Diagnosis of Fractures: Essential Steps for Effective Treatment

Key Takeaway
This topic focuses on Diagnosis of Fractures: Essential Steps for Effective Treatment, The diagnosis of fractures primarily relies on mandatory radiographic examination, including anteroposterior and lateral views of the suspected area and adjacent joints. Clinical signs such as palpable sharp edges or localized edema can indicate a fracture, especially for hairline or stress fractures. Proper imaging, with specific requests detailing the affected bone, ensures accurate diagnosis and guides treatment.
Introduction and Epidemiology
Fractures represent a fundamental pathology within orthopedic surgery, requiring a rigorous, systematic approach to diagnosis and management. The epidemiology of fractures typically follows a bimodal distribution. High-energy trauma, such as motor vehicle collisions and falls from height, predominantly affects young males, resulting in complex, multi-fragmentary, or open fractures. Conversely, low-energy fragility fractures are primarily observed in the elderly population, particularly post-menopausal females, secondary to osteoporotic bone density changes.
The initial evaluation of any fracture, particularly in the trauma setting, must adhere to Advanced Trauma Life Support protocols to rule out life-threatening injuries before focusing on isolated musculoskeletal pathology. The diagnostic algorithm relies heavily on a meticulous clinical examination coupled with precise radiographic imaging. Accurate diagnosis is not merely the identification of a cortical breach; it encompasses the assessment of the soft tissue envelope, neurovascular status, and the biomechanical personality of the fracture. This comprehensive evaluation dictates the subsequent treatment cascade, distinguishing between injuries amenable to conservative casting and those necessitating complex operative intervention.
Surgical Anatomy and Biomechanics
A profound understanding of osteology, vascular anatomy, and biomechanics is prerequisite for effective fracture management. Bone is a dynamic, anisotropic composite material, exhibiting different mechanical properties depending on the direction of the applied load. Cortical bone, found primarily in the diaphysis of long bones, is dense and withstands high compressive and torsional forces but is vulnerable to tension and shear. Cancellous bone, located in the metaphyses and epiphyses, is highly porous and trabecular, optimized for energy dissipation and load transfer across articulations.
The vascular supply to long bones is dual-sourced, comprising the intramedullary nutrient artery system and the periosteal vascular network. The nutrient artery supplies the inner two-thirds of the cortex, while the periosteal vessels supply the outer one-third. Disruption of this vascular architecture during trauma or iatrogenically during surgical exposure significantly impairs the biological potential for fracture healing. Surgical approaches must respect angiosomes and utilize internervous planes to minimize collateral damage to the soft tissue envelope, which is critical for periosteal perfusion.
Biomechanically, fracture healing is dictated by the mechanical environment at the fracture site, specifically the interfragmentary strain. According to Perren’s strain theory, primary bone healing (direct Haversian remodeling without callus formation) requires absolute stability, defined as interfragmentary strain of less than 2%. This is typically achieved through anatomical reduction and interfragmentary compression using lag screws and neutralization plates. Secondary bone healing involves endochondral ossification and callus formation, which is stimulated by relative stability (strain between 2% and 10%). Intramedullary nailing, bridge plating, and external fixation provide relative stability, promoting robust callus formation while preserving the fracture hematoma.
Indications and Contraindications
The decision to proceed with operative versus non-operative management is multifactorial, depending on patient-specific variables (age, comorbidities, functional demands), fracture characteristics (displacement, comminution, articular involvement), and soft tissue integrity.
Operative Versus Non Operative Management
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Absolute Indications | Open fractures (Gustilo-Anderson I-III); Neurovascular compromise; Compartment syndrome; Polytrauma requiring early mobilization. | Undisplaced, stable fractures; Unacceptable surgical risk (severe medical comorbidities); Non-ambulatory baseline status (in specific lower extremity fractures). |
| Relative Indications | Displaced intra-articular fractures (>2mm step-off); Failure of conservative management; Unacceptable axial or rotational malalignment; Floating joint injuries. | Minimally displaced extra-articular fractures; Pediatric fractures with high remodeling potential; Fractures with acceptable alignment per established parameters. |
| Contraindications | Active systemic or local infection (for internal fixation); Severe soft tissue compromise prohibiting safe incision (e.g., massive fracture blisters); Terminal illness with short life expectancy. | Unstable fracture patterns prone to progressive deformity; Intra-articular step-offs predisposing to post-traumatic osteoarthritis. |
Pre Operative Planning and Patient Positioning
Pre-operative planning begins at the moment of initial patient contact and represents the synthesis of clinical examination and radiographic evaluation. A meticulously planned procedure minimizes intra-operative complications, reduces tourniquet and operative time, and optimizes functional outcomes.
