Challenging Oncology Cases: Aneurysmal Bone Cyst Diagnosis

Key Takeaway
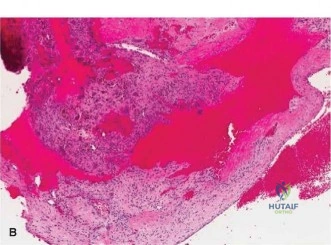
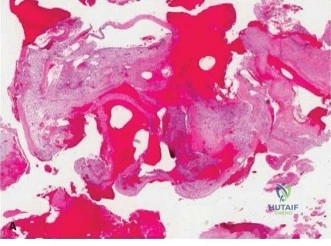
We review everything you need to understand about Challenging Oncology Cases: Aneurysmal Bone Cyst Diagnosis. Aneurysmal Bone Cysts (ABCs) are destructive, reactive bone lesions characterized by multiple blood-filled cavities. Radiographically, they present as eccentric, expanded radiolucent lesions, retaining a thin periosteal rim. Histologically, they feature cavernous blood spaces with multinucleated giant cells and no cellular atypia. MRI often confirms diagnosis with characteristic fluid-fluid levels, important for distinguishing these **oncology cases aneurysmal** manifestations.
You are in the trauma clinic. A 16-year-old boy presents with a 6-month history of insidious left shoulder pain, exacerbated by a low-energy fall during basketball. He now has a restricted, painful shoulder. You obtain these initial radiographs. How would you describe the lesion, and what is your immediate differential diagnosis?
Candidate: The radiograph shows an expansile, lytic lesion in the proximal humeral metaphysis. It has a 'soap-bubble' appearance with internal septations. There is a pathological fracture through the cortex. My main differential includes an Aneurysmal Bone Cyst (ABC), Unicameral Bone Cyst (UBC), and potentially a Telangiectatic Osteosarcoma or Giant Cell Tumor.
Candidates often fail to describe the lesion using standard terminology (e.g., Lodwick classification, zone of transition, cortical thinning). They also frequently omit the age-specific probability; for instance, failing to note that a GCT is highly unlikely prior to physeal closure, or failing to acknowledge the urgency of ruling out malignancy in any lesion with a pathological fracture.
Describe the location (metaphyseal), margin (geographic, Lodwick IB/IC), and morphology (expansile, multiloculated 'soap-bubble'). Mention the pathological fracture. Structuring the differential by probability: 1. Aneurysmal Bone Cyst (most likely given age and appearance), 2. Unicameral Bone Cyst (though usually more central/less expansile), 3. Telangiectatic Osteosarcoma (the 'must-not-miss' diagnosis), 4. Giant Cell Tumor (unlikely due to open physis). Explicitly state that tissue diagnosis is required.
You have performed an MRI and the biopsy. The pathology shows blood-filled spaces with osteoclast-like giant cells and a USP6 gene rearrangement. The MRI shows fluid-fluid levels. What is your definitive diagnosis, and how do you plan the surgical approach?
Candidate: The diagnosis is a primary Aneurysmal Bone Cyst (ABC) confirmed by the USP6 rearrangement. I would plan a deltopectoral approach. I must ensure the previous biopsy tract is excised en bloc with the skin incision to prevent tumor seeding. The goal is extended curettage and internal fixation.
Failing to mention the biopsy tract excision—this is a critical 'surgical safety' point. Candidates often jump to fixation without detailing the 'extended' part of the curettage (burring + adjuvants), which is the standard of care to prevent recurrence.
Confirm the diagnosis is a primary ABC. The surgical plan must follow: 1. Deltopectoral approach with en-bloc excision of the biopsy tract. 2. Extended intralesional curettage (mechanical burring 2-3mm into healthy bone). 3. Adjuvants (Hydrogen peroxide or Argon beam) to address the reactive zone. 4. Reconstruction using a combination of cancellous allograft and injectable calcium phosphate cement. 5. Stable internal fixation using a locking plate with calcar screws to address the pathological fracture and prevent varus collapse.
The surgery went well. The lesion is filled with cement and bone graft, and stabilized with a PHILOS plate. What are your main concerns for postoperative rehabilitation and long-term follow-up?
Candidate: Rehabilitation involves early pendulum exercises while protecting against active motion during the initial phase. Long-term, I am concerned about local recurrence, so I will schedule serial radiographs every 3 months for the first two years.
Ignoring the "varus collapse" risk. Candidates often forget to mention the need for serial radiographic monitoring of the fixation construct itself, not just the tumor. They also fail to mention the transition from protected passive motion to full strengthening.
Structured rehabilitation: Phase 1 (Protection/Pendulums), Phase 2 (AAROM), Phase 3 (Strengthening/Return to function). Oncological surveillance: Standardized protocol (3-monthly for 2 years, then tapering). Mention specific risks: Local recurrence (mitigated by extended curettage), varus collapse of the proximal humerus, and the necessity of clearing the patient for contact sports only after radiographic union and strength recovery (>90% of contralateral).
