Orthopaedic Fracture & Soft-Tissue Classification Guide

Key Takeaway
Accurate fracture and soft-tissue classification is the cornerstone of orthopaedic traumatology. It dictates surgical decision-making, predicts prognostic outcomes, and standardizes academic communication. This guide comprehensively details the AO/OTA alphanumeric system, the Gustilo-Anderson criteria for open fractures, and the Tscherne classification, providing evidence-based frameworks for surgical approaches, fixation strategies, and postoperative protocols in complex musculoskeletal trauma.
Comprehensive Introduction and Patho-Epidemiology
In the realm of orthopaedic traumatology, the classification of fractures is far more than a mere academic exercise or a coding requirement; it is the foundational blueprint for surgical decision-making and patient prognostication. Historically, fractures were described using eponymous or purely descriptive terms that lacked the rigor necessary for standardized communication or scientific comparison. The evolution of modern orthopaedic surgery demanded a universal language. When combined with a rigorous assessment of the surgeon’s capabilities, institutional facilities, available resources, and the patient’s physiological profile, an accurate classification of the fracture and its associated soft-tissue envelope allows for the determination of the optimal treatment algorithm. This paradigm shift transformed orthopaedic trauma from a reactive discipline into a highly predictive, biomechanically driven science where the morphology of the osseous failure directly dictates the mechanical properties required of the chosen osteosynthesis construct.
The patho-epidemiology of fractures follows a distinctly bimodal distribution, reflecting two divergent mechanisms of injury and physiological baselines. The first peak occurs in young, predominantly male patients involved in high-energy trauma, such as motor vehicle collisions, falls from height, or ballistic injuries. These scenarios impart massive kinetic energy to the extremity, resulting in complex, multifragmentary fracture patterns (AO/OTA Type C) and devastating soft-tissue compromise. The second peak is observed in the elderly population, characterized by low-energy fragility fractures secondary to osteoporosis or osteopenia. In these osteoporotic fractures, the energy transfer is minimal, but the diminished structural integrity of the bone leads to characteristic failure patterns, such as proximal femur, distal radius, and proximal humerus fractures. Understanding this epidemiological dichotomy is critical, as the biological healing capacity and the mechanical holding power of implants differ vastly between dense, healthy cortical bone and osteoporotic, cavernous metaphyseal bone.
Fracture classification must also be contextualized within the patient's overall physiological state, particularly in the setting of polytrauma. The systemic inflammatory response to severe musculoskeletal injury is profound. Modern trauma algorithms recognize that the cumulative inflammatory burden—often termed the "second hit" phenomenon—of multiple long-bone fractures profoundly impacts the incidence of Acute Respiratory Distress Syndrome (ARDS) and Multi-Organ Failure (MOF). Injury severity scoring systems attempt to quantify the magnitude of multiple injuries to predict survival and guide the timing of orthopaedic interventions, specifically differentiating between candidates for Early Total Care (ETC) and Damage Control Orthopaedics (DCO). The Injury Severity Score (ISS) calculates severity based on the sum of the squares of the highest Abbreviated Injury Scale (AIS) scores in the three most severely injured body regions, with an ISS > 15 indicating major trauma and an ISS > 40 associated with high mortality.
Furthermore, physiological scoring systems like the Revised Trauma Score (RTS) and extremity-specific indices like the NISSSA Score (evaluating Nerve Injury, Ischemia, Soft-Tissue Injury, Skeletal Injury, Shock, and Age) provide highly predictive metrics for limb salvage versus primary amputation in severe lower extremity trauma. These scores often outperform the traditional Mangled Extremity Severity Score (MESS) by incorporating a more nuanced evaluation of the soft-tissue envelope and ischemic time. Ultimately, precise fracture and soft-tissue classification remains the critical first step in navigating the complex resuscitation and reconstruction of the polytraumatized patient, dictating not only the mechanics of the bone repair but the biological survival of the patient.
Detailed Surgical Anatomy and Biomechanics
Understanding the morphological characteristics of a fracture provides direct insight into the mechanism of injury, the energy dissipated through the limb, and the biomechanical forces required for stable osteosynthesis. The AO/OTA alphanumeric classification system remains the gold standard for diaphyseal and articular fracture classification. This system categorizes fractures based on morphological characteristics and precise anatomical location, utilizing a standardized grid that dictates the biomechanical environment. Type A fractures are simple (transverse, oblique, spiral) where the bone retains some load-sharing capacity once reduced. Type B fractures are wedge fractures (intact or fragmentary) where some cortical contact exists between the main proximal and distal fragments after reduction. Type C fractures are complex or multifragmentary, where no contact exists between the main proximal and distal fragments after reduction, meaning the implant must bear the entire mechanical load until bridging callus forms.
