The Critical Significance of Hairline Fractures: Don't Overlook Them
Key Takeaway
Here are the crucial details you must know about The Critical Significance of Hairline Fractures: Don't Overlook Them. The significance hairline fractures lies in their subtle nature, often caused by minimal trauma insufficient to cause significant fragment displacement. These fractures can be challenging to detect on initial radiographs, sometimes requiring repeat films, CT, MRI, or bone scans. While generally healing rapidly with symptomatic treatment, the scaphoid and femoral neck are notable exceptions requiring careful management.
The Critical Significance of Hairline Fractures Don't Overlook Them
As orthopedic surgeons, residents, and medical students, our diagnostic acuity and treatment paradigms are continually refined by our understanding of fracture patterns. Among the diverse spectrum of bony disruptions, hairline fractures frequently present a unique diagnostic and management challenge. These subtle injuries, often resulting from minimal trauma and initially lacking overt radiographic evidence, possess a critical significance that, if overlooked, can lead to substantial morbidity. This comprehensive review aims to underscore the diagnostic pitfalls, biomechanical implications, and management strategies associated with hairline fractures, emphasizing their importance in contemporary orthopedic practice.
Introduction and Epidemiology
Hairline fractures represent a unique category of skeletal injury, defined primarily by the minimal trauma required to produce them and the absence of significant fragment displacement. These fractures can be either incomplete, involving only a portion of the bone cortex, or complete, traversing the entire bone but without displacement of the fragments. Their insidious nature stems from the often-benign initial presentation coupled with diagnostic challenges on conventional radiography.
The epidemiology of hairline fractures is broad, affecting individuals across all age groups and activity levels, though certain populations are at higher risk. Athletes, particularly those engaged in repetitive impact sports such as running, basketball, or gymnastics, frequently develop stress fractures, which are a common subtype of hairline fracture. These occur when chronic, repetitive microtrauma exceeds the bone's remodeling capacity, leading to a fatigue-induced failure. Conversely, older adults or individuals with compromised bone quality, such as those with osteoporosis or osteomalacia, are susceptible to insufficiency fractures from normal physiological loading. Pathological fractures, where a pre-existing bone lesion (e.g., a simple bone cyst, metastatic disease) weakens the bone matrix, can also present as hairline patterns.
Understanding Fracture Patterns and Significance
Hairline fractures result from forces just sufficient to disrupt bone integrity without causing macroscopic displacement. This delicate balance of trauma and structural resistance makes them elusive. The initial presentation might involve localized pain, swelling, and tenderness, often out of proportion to the seemingly minor inciting event. A key differentiator is the lack of immediate instability or gross deformity typical of more severe fractures. Recognizing the potential for significant long-term sequelae, including non-union, progression to displaced fractures, or avascular necrosis, necessitates a high index of suspicion.
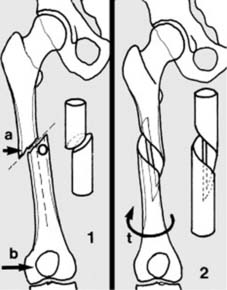
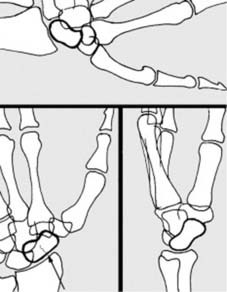
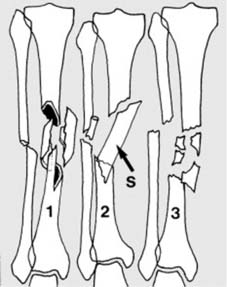
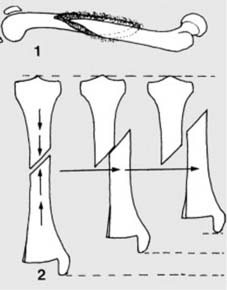
Hairline fractures result from minimal trauma, i.e., trauma which is just great enough to produce a fracture but not severe enough to produce any significant displacement of the fragments. Such fractures may be (1) incomplete or (2) complete.
Pathological Fractures and Differential Diagnosis
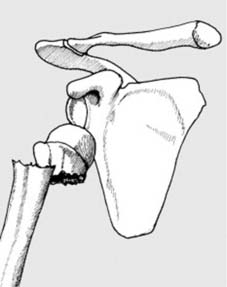
It is imperative to distinguish primary traumatic hairline fractures from those that are pathological in nature. Pathological fractures occur through bone that has been structurally compromised by a pre-existing disease process.