Clinical Evaluation
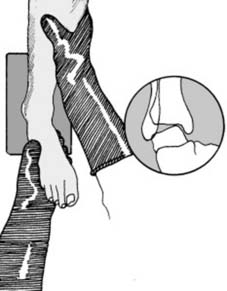
The clinical diagnosis of a fracture mandates a structured physical examination, emphasizing inspection, palpation, and assessment of the neurovascular status distal to the injury.

The sharp edge of a fracture may be palpable beneath the subcutaneous tissues. Note also the presence of localized edema. This is a particularly useful sign over hair-line and stress fractures, where initial radiographic findings may be subtle or absent. The development of edema may, however, take some hours to reach detectable proportions, necessitating serial examinations in occult injuries.

If the fracture is mobile, moving the part may produce angulation or crepitus from the bone ends rubbing together. In addition, the patient will experience severe pain from such movement. These signs may be inadvertently observed during routine examination of the patient, but should not be actively sought unless the patient is unconscious and the diagnosis is in doubt. Eliciting crepitus intentionally causes unnecessary pain and risks further iatrogenic injury to the surrounding neurovascular structures and periosteum.
Radiographic Examination
In every case of suspected fracture, radiographic examination of the fracture is mandatory. Radiographs of the part will generally give a clear indication of the presence of a fracture and provide a sound basis for templating and planning surgical treatment. In the case where there is some clinical doubt, radiographs will reassure both patient and surgeon and avert any later medicolegal criticism.
Radiographers receive thorough training in the techniques for the satisfactory visualization of any suspect area, but it is essential that they in turn are given clear guidance as to the area under suspicion. The request form must be quite specific, otherwise critical diagnostic mistakes may occur. At its simplest, the request must state both the area to be visualized and the bone suspected of being fractured. It is highly desirable to include the joints above and below the fracture to rule out concomitant injuries. It need hardly be stressed that a thorough clinical examination should precede the completion of the radiographic request if repetition and the taking of unnecessary films are to be avoided.
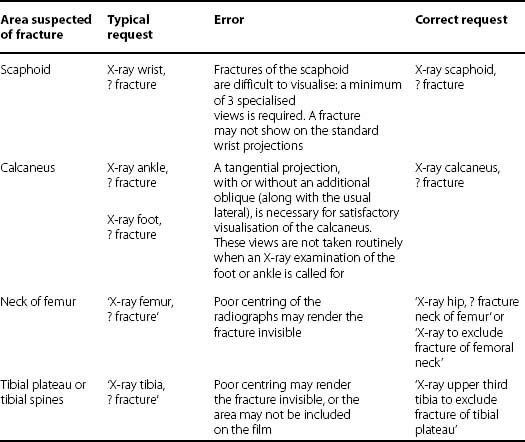
The following table lists some of the commonest errors made in the filling in of radiographic request forms:
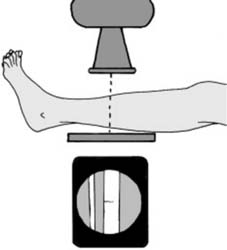
Standard Projections
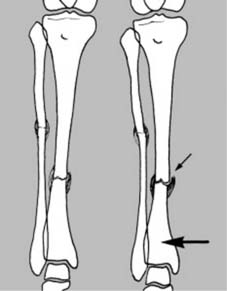
The cornerstone of orthopedic imaging relies on orthogonal views. These are standard anteroposterior and lateral projections. Ideally, the X-ray beam should be centered over the area of suspected fracture, with visualization of the proximal and distal joints.

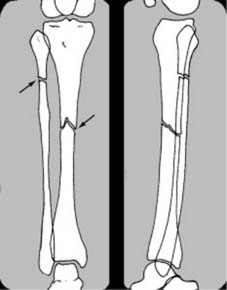
This rule is especially important in the paired long bones where, for example, a fracture of the tibia at one level may be accompanied by a fibular fracture at another level, or a radius fracture may be associated with a distal radioulnar joint dislocation (Galeazzi fracture-dislocation).
Comparison Films
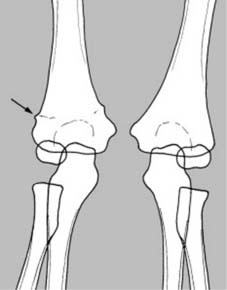
Where there is some difficulty in interpreting the radiographs, comparison films of the contralateral, uninjured side should be taken for direct comparison. This is particularly crucial in the elbow region in pediatric patients where the epiphyseal structures (capitellum, radial head, internal epicondyle, trochlea, olecranon, external epicondyle) are continually changing and ossifying at different ages, or where there is some unexplained shadow or a suspected congenital abnormality.