The biomechanics of these fracture patterns are intrinsically linked to Perren’s Strain Theory, which dictates the type of bone healing that will occur. Transverse fractures result from direct, high-energy bending forces and possess excellent compressive stability but poor torsional stability. Oblique fractures, resulting from combined bending and axial compression, are inherently unstable under axial loads and are prone to shortening and shear. Spiral fractures are caused by low-energy torsional forces; they often have a large surface area for healing but require neutralization of rotational forces during fixation. Comminuted and segmental fractures indicate massive high-energy transfer resulting in multiple fragments or isolated diaphyseal segments. In these Type C patterns, the application of absolute stability (interfragmentary compression) is mechanically impossible and biologically detrimental. Instead, relative stability constructs, such as intramedullary nails or bridge plates, must be utilized to preserve the soft-tissue envelope and stimulate secondary bone healing via endochondral ossification, maintaining strain levels between 2% and 10% to promote robust callus formation.
Just as the osseous injury must be meticulously classified, the associated soft-tissue envelope must be rigorously graded, as it is the primary determinant of infection risk, fracture union, and ultimate limb survival. The Gustilo-Anderson classification for open fractures provides critical prognostic information regarding the risk of deep infection and osteomyelitis based on wound size, degree of soft-tissue damage, periosteal stripping, and vascular compromise. Type I and II fractures represent lower-energy injuries with minimal to moderate soft-tissue damage.
Type IIIA injuries involve extensive soft-tissue lacerations or flaps but maintain adequate soft-tissue coverage of the fractured bone, inherently including all high-energy traumas, segmental fractures, or severely comminuted fractures regardless of the actual size of the skin wound.


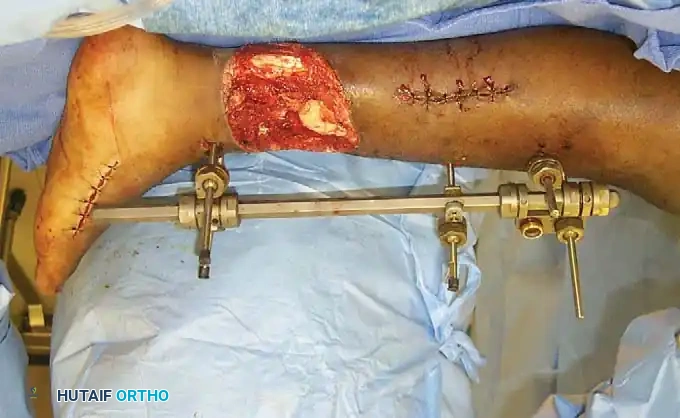
Type IIIB injuries are characterized by extensive soft-tissue loss with severe periosteal stripping and bony exposure, usually requiring a rotational or free muscle flap for coverage.

Type IIIC injuries denote any open fracture associated with an arterial injury requiring formal vascular repair for limb salvage.
Equally critical, yet frequently overlooked, is the Tscherne classification for closed fractures, which addresses the severity of soft-tissue injury in the absence of a skin breach. The Tscherne classification grades closed soft-tissue injuries from Grade 0 (minimal damage from indirect violence) to Grade 3 (extensive skin contusion, underlying muscle damage, subcutaneous avulsion or Morel-Lavallée lesions, and established compartment syndrome). The physiological status of the periosteal and endosteal blood supplies is entirely dependent on the integrity of this surrounding soft-tissue envelope. A Tscherne Grade 3 closed fracture often presents a higher risk for deep infection and delayed union following internal fixation than a Gustilo Type I open fracture, emphasizing that the "personality" of the fracture is dictated equally by the bone and the soft tissues.
Exhaustive Indications and Contraindications
The integration of fracture morphology (AO/OTA) and soft-tissue grading (Gustilo-Anderson/Tscherne) forms the basis for all indications and contraindications in operative fracture management. The primary decision matrix involves choosing between absolute stability (anatomical reduction and interfragmentary compression) and relative stability (functional reduction and flexible fixation). Absolute stability is strictly indicated for articular fractures (to prevent post-traumatic arthrosis) and simple diaphyseal fractures (AO Type A) where the bone can share the load with the implant. Techniques such as lag screw fixation combined with a neutralization plate are indicated here. Conversely, absolute stability is contraindicated in complex, multifragmentary diaphyseal fractures (AO Type C). Attempting anatomical reduction in these scenarios requires extensive periosteal stripping, which devascularizes the butterfly fragments, predictably leading to atrophic nonunion and catastrophic implant failure.