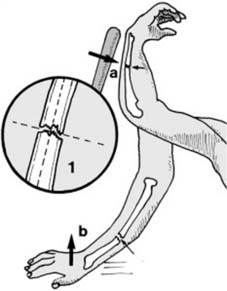
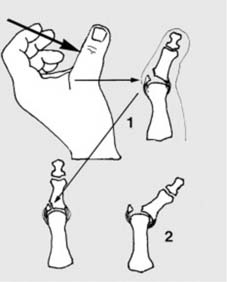
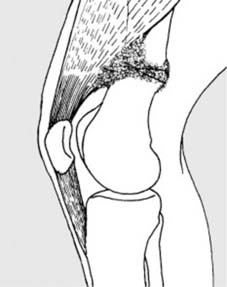
Pathological fractures may also occur at the site of simple tumours, e.g. a fracture of the humerus (a) in a child with a simple bone cyst (b). The commonest causes of pathological fracture are osteoporosis and osteomalacia.
The commonest causes of pathological fracture are osteoporosis and osteomalacia, which reduce bone mineral density and architectural integrity. Other causes include benign tumors (e.g., simple bone cysts, fibrous dysplasia), malignant primary bone tumors, or metastatic disease. A hairline fracture in a long bone, particularly in a younger patient without a significant history of trauma, should prompt a thorough investigation for underlying pathological processes. This includes a detailed medical history, family history, and potentially laboratory studies for metabolic bone disease or oncologic screening. The clinical presentation of a pathological hairline fracture may be indistinguishable from a traumatic one, underscoring the importance of vigilance.
Stress Fractures as a Hairline Subtype
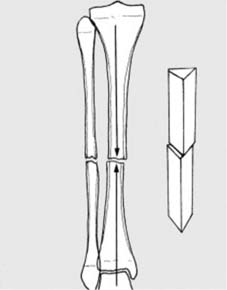
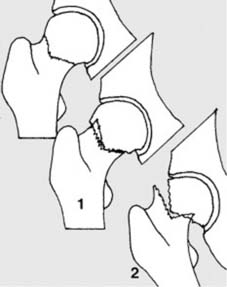
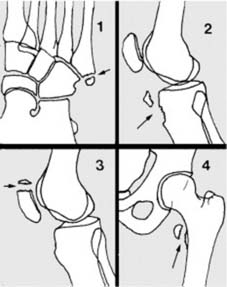
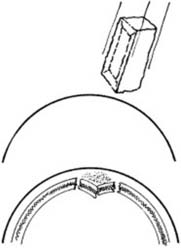
Stress fractures are inherently hairline in pattern, representing a failure of normal bone subjected to abnormal, repetitive stress, or abnormal bone subjected to normal stress.
Stress fractures are generally hair-line in pattern.
These can be further categorized into fatigue fractures (normal bone, abnormal stress) and insufficiency fractures (abnormal bone, normal stress). Common sites include the tibia, fibula, metatarsals, navicular, and femoral neck. The identification of a stress fracture is crucial, as delayed diagnosis can lead to complete fracture displacement, chronic pain, non-union, or even avascular necrosis, particularly in high-risk locations such as the femoral neck or scaphoid.
Surgical Anatomy and Biomechanics
A thorough understanding of bone anatomy and the biomechanical principles governing fracture propagation is fundamental to appreciating the significance of hairline fractures. The bone matrix, a complex composite of collagen and hydroxyapatite, is exquisitely adapted to resist various mechanical stresses, yet it has finite limits.
Bone Structure and Microtrauma
Bone is a dynamic tissue constantly undergoing remodeling through the coupled actions of osteoblasts and osteoclasts. This process allows bone to adapt to mechanical loads (Wolff's Law). Hairline fractures often initiate as microfractures within the trabecular or cortical bone, representing a failure of this remodeling capacity to keep pace with repetitive stress. Cortical bone, dense and compact, is primarily responsible for resisting bending and torsional forces, while cancellous (trabecular) bone, with its porous, spongy architecture, is crucial for resisting compressive forces and dissipating energy.
Biomechanical Factors in Fracture Genesis
The development of a hairline fracture is influenced by several biomechanical factors:
1. Loading Magnitude and Frequency: Repetitive submaximal loads can accumulate over time, leading to material fatigue even if individual loads are well within the bone's elastic limits. High-frequency loading, common in athletes, leaves insufficient time for complete bone remodeling cycles.