Oblique Projections and Advanced Imaging
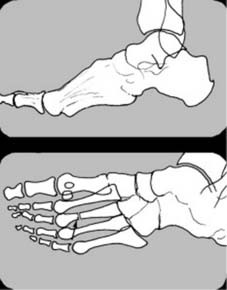
In the case of the hand and foot, an oblique projection may be highly helpful when the lateral view gives rise to confusion due to the superimposition of multiple metacarpal or metatarsal shafts.
When standard and oblique plain radiographs are insufficient to delineate complex intra-articular fracture patterns, cross-sectional imaging is required. Computed Tomography with sagittal, coronal, and 3D reconstructions is the gold standard for evaluating articular comminution, impaction, and spatial orientation of fracture fragments, which is critical for pre-operative templating.
Patient Positioning and Operating Room Setup
Proper patient positioning is as critical as the surgical approach itself. The positioning must allow for adequate surgical exposure, unhindered access for intra-operative fluoroscopy (C-arm), and the ability to manipulate the limb for fracture reduction. Radiolucent tables or specialized fracture tables are frequently utilized. For instance, in the management of femoral shaft fractures utilizing an antegrade intramedullary nail, the patient may be positioned supine on a fracture table with the injured limb in traction and the contralateral limb scissored to allow lateral fluoroscopic imaging of the proximal femur. Pressure points must be meticulously padded to prevent iatrogenic neuropathies, and a surgical safety checklist must be completed prior to incision.
Detailed Surgical Approach and Technique
The surgical management of fractures must adhere to the foundational principles established by the AO Foundation: anatomical reduction (particularly for intra-articular fractures), stable internal fixation, preservation of blood supply, and early, active, pain-free mobilization.
Incision and Dissection
Surgical approaches must be carefully planned to utilize internervous planes, thereby avoiding denervation of the surrounding musculature. For example, the anterior (Henry) approach to the radius exploits the internervous plane between the brachioradialis (radial nerve) and the pronator teres/flexor carpi radialis (median nerve). Incisions should be longitudinal and incorporate previous surgical scars when possible, maintaining broad skin bridges to prevent necrosis.
Soft tissue handling must be atraumatic. The periosteum should only be elevated precisely where the implant will interface with the bone, minimizing stripping to preserve the periosteal blood supply. In cases of severe soft tissue injury, minimally invasive plate osteosynthesis techniques should be employed to slide plates submuscularly, bridging the fracture zone without direct exposure.
Reduction Techniques
Fracture reduction can be achieved via direct or indirect methods. Direct reduction involves exposing the fracture site and manipulating the fragments using reduction forceps, dental picks, or elevators. This is essential for intra-articular fractures where anatomical restoration of the joint surface is paramount to prevent post-traumatic osteoarthritis.
Indirect reduction relies on ligamentotaxis and traction to align the fracture fragments without exposing the fracture hematoma. This technique is highly favored in diaphyseal and metaphyseal comminuted fractures. Instruments such as a femoral distractor, external fixator, or skeletal traction pins are utilized to restore length, alignment, and rotation.
Fixation Methods
The choice of fixation is dictated by the required biomechanical stability.
- Lag Screw and Neutralization Plating: Used for simple fracture patterns (e.g., oblique or spiral). A lag screw achieves interfragmentary compression, providing absolute stability. A plate is then applied to neutralize bending, shear, and torsional forces that would otherwise cause the lag screw to fail.
- Bridge Plating: Utilized for comminuted diaphyseal or metaphyseal fractures. The plate spans the zone of comminution, fixed only to the proximal and distal intact bone segments. This provides relative stability, preserving the fracture biology and promoting secondary bone healing via callus formation.
- Intramedullary Nailing: The gold standard for most diaphyseal fractures of the femur and tibia. It acts as a load-sharing device, providing excellent resistance to bending while allowing axial micromotion, which stimulates callus formation. Reaming the canal increases the contact area for the nail and provides an autogenous bone graft to the fracture site, though it temporarily disrupts endosteal blood supply.
- External Fixation: Often deployed in the acute trauma setting for damage control orthopedics, particularly in open fractures with severe soft tissue contamination or in polytrauma patients requiring rapid stabilization. It allows for soft tissue resuscitation while maintaining fracture alignment, later to be converted to definitive internal fixation.
Complications and Management
Orthopedic trauma surgery carries inherent risks. Anticipation, early recognition, and aggressive management of complications are vital for limb salvage and functional recovery.