For complex, high-energy fractures (AO Type C), relative stability is universally indicated. The goal is to restore length, alignment, and rotation (LAR) while preserving the fracture hematoma and the biological potential of the soft-tissue envelope. Intramedullary nailing (IMN) is the gold standard for diaphyseal fractures of the femur and tibia, acting as a load-sharing, relative stability device that promotes robust secondary callus formation. When IMN is anatomically contraindicated (e.g., periarticular fractures, narrow medullary canals), Minimally Invasive Plate Osteosynthesis (MIPO) utilizing bridge plating techniques is indicated. The bridge plate acts as an extramedullary splint, bypassing the zone of comminution. The working length of the plate (the distance between the innermost screws) must be optimized to allow for flexible, elastic deformation of the construct under load, thereby stimulating callus formation without exceeding the fatigue limit of the titanium or stainless steel implant.
The soft-tissue envelope dictates the timing of these interventions, distinguishing between Early Total Care (ETC) and Damage Control Orthopaedics (DCO). ETC, involving immediate definitive internal fixation, is indicated for hemodynamically stable patients with isolated injuries or polytrauma patients who are adequately resuscitated (lactate < 2.5 mmol/L, normal coagulation profile) and present with Tscherne Grade 0-1 or Gustilo Type I-II injuries. DCO is strictly indicated for patients in extremis, those in the "borderline" physiological category, or those presenting with severe soft-tissue compromise (Gustilo IIIB/IIIC, Tscherne Grade 3). In DCO, immediate internal fixation is absolutely contraindicated due to the exorbitant risk of deep infection, wound breakdown, and physiological exhaustion ("second hit"). The indicated procedure is the rapid application of a spanning external fixator, aggressive serial debridements, and delayed definitive internal fixation only once the patient's physiology has normalized and the soft-tissue envelope has stabilized (evidenced by the resolution of edema and the appearance of the "wrinkle sign").
Table: Indications and Contraindications by Classification
| Fracture / Soft Tissue Classification | Primary Fixation Strategy | Indicated Techniques | Absolute Contraindications |
|---|---|---|---|
| AO Type A (Simple Diaphyseal) | Absolute or Relative Stability | Lag screw + Neutralization Plate, IM Nail | Bridge plating (risk of nonunion due to low strain) |
| AO Type C (Complex Diaphyseal) | Relative Stability (Biological) | Bridge Plating (MIPO), Locked IM Nail | Anatomical reduction with lag screws (devascularization) |
| Intra-articular (AO Type B/C) | Absolute Stability | Lag screws, Buttress plating, Anti-glide | Flexible fixation of the articular block (leads to arthritis) |
| Gustilo Type I / II | Early Total Care (ETC) | Immediate IM Nail or Plating | Prolonged external fixation (unnecessary risk of pin tract infection) |
| Gustilo Type IIIB / IIIC | Damage Control Orthopaedics | Spanning Ex-Fix, Serial Debridement, Flap | Immediate definitive internal plating (high infection risk) |
| Tscherne Grade 3 (Closed) | Damage Control Orthopaedics | Spanning Ex-Fix, Elevation | Immediate open reduction through compromised skin |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning is the most critical cognitive phase of fracture surgery, transforming the theoretical classification of the injury into a concrete, step-by-step surgical execution. This phase begins with obtaining high-quality, orthogonal radiographs of the entire involved bone, including the joints above and below the injury, to rule out contiguous fractures (e.g., a femoral neck fracture ipsilateral to a femoral shaft fracture). Digital templating is mandatory. For AO Type A fractures where absolute stability is planned, the surgeon must template the exact size of the lag screws, the length of the neutralization plate, and the precise trajectory of the drill bits. For AO Type C fractures requiring bridge plating, the surgeon must calculate the plate span ratio (plate length to fracture length, ideally > 3:1 in comminuted fractures) and the plate screw density (number of screws inserted divided by the number of plate holes, ideally < 0.5) to optimize the construct's stiffness and working length.