2. Load Distribution: Uneven load distribution can create stress risers, localizing stress in particular areas, such as the tension side of a long bone during bending or areas of abrupt change in bone geometry.
3. Muscle Fatigue: Fatigued muscles lose their ability to absorb impact, transferring greater forces directly to the bone. This is a common mechanism in stress fractures in endurance athletes.
4. Bone Quality: Factors like bone mineral density, microarchitecture, and intrinsic material properties of bone (e.g., collagen cross-linking) significantly influence its resistance to fracture. Osteoporotic bone, for instance, has reduced bone mass and degraded microarchitecture, making it more susceptible to hairline fractures from minimal trauma.
5. Anatomical Location: Certain bones and regions are inherently more prone to hairline fractures due to their specific biomechanical roles and vascular supply. The femoral neck, scaphoid, and navicular are examples where hairline fractures are particularly concerning due to the risk of avascular necrosis and non-union.
The Remodeling Cascade and Fracture Healing
Following microtrauma, a cascade of biological events initiates to repair the bone. This involves an inflammatory phase, followed by soft and hard callus formation, and finally, remodeling. In hairline fractures, especially stress fractures, this process is ongoing. The initial microfractures can trigger local osteoclastic activity to remove damaged bone, but if the mechanical stress continues unabated, osteoblastic repair cannot keep pace, leading to progressive structural weakening and propagation of the fracture line. This imbalance is critical and explains why early diagnosis and activity modification are paramount.
Indications and Contraindications
The decision-making process for managing hairline fractures hinges on a comprehensive assessment of fracture stability, anatomical location, patient factors, and potential for complications. While many hairline fractures can be managed non-operatively, specific scenarios necessitate surgical intervention.
Non-Operative Management Indications
The majority of stable, non-displaced hairline fractures are amenable to conservative treatment.
* Stable Fracture Pattern: Fractures that do not demonstrate displacement on initial or serial imaging and are not located in areas with high intrinsic instability.
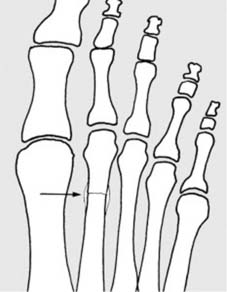
* Low-Risk Anatomical Location: Examples include metatarsal stress fractures (except the base of the fifth metatarsal), fibular stress fractures, and most uncomplicated tibial stress fractures.
* Patient Compliance: Patients capable of adhering to activity modification, non-weight-bearing, or protected weight-bearing protocols.
* Minimal Symptoms: Fractures causing manageable pain with rest and activity modification.
Operative Management Indications
Surgical intervention is generally reserved for hairline fractures that carry a high risk of complications with conservative treatment, fail to heal, or are in critical anatomical locations.
* High-Risk Anatomical Locations:
* Femoral Neck Stress Fractures: Especially tension-side fractures or those with any displacement, due to the high risk of avascular necrosis and complete fracture displacement.
* Scaphoid Fractures: Due to the precarious blood supply and high rate of non-union.
* Talus Fractures: Particularly the neck or body, given the risk of avascular necrosis.
* Navicular Stress Fractures: Often slow to heal and prone to non-union with conservative management, especially in athletes.
* Fifth Metatarsal Base Fractures (Jones Fractures): Known for delayed union and non-union due to poor vascularity in the fracture zone.
* Progression of Displacement: If serial radiographs demonstrate progressive widening or displacement of the fracture line despite adequate conservative measures.
* Delayed or Non-Union: Failure of the fracture to show signs of healing within expected timeframes (e.g., 3-6 months).
* Pathological Hairline Fractures: In cases where the underlying pathology (e.g., aggressive tumor) requires stabilization or biopsy, or where the fracture significantly compromises structural integrity.
* Athlete's Demand: In high-performance athletes, surgical fixation may be considered for certain stress fractures (e.g., tibial, navicular) to accelerate return to sport and minimize downtime, provided the risks are thoroughly discussed.
Contraindications for Surgery
Absolute contraindications for surgical intervention are rare and generally relate to patient-specific factors precluding safe anesthesia and surgery. These include severe acute medical comorbidities (e.g., unstable cardiac disease, uncontrolled sepsis) or extreme frailty where the risks of surgery outweigh the potential benefits. Relative contraindications may include poor patient compliance, local skin conditions (e.g., active infection, severe dermatoses) at the surgical site, or the presence of medical conditions that significantly impair bone healing (e.g., severe uncontrolled diabetes, smoking, chronic steroid use) that have not been adequately addressed.