Common Complications and Salvage Strategies
| Complication | Incidence / Risk Factors | Clinical Presentation | Management and Salvage Strategies |
|---|---|---|---|
| Acute Compartment Syndrome | High-energy tibial shaft fractures, crush injuries. | Pain out of proportion, pain with passive stretch, tense compartments, paresthesia. | Emergent four-compartment fasciotomy. Delayed primary closure or split-thickness skin grafting once swelling subsides. |
| Fracture-Related Infection | Open fractures, prolonged operative time, diabetes, smoking. | Erythema, purulent drainage, increasing pain, elevated CRP/ESR, radiographic loosening of hardware. | Aggressive surgical debridement, hardware removal if unstable or fracture healed, retention if stable and acute. Culture-directed IV antibiotics. Potential staged reconstruction with antibiotic spacers. |
| Nonunion | Smoking, NSAID use, inadequate fixation (mechanical), poor blood supply (biological). | Persistent pain at fracture site >6 months, absence of bridging callus on radiographs, hardware failure. | Hypertrophic: Improve mechanical stability (e.g., exchange nailing, compression plating). Atrophic: Improve biology (autologous bone grafting, decortication, BMPs) and optimize stability. |
| Malunion | Inadequate intra-operative reduction, premature weight-bearing, subsidence. | Visible deformity, limb length discrepancy, altered joint mechanics. | Corrective osteotomy (opening wedge, closing wedge, or dome) with rigid internal fixation to restore mechanical axis and joint orientation. |
| Post-Traumatic Osteoarthritis | Intra-articular fractures with >2mm step-off, chondral injury at impact. | Progressive joint pain, stiffness, radiographic joint space narrowing, osteophytes. | Conservative management initially (NSAIDs, injections, bracing). Surgical salvage includes joint arthrodesis or total joint arthroplasty depending on patient age and joint involved. |
Post Operative Rehabilitation Protocols
Rehabilitation is an integral component of the surgical prescription, requiring close collaboration between the orthopedic surgeon and physical therapy team. Protocols are phased and tailored to the specific fracture pattern, fixation rigidity, and soft tissue healing timelines.
Phase 1 Immediate Post Operative
The primary goals in the first 0 to 14 days are protection of the surgical repair, edema control, and prevention of deep vein thrombosis. The limb is often immobilized in a splint or brace. Cryotherapy and elevation are strictly enforced. Passive range of motion of the adjacent, uninvolved joints is initiated to prevent stiffness. Weight-bearing status is heavily dependent on the injury; intra-articular fractures typically require strict non-weight-bearing status, whereas diaphyseal fractures treated with intramedullary nailing may allow for immediate weight-bearing as tolerated.
Phase 2 Early Motion and Tissue Healing
From 2 to 6 weeks, soft tissue healing progresses, and early soft callus begins to form. Sutures or staples are removed. The focus shifts to restoring active and active-assisted range of motion of the involved joints. Bracing may be transitioned to a functional orthosis. In lower extremity injuries, progressive partial weight-bearing may be initiated under radiographic guidance, utilizing assistive devices.
Phase 3 Strengthening and Proprioception
Between 6 and 12 weeks, hard callus formation is typically visible on radiographs, providing sufficient stability to withstand physiological loads. Rehabilitation intensifies to include progressive resistance exercises, closed kinetic chain activities, and proprioceptive training. Full weight-bearing is usually achieved during this phase.
Phase 4 Return to Function
Beyond 12 weeks, remodeling of the woven bone into lamellar bone continues. The objective is to return the patient to their pre-injury level of occupational and athletic activity. Advanced functional drills, plyometrics, and work-hardening programs are implemented. The hardware is generally left in situ unless it causes symptomatic soft tissue irritation, in which case elective removal may be considered after complete radiographic consolidation (typically >12-18 months post-operatively).
Summary of Key Literature and Guidelines
Evidence-based practice dictates that fracture management aligns with established national and international guidelines.
The AO Foundation's Principles of Fracture Management remains the definitive text guiding the biomechanical and biological rationale for internal fixation. Their classification system provides a universal language for describing fracture morphology and guiding treatment algorithms.
For open fractures, the Gustilo-Anderson classification system remains the standard for categorizing soft tissue injury severity and dictating antibiotic prophylaxis and surgical timing. Literature supports the administration of intravenous antibiotics within one hour of injury and urgent, thorough surgical debridement to mitigate infection risks.
In the United Kingdom, the British Orthopaedic Association Standards for Trauma provide rigorous, evidence-based guidelines for the management of specific injuries, such as severe open lower limb fractures. These guidelines emphasize the necessity of a multidisciplinary approach, requiring combined orthoplastic surgical teams for definitive soft tissue coverage and skeletal stabilization within 72 hours of injury, significantly reducing the rates of deep infection and amputation.
Adherence to these academic principles, combined with meticulous clinical and radiographic evaluation, ensures the highest standard of care in the surgical management of fractures.