Incision planning is entirely dictated by the soft-tissue classification and the underlying angiosome anatomy. In the setting of high-energy trauma (Tscherne Grade 2 or 3), traditional extensile exposures are frequently contraindicated due to the risk of massive wound necrosis. Incisions must be meticulously planned to avoid zones of severe contusion, fracture blisters, or impending skin necrosis. The surgeon must utilize angiosome-sparing approaches, ensuring that full-thickness fasciocutaneous flaps are elevated without undermining the subcutaneous tissues, thereby preserving the delicate perforating vessels. For example, in a complex tibial plateau fracture with severe lateral soft-tissue compromise, a standard anterolateral approach may be abandoned in favor of a posterolateral or dual-incision technique to access the articular surface through pristine tissue corridors.
Patient positioning and operating room setup must account for the planned surgical approach, the need for intraoperative traction, and unimpeded fluoroscopic access. The patient must be positioned on a radiolucent table that allows the C-arm to obtain perfect anteroposterior and lateral views without moving the fractured extremity. For intramedullary nailing of the femur or tibia, the use of a fracture table with skeletal traction or a flat radiolucent table with a femoral distractor must be decided pre-operatively based on the fracture morphology and the presence of associated injuries (e.g., a fracture table is contraindicated in the presence of an unstable pelvic ring injury). The C-arm must be positioned to visualize the joint above and below the fracture seamlessly. Meticulous attention to padding all bony prominences is required to prevent iatrogenic nerve palsies, particularly the common peroneal nerve at the fibular neck and the ulnar nerve at the cubital tunnel, during prolonged reconstructive procedures.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of fracture repair is a highly choreographed sequence that must adhere strictly to the biomechanical and biological principles dictated by the fracture's classification. In the setting of open fractures (Gustilo-Anderson Types I-IIIC), the procedure invariably begins with a radical, systematic debridement. The traumatic wound must be extended longitudinally to allow full visualization of the zone of injury. Debridement proceeds from superficial to deep: skin, subcutaneous fat, fascia, muscle, and finally, bone. Muscle viability is rigorously assessed using the "4 C's": Color (red vs. dark/dusky), Consistency (firm vs. friable), Contractility (response to electrocautery or forceps pinch), and Capacity to bleed. Any devitalized cortical bone devoid of soft-tissue attachment must be meticulously excised, as it serves as a nidus for biofilm formation and deep infection. Copious low-pressure irrigation with normal saline follows the debridement to reduce the bacterial load mechanically.
Reduction techniques are fundamentally altered based on the AO/OTA classification. For Type A fractures undergoing absolute stability, direct reduction techniques are employed. The fracture ends are anatomically keyed together using reduction forceps (e.g., Weber clamps). A lag screw is then placed across the fracture plane to generate static interfragmentary compression, obliterating the fracture gap and preventing micro-motion. This construct is subsequently protected by a neutralization plate, which resists torsional, bending, and shear forces that would otherwise cause the lag screw to fail. This technique demands precise contouring of the plate to the osseous anatomy to prevent displacement of the reduction when the plate is compressed against the bone.
Conversely, for Type C multifragmentary fractures, indirect reduction techniques are mandatory. The goal is to restore Length, Alignment, and Rotation (LAR) without disturbing the fracture hematoma or stripping the remaining periosteal attachments of the comminuted fragments. Tools such as a femoral distractor, skeletal traction pins, or percutaneous reduction clamps (joysticks) are utilized to align the proximal and distal main fragments. Once LAR is restored, a bridge plate is slid submuscularly across the comminuted zone (MIPO technique) or an intramedullary nail is passed down the canal. When utilizing a bridge plate, the surgeon must ensure an adequate working length, typically leaving 2 to 3 plate holes empty directly over the fracture site. This deliberate omission of screws decreases the stiffness of the construct, allowing for symmetrical elastic micro-motion at the fracture site under physiological loading, which is the potent mechanical stimulus necessary for the formation of robust enchondral bridging callus.
Complications, Incidence Rates, and Salvage Management
Despite meticulous adherence to classification-based treatment algorithms, orthopaedic trauma surgery is fraught with severe complications, largely driven by the initial energy of the injury and the severity of the soft-tissue compromise. Infection remains the most devastating complication, with incidence rates directly correlating to the Gustilo-Anderson classification. While Gustilo Type I fractures have an infection rate of approximately 0-2%, Type IIIB and IIIC fractures exhibit deep infection rates ranging from 10% to over 50%, depending on the timing of soft-tissue coverage and the adequacy of the initial debridement. Biofilm-forming organisms, particularly Staphylococcus aureus and Pseudomonas aeruginosa, adhere to necrotic bone and orthopaedic implants, rendering systemic antibiotics ineffective. Management of established deep infection requires aggressive surgical intervention, including complete hardware removal, radical resection of all infected and necrotic bone (creating a critical-sized defect), and the placement of antibiotic-impregnated polymethylmethacrylate (PMMA) spacers.