Operative vs. Non-Operative Indications
The following table summarizes key indications for operative and non-operative management of hairline fractures.
| Feature / Indication | Non-Operative Management | Operative Management |
|---|---|---|
| Fracture Stability | Stable, non-displaced, no progression | Unstable, progressive displacement, delayed/non-union |
| Anatomical Location | Low-risk sites (e.g., some metatarsals, fibula shaft) | High-risk sites (e.g., femoral neck, scaphoid, talus, navicular, Jones fracture) |
| Underlying Pathology | None, or well-controlled metabolic bone disease | Pathological fractures requiring biopsy or stabilization |
| Patient Demands | Low activity level, able to tolerate prolonged immobilization/NWB | High-performance athlete needing accelerated recovery |
| Symptoms | Resolving with rest, tolerable pain | Persistent, debilitating pain despite conservative care |
| Healing Progress | Evidence of healing on serial imaging | Lack of healing, delayed union, or non-union |
| Comorbidities | No significant contraindications for conservative care | Patient fit for surgery, risks of AVN/non-union outweigh surgical risk |
Pre Operative Planning and Patient Positioning
Effective management of hairline fractures, especially those requiring operative intervention, mandates meticulous pre-operative planning and precise patient positioning. Given the often subtle nature of these injuries, diagnostic accuracy is paramount.
Diagnostic Workup and Imaging
The initial clinical suspicion for a hairline fracture arises from a detailed history of the inciting mechanism (trauma vs. repetitive stress), localized pain, tenderness to palpation, and potentially swelling.
-
Clinical Examination: Thorough neurovascular assessment and evaluation of range of motion and stability. Specific tests (e.g., hop test for tibial stress fracture, scaphoid compression test) can be indicative.
-
Initial Radiographs: While often negative in early hairline fractures, high-quality, appropriately centered radiographs are the first line of investigation.
- Multiple Projections: Standard anteroposterior and lateral views are often insufficient. Additional oblique projections of the area may be helpful, especially in complex anatomical regions like the foot or wrist.
- Quality Control: Do not accept poor quality films. Repeat imaging with proper technique is essential.
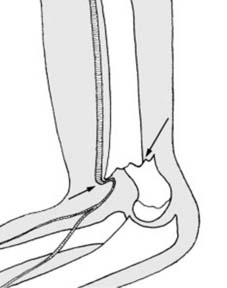
- Delayed Imaging: Films repeated after 7–10 days (or sometimes 2-3 weeks) may show the fracture quite clearly due to early decalcification at the fracture site, which makes the fracture line more visible. This is a crucial strategy.
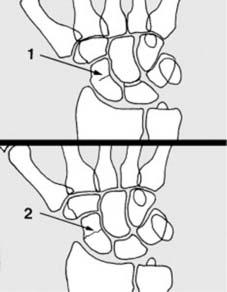
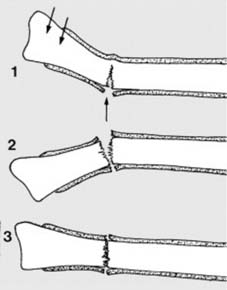
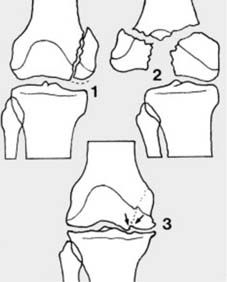
These fractures may be difficult to detect on the radiographs, and where there are reasonable clinical grounds for suspecting a fracture, the rules are quite clear. 1. Additional oblique radiographic projections of the area may be helpful. 2. Do not accept poor quality films. 3. Films repeated after 7–10 days may show the fracture quite clearly (due to decalcification at the fracture site). 4. A CT scan may also help confirm the diagnosis. -
Advanced Imaging:
- Computed Tomography (CT) Scan: A CT scan may also help confirm the diagnosis by providing detailed cross-sectional views, particularly useful for cortical breaks, identification of subtle displacement, or pre-existing bone lesions. It's excellent for visualizing bony anatomy.
- Magnetic Resonance Imaging (MRI): MRI is highly sensitive for detecting bone marrow edema, which is an early sign of stress reactions and fractures, often visible even before a distinct fracture line appears on plain radiographs or CT. It can differentiate between a stress reaction and a complete stress fracture and is invaluable for assessing surrounding soft tissues and ruling out other pathologies.
