which of the following is the most commonly utilized biological graft for this procedure?
Explanation
Question 45
A 26-year-old snowboarder falls on an extended wrist and presents with dorsal wrist pain. Radiographs demonstrate a scapholunate interval of 4 mm and a scaphoid ring sign on the AP view. What is the most likely diagnosis?
Explanation
Question 46
A 22-year-old male rugby player presents with recurrent anterior shoulder instability. A 3D CT scan of the shoulder reveals an anterior glenoid bone loss of 25% with an engaging Hill-Sachs lesion. What is the most appropriate surgical management?
Explanation
Question 47
A 45-year-old female experiences a sudden pop in her posterior knee while deep squatting. MRI reveals a >3 mm medial meniscus extrusion and a complete radial tear at the posterior root. Which of the following best describes the biomechanical consequence of this untreated injury?
Explanation
Question 48
A 28-year-old male sustains a dashboard injury to his right knee. Physical examination reveals a positive posterior drawer test. The dial test shows 15 degrees of increased external rotation on the injured side compared to the normal side at 30 degrees of flexion, but symmetric external rotation at 90 degrees of flexion. What is the most likely diagnosis?
Explanation
Question 49
An 18-year-old female presents with recurrent lateral patellar dislocations. Advanced imaging reveals a normal patellar height (Caton-Deschamps index 1.0) but a tibial tubercle-trochlear groove (TT-TG) distance of 23 mm. What is the most appropriate surgical treatment?
Explanation
Question 50
A 20-year-old collegiate baseball pitcher reports medial elbow pain during the late cocking and early acceleration phases of throwing. Examination reveals a positive moving valgus stress test and distinct paresthesias in the ring and small fingers. MRI confirms a full-thickness ulnar collateral ligament (UCL) tear. What is the recommended surgical management?
Explanation
Question 51
A 25-year-old ice hockey player presents with chronic, deep groin pain exacerbated by hip flexion and internal rotation. An AP pelvis radiograph demonstrates a "crossover sign." This radiographic finding is indicative of which of the following pathomorphologies?
Explanation
Question 52
A 30-year-old male is brought to the emergency department after sustaining a knee dislocation during a football game. The knee was reduced on the field. On examination, the foot is warm, but the ankle-brachial index (ABI) is measured at 0.85. What is the most appropriate next step in management?
Explanation
Question 53
A 40-year-old competitive water skier sustains an acute posterior thigh injury after forceful hip flexion with the knee fully extended. MRI shows an avulsion of the conjoined tendon and semimembranosus from the ischial tuberosity with 3.5 cm of retraction. What is the most appropriate treatment?
Explanation
Question 54
During the late cocking phase of throwing, the 'peel-back' mechanism places maximal stress on which of the following glenohumeral structures, leading to a specific pattern of labral injury?
Explanation
Question 55
A 22-year-old distance runner presents with bilateral anterolateral leg pain that reliably occurs after 2 miles of running and resolves with rest. Which of the following intracompartmental pressure measurements confirms the diagnosis of chronic exertional compartment syndrome?
Explanation
Question 56
When counseling a patient on anterior cruciate ligament (ACL) reconstruction, which of the following commonly utilized graft choices possesses the highest ultimate tensile load?
Explanation
Question 57
A 28-year-old construction worker falls directly onto his shoulder and sustains a Type III acromioclavicular (AC) joint separation. Which ligament acts as the primary restraint to superior translation of the distal clavicle?
Explanation
Question 58
A 12-year-old Little League pitcher complains of progressively worsening medial elbow pain. Radiographs demonstrate widening of the medial epicondyle apophysis without significant displacement. What is the most appropriate initial management?
Explanation
Question 59
During hip arthroscopy, the placement of the anterolateral portal is performed first. Which of the following nerves is at the greatest risk of iatrogenic injury during the establishment of this specific portal?
Explanation
Question 60
An 11-year-old male soccer player presents with medial knee pain. Radiographs reveal an osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle. The physes are widely open, and MRI shows no fluid behind the lesion. What is the most appropriate initial management?
Explanation
Question 61
A post-operative lateral radiograph of a 22-year-old male following an ACL reconstruction reveals that the femoral tunnel was placed significantly anterior to the anatomic footprint. What is the expected clinical and biomechanical consequence of this tunnel malposition?
Explanation
Question 62
A 45-year-old active female presents with acute posterior medial knee pain after a deep squat. An MRI demonstrates a posterior root tear of the medial meniscus. Which of the following best describes the biomechanical consequence of this specific injury?
Explanation
Question 63
A 22-year-old rugby player with recurrent anterior shoulder instability is found to have 25% anterior glenoid bone loss on a 3D CT scan. A Latarjet procedure is planned. What is the primary stabilizing mechanism of this surgical procedure?
Explanation
Question 64
During a medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar instability, the surgeon inadvertently places the femoral tunnel 10 mm proximal to the Schöttle point. What graft tensioning mismatch is expected during the knee arc of motion?