Nonunion and malunion are frequent mechanical and biological complications, particularly in AO Type C fractures and segmental bone loss scenarios. Atrophic nonunion occurs when the biological environment is compromised—often due to excessive iatrogenic periosteal stripping during surgery or severe initial soft-tissue trauma—resulting in a lack of callus formation. Hypertrophic nonunion, conversely, is a mechanical failure characterized by abundant callus ("elephant foot" appearance) that fails to bridge the fracture gap due to excessive strain (instability) in the fixation construct. Salvage of atrophic nonunion requires biological augmentation, typically through autologous bone grafting (e.g., iliac crest bone graft) and optimization of the mechanical environment. Hypertrophic nonunions are treated primarily by increasing the stability of the construct, such as exchanging an intramedullary nail for a larger diameter nail to reduce micro-motion.
For critical-sized bone defects resulting from severe trauma (e.g., Gustilo IIIB with bone loss) or radical debridement for osteomyelitis, advanced reconstructive salvage techniques are required. The Masquelet induced-membrane technique is a two-stage procedure: the first stage involves placing a PMMA cement spacer into the defect to induce a biologically active, vascularized pseudomembrane; the second stage, performed 6-8 weeks later, involves removing the spacer and packing the membrane-lined void with massive autologous cancellous bone graft. Alternatively, distraction osteogenesis utilizing an Ilizarov circular external fixator allows for bone transport, gradually moving a healthy segment of bone across the defect at a rate of 1 mm per day, generating new bone in its wake. When these heroic limb-salvage efforts fail, or when the limb is insensate and non-functional, secondary amputation remains a definitive and necessary salvage option to restore the patient's overall mobility and quality of life.
Table: Complication Rates and Salvage Strategies by Classification
| Injury Classification | Primary Complication Risk | Estimated Incidence | Salvage Strategy / Management |
|---|---|---|---|
| Gustilo Type I / II | Superficial Infection | 1 - 5% | Oral/IV Antibiotics, Local wound care |
| Gustilo Type IIIB / IIIC | Deep Infection / Osteomyelitis | 10 - 50% | Hardware removal, Radical debridement, PMMA spacer, Flap |
| AO Type A (Simple) | Hypertrophic Nonunion (if poorly fixed) | 2 - 5% | Revision fixation (increase stability), Exchange nailing |
| AO Type C (Comminuted) | Atrophic Nonunion / Hardware Failure | 10 - 20% | Autologous bone grafting, Revision plating/nailing |
| Critical Bone Loss (>3cm) | Segmental Defect | N/A | Masquelet technique, Ilizarov bone transport, Vascularized fibula |
| Tscherne Grade 3 | Compartment Syndrome | 5 - 15% | Emergent 4-compartment fasciotomy, Delayed closure |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation protocol is not a generic, one-size-fits-all prescription; it must be meticulously tailored to the specific fracture classification, the chosen method of osteosynthesis (absolute vs. relative stability), and the status of the soft-tissue envelope. The rehabilitation process is generally divided into three distinct, biologically driven phases: Phase 1 (Protection and Tissue Healing), Phase 2 (Early Mobilization and Callus Formation), and Phase 3 (Strengthening and Full Weight-Bearing). Communication between the orthopaedic surgeon and the physical therapy team is paramount, as premature loading of a relative stability construct can lead to catastrophic hardware failure, while prolonged immobilization of an articular fracture guarantees severe post-traumatic stiffness and arthrofibrosis.
Phase 1 (Weeks 0-2) focuses entirely on wound healing, edema control, and the prevention of deep vein thrombosis (DVT). For severe soft-tissue injuries (Gustilo IIIB/C, Tscherne Grade 3), wound management is the primary concern. Wounds may require negative pressure wound therapy (NPWT) and strict elevation. Joint immobilization in a neutral position via splinting may be necessary to protect vascular repairs or rotational flaps. Weight-bearing is strictly prohibited for lower extremity injuries in this phase to prevent shear forces across the healing soft-tissue envelope. However, for isolated, simple diaphyseal fractures (AO Type A) treated with a statically locked intramedullary nail, immediate weight-bearing as tolerated may be initiated, as the robust titanium implant acts as a load-sharing device that can withstand physiological forces while the bone heals.