- Bone Scintigraphy (Bone Scan): Technetium-99m bone scans are very sensitive in detecting areas of increased metabolic activity, characteristic of stress fractures and other bone pathologies. While highly sensitive, it is less specific than MRI for differentiating various causes of bone pain.
Pre-operative Considerations
Once a hairline fracture is confirmed and deemed surgical, planning must address the specific anatomical site and patient context.
* Patient Optimization: Address underlying comorbidities, especially those affecting bone health (e.g., Vitamin D deficiency, osteoporosis, smoking cessation, nutritional status). Optimize glycemic control in diabetic patients.
* Anatomical Specificity: For femoral neck stress fractures, the fracture orientation (tension vs. compression side) dictates fixation strategy. For scaphoid, understanding the vascularity is paramount.
* Implant Selection: Based on fracture location, biomechanical demands, and surgeon preference (e.g., cannulated screws, K-wires, intramedullary nails, plates).
* Consent: Thorough discussion with the patient regarding the nature of the fracture, surgical procedure, potential complications (non-union, AVN), rehabilitation, and expected outcomes.
Patient Positioning and Surgical Preparation
Patient positioning is critical for optimal surgical exposure and access, ensuring the ability to achieve anatomical reduction and stable fixation while minimizing iatrogenic injury.
* General Principles: Maintain physiological alignment, prevent pressure injuries, ensure airway access, and facilitate fluoroscopic imaging.
* Lower Extremity: For femoral neck, supine on a fracture table or radiolucent table for traction and imaging. For tibia or fibula, supine with knee flexed or lateral decubitus. For foot, supine or prone depending on the specific bone.

* Upper Extremity: For scaphoid, supine with arm extended on a hand table. For humerus, supine or lateral decubitus.

* Sterile Field: Wide sterile preparation and draping to allow for extension of the incision or unanticipated exposure.

Detailed Surgical Approach and Technique
The surgical management of hairline fractures, when indicated, demands precision and a nuanced understanding of local anatomy and biomechanics. While specific techniques vary by fracture location, common principles guide the approach.
Principles of Hairline Fracture Fixation
- Minimally Invasive Approaches: Whenever feasible, percutaneous or mini-open techniques are preferred to minimize soft tissue disruption, preserve vascularity, and reduce post-operative pain and recovery time.
- Anatomical Reduction: Even hairline fractures can have subtle displacement or angulation that can lead to non-union or chronic pain. If displacement is present or develops, anatomical reduction is crucial.
- Stable Fixation: The goal is to provide sufficient stability to allow for primary bone healing while permitting early controlled mobilization as appropriate. Compression across the fracture site is often desired.
- Preservation of Vascularity: Meticulous dissection to protect local blood supply, particularly critical in areas with tenuous vascularity like the scaphoid or femoral head.
- Biologic Augmentation: In cases of delayed or non-union, or in areas with poor healing potential, adjunctive measures such as bone grafting (autograft or allograft), bone marrow aspirate concentrate (BMAC), or platelet-rich plasma (PRP) may be considered.
Surgical Approaches and Techniques by Location
Femoral Neck Stress Fractures
Tension-side femoral neck stress fractures and those with any degree of displacement carry a high risk of complete fracture, avascular necrosis (AVN), and non-union.
* Approach: An anterolateral or direct lateral approach to the proximal femur is typically utilized.
* Technique: Percutaneous cannulated screw fixation is the preferred method. Multiple screws (usually 2 or 3) are placed in a triangular or parallel fashion to provide rigid fixation. Image intensification is critical for accurate screw placement, ensuring they cross the fracture site and engage the femoral head effectively.
Scaphoid Waist Stress Fractures
Due to its precarious blood supply, scaphoid hairline fractures require careful consideration.
* Approach: Dorsal or volar approach depending on surgeon preference and fracture configuration. A dorsal approach may involve dissecting between the extensor pollicis longus and extensor pollicis brevis, while a volar approach may involve the interval between the flexor carpi radialis and the radial artery.
* Technique: Percutaneous screw fixation (e.g., Herbert screw, cannulated headless screw) is common. The screw is typically inserted across the waist of the scaphoid to provide interfragmentary compression. Bone grafting may be added if there is significant bone loss or signs of non-union.

Tibial Stress Fractures (Anterior Cortex)
"Dreaded black line" stress fractures of the anterior tibial cortex are high-risk for non-union.