Explanation
Question 65
A 20-year-old cross-country runner complains of bilateral leg pain and dorsal foot numbness occurring after 2 miles of running and resolving with rest. Intracompartmental pressure testing is ordered to evaluate for chronic exertional compartment syndrome. Which of the following threshold measurements confirms the diagnosis?
Explanation
Question 66
A 24-year-old professional baseball pitcher presents with vague posterior shoulder pain and decreased pitching velocity. Physical exam of the throwing shoulder reveals 20 degrees of internal rotation and 130 degrees of external rotation at 90 degrees of abduction. What is the most appropriate initial treatment?
Explanation
Question 67
A 28-year-old male powerlifter feels a tearing sensation in his anterior chest wall while performing a heavy bench press. Examination reveals an ecchymotic defect at the anterior axillary fold. He is diagnosed with a pectoralis major rupture. Which portion of the muscle is most commonly injured in this scenario?
Explanation
Question 68
A 30-year-old male is evaluated for knee pain 6 months following a motor vehicle collision. With the patient supine and the knee flexed to 90 degrees, the tibia rests in a posteriorly subluxated position. When the patient is asked to actively slide his foot forward on the exam table, the tibia translates anteriorly into an anatomic position. This examination finding is diagnostic for an injury to which structure?
Explanation
Question 69
A 29-year-old elite volleyball player complains of vague posterior shoulder pain and serving weakness. Physical examination demonstrates isolated atrophy and weakness of the infraspinatus with a normal-appearing supraspinatus. At which anatomic location is nerve compression most likely occurring?
Explanation
Question 70
A 14-year-old female gymnast complains of lateral elbow pain and occasional catching. Radiographs reveal a radiolucency at the capitellum. An MRI demonstrates a 12 mm osteochondral defect with a high T2 signal line behind the fragment. What is the most appropriate management?
Explanation
Question 71
A 35-year-old male recreational basketball player sustains an acute Achilles tendon rupture and elects to undergo a percutaneous repair. During the procedure, which nerve is at the highest risk of iatrogenic injury at the level of the distal repair, and where is it located anatomically?
Explanation
Question 72
A 22-year-old ice hockey player has chronic groin pain exacerbated by hip flexion and internal rotation. Radiographs reveal a bony prominence at the anterolateral head-neck junction. Which radiographic parameter is specifically used to quantify this cam-type impingement deformity?
Explanation
Question 73
A 24-year-old professional football receiver hyper-extends his great toe on artificial turf. He presents with severe pain, swelling, and gross instability at the first metatarsophalangeal (MTP) joint. MRI shows a complete tear of the plantar plate with proximal retraction. What is the recommended treatment to optimize his return to play?
Explanation
Question 74
A 21-year-old collegiate soccer player sustains a direct blow to the lateral aspect of her right knee. Exam shows grade II medial joint line opening with a firm endpoint at 30 degrees of flexion, but no opening at 0 degrees. MRI confirms an isolated proximal medial collateral ligament (MCL) tear. What is the most appropriate management?
Explanation
Question 75
A 20-year-old collegiate baseball pitcher reports a sudden snap and sharp medial elbow pain during a curveball pitch. Examination reveals marked pain and subjective instability with a moving valgus stress test. Which anatomical structure is most likely acutely injured?
Explanation
Question 76
A 22-year-old female soccer player undergoes anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. Which of the following is the most commonly reported long-term complication specifically associated with this graft choice compared to a hamstring autograft?
Explanation
Question 77
A 25-year-old football player sustains a knee injury. On examination, the dial test reveals 15 degrees of increased external rotation at 30 degrees of knee flexion compared to the uninjured side. However, at 90 degrees of knee flexion, the external rotation is equal bilaterally. What is the most likely injured structure?
Explanation
Question 78
A 55-year-old active female feels a pop in her posterior knee while squatting. MRI reveals a complete posterior root tear of the medial meniscus. If left untreated, the biomechanical consequences of this injury most closely resemble which of the following?
Explanation
Question 79
A 10-year-old male (Tanner stage 1) sustains a complete anterior cruciate ligament (ACL) tear. He experiences recurrent instability despite bracing and physical therapy. What is the most appropriate surgical management to minimize the risk of growth arrest?
Explanation
Question 80
A 24-year-old professional female soccer player undergoes an anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. Six months postoperatively, she complains of a persistent loss of terminal extension and a noticeable anterior 'clunk' in the knee. Magnetic resonance imaging demonstrates a localized mass of fibrous tissue anterior to the ACL graft in the intercondylar notch. What is the most likely technical error that led to this complication?
Explanation
Question 81
A 45-year-old recreational weightlifter presents with deep-seated shoulder pain exacerbated by bench press and overhead activities. Examination reveals a positive O'Brien test and tenderness in the bicipital groove. MRI arthrography demonstrates a type II SLAP tear. After failing 6 months of targeted physical therapy, which surgical intervention provides the most reliable return to sport while minimizing postoperative stiffness in this patient?
Explanation
None