Phase 2 (Weeks 2-6) marks the transition to early mobilization and the initiation of the biological healing cascade. For fractures treated with absolute stability (lag screws and plates), the goal of fixation is to allow immediate, active range of motion (ROM) of the adjacent joints to nourish the articular cartilage and prevent capsular contracture. However, because these constructs rely on primary bone healing (direct Haversian remodeling without a callus), the fracture site cannot tolerate significant mechanical loading. Therefore, weight-bearing is typically restricted (e.g., touch-down weight-bearing only) until radiographic evidence of obliteration of the fracture line is observed. Conversely, for fractures treated with relative stability (bridge plates or IM nails), controlled micro-motion is actively encouraged to stimulate bridging callus formation. ROM exercises are advanced, but full weight-bearing may still be restricted depending on the degree of comminution (AO Type C) to prevent fatigue failure of the implant before the biological callus can share the load.
Phase 3 (Weeks 6-12+) focuses on progressive mechanical loading, muscle hypertrophy, and return to pre-injury function. The transition to full weight-bearing in complex fractures is dictated by radiographic progression. The surgeon assesses orthogonal radiographs for the presence of bridging callus on at least three of the four visible cortices (anterior, posterior, medial, lateral). Once bridging callus is confirmed, the construct transitions from load-bearing to load-sharing, and progressive resistance training is initiated. Gait training, proprioceptive recovery, and functional kinetic chain exercises are emphasized. In cases of delayed union, the surgeon may intervene during this phase by dynamically locking an intramedullary nail (removing the static locking screws) to allow for controlled axial dynamization, thereby increasing the mechanical strain at the fracture site to jump-start a stalled healing response.
Summary of Landmark Literature and Clinical Guidelines
The modern algorithms for fracture and soft-tissue classification, and their subsequent surgical applications, are not arbitrary; they are the culmination of decades of rigorous, peer-reviewed traumatology research. A comprehensive understanding of this landmark literature is essential for any academic orthopaedic surgeon, as it provides the evidence-based foundation for the clinical guidelines utilized in daily practice. The seminal work by Gustilo and Anderson, originally published in 1976 and subsequently modified in 1984 based on a profound review of 1,025 open fractures, remains the bedrock of open fracture management. Their research definitively correlated the extent of soft-tissue damage and periosteal stripping with the exponential rise in deep infection rates. This classification system directly birthed the current clinical guidelines mandating emergent systemic antibiotic prophylaxis (first-generation cephalosporins for Type I/II, with the addition of aminoglycosides for Type III) and the necessity of radical surgical debridement.
The AO (Arbeitsgemeinschaft für Osteosynthesefragen) alphanumeric classification, spearheaded by Müller et al., revolutionized the mechanical approach to fracture care. By creating a standardized, morphologically precise grid based on data from the AO Documentation Center, this system allowed for the global standardization of osteosynthesis techniques. The clinical validity of the AO/OTA system was rigorously evaluated by Swiontkowski et al., who demonstrated that the system accurately predicts functional outcomes and impairment levels. Specifically, their research validated that patients with multifragmentary Type C fractures exhibit significantly worse long-term functional performance compared to those with simpler Type A or B fractures, thereby justifying the use of more advanced, biologically preserving surgical techniques (like MIPO) for these complex injury patterns to mitigate poor outcomes.
Finally, the management of severe lower extremity trauma and the decision-making process between limb salvage and primary amputation have been fundamentally shaped by the Lower Extremity Assessment Project (LEAP) study. This landmark, multi-center prospective trial evaluated patients with severe, limb-threatening injuries (Gustilo IIIB and IIIC). The LEAP study critically challenged the historical reliance on scoring systems like the MESS, demonstrating that no single scoring system could accurately predict the necessity of amputation with 100% specificity. Furthermore, the study revealed that at two and seven years post-injury, there was no significant difference in functional outcomes or quality of life between patients who underwent successful limb salvage and those who underwent early amputation and prosthetic fitting. These findings cemented the current clinical guidelines that emphasize a multidisciplinary approach, shared decision-making with the patient, and the recognition that a well-executed amputation is a reconstructive procedure, not a failure of treatment, particularly when the soft-tissue envelope and neurovascular structures are irreparably destroyed.