* Approach: An anteromedial approach to the tibia.
* Technique: Intramedullary nailing or plate fixation may be required. IM nailing provides excellent stability for diaphyseal fractures. For focal cortical defects, curettage and bone grafting with plate neutralization can be employed.

Navicular Stress Fractures
Common in athletes and prone to non-union.
* Approach: Dorsal approach to the midfoot, carefully dissecting to avoid neurovascular structures.
* Technique: Percutaneous screw fixation across the fracture line, often with bone grafting (autogenous cancellous bone graft) if there is sclerosis or a history of delayed healing.

Fifth Metatarsal Base Fractures (Jones Fractures)
These metaphyseal-diaphyseal junction fractures have a high non-union rate.
* Approach: Dorsolateral incision over the base of the fifth metatarsal.
* Technique: Intramedullary screw fixation is typically performed, often a solid, fully threaded screw to maximize purchase in the metaphysis. Bone grafting may be considered in chronic non-unions.
Intraoperative Considerations
- Fluoroscopy: Essential for guiding reduction and implant placement, verifying screw length, and confirming appropriate compression.
- Soft Tissue Management: Gentle handling of tissues, meticulous hemostasis, and proper wound closure are critical to minimize infection and promote healing.
- Bone Grafting: For atrophic non-unions or where bone viability is a concern, bone graft harvest and application are integrated into the technique.
- Final Assessment: Before closure, ensure stability, confirmed reduction, and appropriate implant positioning on final fluoroscopic views.
Complications and Management
Despite meticulous surgical technique and attentive post-operative care, hairline fractures, especially those requiring operative intervention, are not without potential complications. Recognizing these early and implementing effective salvage strategies is crucial for optimizing patient outcomes.
Common Complications
- Delayed Union and Non-Union: This is arguably the most common and significant complication, particularly for high-risk hairline fractures (e.g., scaphoid, femoral neck, navicular, Jones fractures, anterior tibial stress fractures). The incidence varies significantly by anatomical site and patient factors, ranging from 5-10% in some well-managed cases to 30% or more in challenging stress fracture patterns.
- Avascular Necrosis (AVN): A devastating complication, especially in bones with tenuous blood supply (e.g., femoral head, scaphoid, talus). AVN can lead to bone collapse, severe pain, and degenerative arthritis. Its incidence with hairline fractures is generally lower than with displaced fractures but remains a significant concern in high-risk locations.
- Progression to Displaced Fracture: If a hairline fracture, particularly a stress fracture, continues to be loaded inappropriately, it can propagate and displace, converting a relatively stable injury into a complex one requiring more extensive surgery and carrying a worse prognosis. This risk is higher with tension-sided fractures.
- Hardware-Related Complications: Applicable to surgically managed cases. These include:
- Infection: Superficially (1-5%) or deep (<1%).
- Implant prominence/irritation: Requiring hardware removal (5-20%).
- Implant failure: Breakage, pull-out, or migration due to inadequate fixation or premature loading (<5%).
- Chronic Pain: Persistent pain at the fracture site or adjacent joints, even after radiographic healing, can result from nerve irritation, residual malalignment, or post-traumatic arthritis.
- Complex Regional Pain Syndrome (CRPS): A rare but severe complication characterized by disproportionate pain, swelling, and autonomic dysfunction.
- Refracture: Especially in athletes returning to high-impact activities without adequate bone healing or rehabilitation.
Management and Salvage Strategies
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Delayed Union / Non-Union | 5-30% | Conservative: Prolonged immobilization, non-weight-bearing, electrical stimulation, nutritional optimization. Surgical: Revision fixation (e.g., larger screws, plates), fresh autogenous bone grafting (corticocancellous or cancellous), vascularized bone graft (for severe cases like scaphoid), IM nailing, biological adjuncts (BMAC, PRP). |
| Avascular Necrosis (AVN) | 2-15% (site-dependent) | Early: Core decompression, vascularized bone graft, electrical stimulation. Late: Arthroplasty (hip, shoulder), arthrodesis (talus, scaphoid), joint reconstruction. |
| Progression to Displaced Fracture | 5-10% | Immediate surgical open reduction and internal fixation (ORIF) with appropriate implants (e.g., plates, screws, IM nails) to restore anatomy and stability. Address underlying causes (e.g., remove activity restrictions). |
| Hardware-Related Complications | 5-20% (prominence) / <5% (failure) | Prominence/Irritation: Elective hardware removal after fracture healing. Infection: Debridement, antibiotics, implant retention (if stable) or removal (if unstable/deep infection), potentially revision surgery. Failure: Revision fixation, potentially bone grafting. |
| Chronic Pain | Variable | Physical therapy, pain management consultation, NSAIDs, neuropathic pain medications, diagnostic injections, psychological support. Rule out nerve impingement or residual pathology. Revision surgery if structural cause identified. |
| Complex Regional Pain Syndrome (CRPS) | <1% | Early diagnosis is key. Multidisciplinary approach: physical therapy, occupational therapy, pain management specialists (nerve blocks, neuromodulation), psychological support, medications (e.g., gabapentin, amitriptyline, corticosteroids). |
| Refracture | Variable | Treat as a new fracture (conservative or surgical), re-evaluate underlying bone health (osteoporosis, metabolic workup), ensure adequate rehabilitation and gradual return to activity. |
Prophylaxis and Monitoring
Many complications can be mitigated through rigorous adherence to pre-operative planning, meticulous surgical technique, and robust post-operative protocols. Close radiographic and clinical follow-up is essential to detect early signs of delayed healing, implant issues, or impending complications. Patient education on activity restrictions, weight-bearing precautions, and warning signs is critical for minimizing the risk of progression or refracture. Optimizing bone health through adequate calcium and vitamin D intake, and treating underlying osteoporosis, are fundamental prophylactic measures.
Post Operative Rehabilitation Protocols
Post-operative rehabilitation following the management of hairline fractures, especially those requiring surgical intervention, is a critical phase designed to restore function, prevent complications, and facilitate a safe return to pre-injury activity levels. The protocol must be individualized, considering the fracture location, type of fixation, bone quality, and patient-specific factors such as age, activity level, and comorbidities.
General Principles of Rehabilitation
- Protection and Immobilization: Initially, the fracture site requires protection to allow for early healing. This may involve bracing, casting, or restricted weight-bearing. The duration depends on the stability of fixation and the healing potential of the bone.
- Controlled Mobilization: Gradually introduce range of motion exercises to prevent stiffness and promote joint health, without compromising fracture stability.
- Graduated Weight-Bearing: Progression of weight-bearing is carefully monitored, often guided by radiographic evidence of healing and clinical stability. This typically moves from non-weight-bearing (NWB) to toe-touch weight-bearing (TTWB), partial weight-bearing (PWB), and finally, weight-bearing as tolerated (WBAT).
- Strengthening: Once adequate healing is established, progressive strengthening exercises for muscles surrounding the injured bone and adjacent joints are initiated.
- Proprioception and Balance Training: Essential, especially for lower extremity fractures, to restore neuromuscular control and reduce the risk of re-injury.
- Functional Training: Activity-specific drills are introduced as healing progresses, mimicking movements required for daily living or sports.
- Bone Health Optimization: Continue to monitor and manage factors influencing bone density and metabolism, such as Vitamin D and calcium supplementation, and anti-osteoporotic medications if indicated.
Phase-Specific Protocols (Illustrative Examples)
Phase 1: Immobilization and Early Protection (Weeks 0-6)
- Goal: Protect the fracture site, manage pain and swelling, maintain joint mobility in unaffected areas.
- Weight-Bearing: Typically NWB or TTWB, depending on fracture stability and location (e.g., NWB for femoral neck, scaphoid; TTWB for some metatarsal fractures).
- Exercises: Gentle, active range of motion for adjacent non-immobilized joints. Isometric exercises for muscles in the immobilized limb (e.g., quadriceps sets, gluteal sets). Upper body conditioning.
Phase 2: Controlled Mobilization and Gradual Weight-Bearing (Weeks 6-12)
- Goal: Increase range of motion, initiate partial weight-bearing, begin gentle strengthening.
- Weight-Bearing: Progress from TTWB to PWB, then WBAT as clinically and radiographically indicated. Use crutches or a walker for support.
- Exercises: Active and passive range of motion for the injured joint. Gentle resisted exercises using bands or light weights. Core strengthening. Stationary cycling (if lower extremity). Aquatic therapy.
Phase 3: Progressive Strengthening and Neuromuscular Control (Weeks 12-24)
- Goal: Restore full strength, endurance, and proprioception. Prepare for functional activities.
- Weight-Bearing: Full weight-bearing. Discontinue assistive devices.
- Exercises: Progressive resistive exercises for all major muscle groups. Balance and proprioception drills (e.g., single-leg stance, unstable surfaces). Plyometrics (if appropriate for location and healing status). Begin sport-specific drills at low intensity.
Phase 4: Return to Activity/Sport (Months 6+)
- Goal: Gradual, safe return to pre-injury activity levels or sport.
- Criteria: Full pain-free range of motion, restored strength (e.g., >90% strength compared to contralateral limb), good balance, radiographic evidence of complete healing. Psychological readiness.
- Protocol: Graded return to activity under supervision. Gradual increase in intensity, duration, and frequency of sport-specific training. Emphasize proper biomechanics and conditioning to prevent re-injury. Stress fracture patients may require bone density screening and consultation with a sports nutritionist.
Monitoring and Adjustments
Throughout rehabilitation, regular clinical and radiographic assessments are crucial. Pain, swelling, and any new instability warrant a re-evaluation of the protocol. Non-union or delayed union may necessitate a return to earlier protective phases or consideration of salvage surgical procedures. Communication between the surgeon, physical therapist, and patient is paramount for optimal outcomes.
Summary of Key Literature and Guidelines
The literature on hairline fractures, particularly stress fractures and occult fractures, highlights a consistent theme: early and accurate diagnosis is critical to prevent potentially devastating complications. Our understanding continues to evolve through advancements in imaging and biomechanical research.
Diagnostic Algorithms
Current guidelines from professional organizations like the American Academy of Orthopaedic Surgeons (AAOS) emphasize a tiered diagnostic approach.
* Clinical Suspicion: Maintain a high index of suspicion, especially in athletes with localized pain or individuals with risk factors for bone fragility.
* Initial Radiographs: While often negative, they are essential to rule out more overt fractures and serve as a baseline. The importance of repeat radiographs in 10-14 days for occult fractures is well-documented in the literature, as early bone resorption at the fracture site can make the line visible.
* Advanced Imaging: MRI is considered the gold standard for early detection of stress fractures due to its sensitivity in identifying bone marrow edema before a visible fracture line appears. CT scans are superior for delineating cortical breaks and complex bony anatomy, while bone scans, though highly sensitive, offer less anatomical detail.
Management Guidelines
The management of hairline fractures varies significantly based on location and risk of complications.
* Conservative Management: The vast majority of stable, low-risk hairline fractures are successfully managed non-operatively with activity modification, rest, and protected weight-bearing. For stress fractures, this typically involves a period of relative rest, followed by gradual return to activity guided by pain. Adherence to a structured rehabilitation program is essential.
* Surgical Intervention: For high-risk stress fractures (e.g., tension-sided femoral neck, scaphoid, anterior tibia, navicular, Jones fractures), or those failing conservative management, surgical fixation is often recommended. Meta-analyses and systematic reviews consistently demonstrate lower rates of non-union and faster return to sport with surgical intervention in these specific high-risk scenarios compared to prolonged conservative treatment. For instance, strong evidence supports internal fixation for displaced femoral neck stress fractures to prevent AVN and non-union.
* Pathological Fractures: Management of pathological hairline fractures necessitates addressing the underlying lesion. This may involve biopsy, tumor resection, or stabilization to prevent further fracture or progression.
Emerging Concepts and Future Directions
- Biologic Augmentation: Research continues into the efficacy of biological adjuncts such as bone marrow aspirate concentrate (BMAC), platelet-rich plasma (PRP), and growth factors to enhance bone healing, particularly in non-unions and recalcitrant stress fractures.
- Advanced Imaging Techniques: Quantitative CT and high-resolution MRI are exploring microstructural changes in bone to better predict fracture risk and monitor healing.
- Personalized Medicine: Genetic factors influencing bone metabolism and stress fracture susceptibility are under investigation, potentially leading to personalized prevention and treatment strategies.
- Bone Health Management: Increased emphasis on comprehensive bone health assessment and management (Vitamin D, calcium, endocrinology consultation) as a cornerstone of both prevention and treatment for hairline fractures, particularly insufficiency fractures.
In conclusion, hairline fractures, though subtle, demand meticulous attention from orthopedic practitioners. Their potential for progression, non-union, and other severe complications necessitates a systematic diagnostic approach, careful risk stratification, and tailored management strategies. Staying abreast of the evolving literature and guidelines is crucial for optimizing patient care and outcomes in this challenging area of orthopedic trauma.
Clinical & Radiographic Imaging