Unlock Perfect Reduction: Key Techniques in Fracture Management
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Unlock Perfect Reduction: Key Techniques in Fracture Management. Techniques in fracture reduction commonly involve closed methods, starting with traction along the limb's line to disimpact fragments and correct shortening. Any residual angulation is then addressed with localized hand pressure. In challenging cases, initial increased angulation may help unlock fragments. Post-reduction, stabilization is critical using methods like plaster fixation, various traction types, cast bracing, or external fixation to prevent redisplacement.
Introduction and Epidemiology
Achieving anatomical reduction is a cornerstone of fracture management, directly correlating with favorable functional outcomes, minimized pain, and reduced incidence of post-traumatic complications. Perfect reduction in orthopedic trauma signifies the restoration of length, alignment, rotation, and joint congruity to as near anatomical as possible, within the limits of biological healing and patient physiology. This objective is particularly critical for intra-articular fractures where even minor incongruity can lead to accelerated degenerative changes and persistent dysfunction.

Fractures represent a ubiquitous burden on global healthcare systems. Their epidemiology varies widely based on age, mechanism of injury, and geographic location. The distribution of fractures typically follows a bimodal curve. High-energy trauma, such as motor vehicle collisions and falls from height, predominantly affects the younger demographic, resulting in complex diaphyseal and articular fracture patterns. Conversely, low-energy mechanisms, primarily simple falls, are the leading cause of fractures in the elderly osteoporotic population, frequently involving the proximal femur, distal radius, and proximal humerus.

Regardless of the specific fracture type or patient demographic, the principles of reduction remain paramount. The primary goal of any osteosynthesis is to facilitate optimal biological healing and reconstruct the skeletal architecture to withstand physiological loads. This allows for the return of patients to their pre-injury functional status, or the best possible outcome given the injury severity. The decision between closed and open reduction, and the subsequent choice of fixation, is a complex process guided by fracture characteristics, patient factors, and surgical expertise, all centered around achieving and maintaining an optimal reduction.
Surgical Anatomy and Biomechanics
A thorough understanding of regional surgical anatomy and the biomechanical forces influencing fracture patterns is indispensable for effective reduction. The specific anatomical location dictates the inherent stability of a fracture and its propensity for displacement.
Deforming Muscle Forces
Muscular attachments exert significant deforming forces on fracture fragments, leading to characteristic displacements. For instance, in a subtrochanteric femoral fracture, the iliopsoas typically causes flexion and external rotation of the proximal fragment, while the abductors pull it into abduction. In contrast, distal radius fractures often displace dorsally and radially due to muscle and ligamentous pull. Understanding these forces is critical for applying counter-forces during reduction maneuvers.

Principles of Ligamentotaxis
This principle is particularly relevant for articular fractures, such as those of the calcaneus, distal radius, or pilon. Intact ligaments spanning a fracture can be tensioned through traction, thereby indirectly reducing articular fragments. This technique leverages the capsuloligamentous attachments to guide fragments back into position, often obviating the need for extensive soft tissue dissection and preserving the delicate vascular supply to the metaphyseal and epiphyseal bone.

The Periosteal Hinge and Fracture Personality
In many closed fractures, an intact periosteal sleeve on one side of the bone can act as a hinge, facilitating reduction by providing a stable pivot point. This hinge must be protected during reduction maneuvers, as its disruption can convert a relatively simple reduction into a more complex one with increased instability. Each fracture possesses a unique personality defined by its morphology, location, and degree of displacement. Simple, stable fracture patterns may be amenable to closed reduction and cast immobilization, while complex, highly comminuted, or intra-articular fractures often necessitate open reduction and internal fixation to restore anatomy and achieve stability.

Bone Quality and Strain Theory
The biomechanical properties of the bone itself significantly influence reduction strategies. Osteoporotic bone is prone to comminution and may not hold fixation well, requiring specific implant designs and reduction techniques that minimize stress risers and maximize construct stability through load-sharing rather than load-bearing mechanisms. Furthermore, Perren’s strain theory dictates the type of healing that will occur based on the mechanical environment. Absolute stability, achieving a strain environment of less than two percent, promotes primary bone healing via cutting cones. Relative stability, which allows for a strain environment between two and ten percent, promotes secondary bone healing through the formation of an endochondral callus.

Indications and Contraindications
The pursuit of perfect anatomical reduction is not universally indicated for all fracture patterns. The decision to pursue absolute anatomical reduction versus functional alignment depends heavily on the anatomical location of the fracture and the physiological demands of the patient. Intra-articular fractures demand meticulous anatomical reduction to restore joint congruity, minimize step-offs, and prevent the rapid onset of post-traumatic osteoarthritis. Diaphyseal fractures of the forearm also require exact anatomical reduction to restore the complex biomechanics of pronation and supination.

Conversely, diaphyseal fractures of the femur and tibia are often managed with principles of relative stability. In these scenarios, the restoration of length, alignment, and rotation is prioritized over the exact anatomical reconstruction of every comminuted fragment. Attempting to perfectly reduce a highly comminuted diaphyseal fracture often requires extensive soft tissue stripping, which devascularizes the bone fragments and significantly increases the risk of nonunion and infection.

| Clinical Scenario | Indication for Operative Reduction | Indication for Non Operative Management |
|---|---|---|
| Intra Articular Fractures | Step off greater than 2mm or instability | Nondisplaced with stable joint kinematics |
| Forearm Diaphysis | Displaced fractures requiring rotational restoration | Truly nondisplaced fractures in pediatric patients |
| Femoral Diaphysis | Almost all adult diaphyseal fractures | Severe medical comorbidities precluding anesthesia |
| Tibial Diaphysis | Unacceptable alignment or open fractures | Acceptable alignment maintained in a long leg cast |
| Pelvic Ring | Hemodynamic instability or mechanical instability | Mechanically stable injuries with minimal displacement |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is the foundation of a successful surgical reduction. This phase transforms a complex, potentially chaotic intraoperative situation into a structured, step-by-step execution of a tactical plan.
Radiographic Analysis and Templating
High-quality orthogonal radiographs are mandatory. For complex articular fractures, a computed tomography scan with two-dimensional multiplanar reformats and three-dimensional reconstructions is essential to understand the fracture morphology, the location of the primary fracture lines, and the presence of articular impaction.

Digital templating allows the surgeon to anticipate the required implant size, screw trajectory, and the sequence of reduction. The tactical plan should outline the primary reduction strategy, the provisional fixation methods, the definitive fixation construct, and alternative salvage plans should the primary strategy fail. Anticipating the need for specific reduction tools, such as large pointed reduction forceps, femoral distractors, or specific retractors, ensures that the surgical team is adequately prepared.

Operating Room Setup and Fluoroscopy
Patient positioning must facilitate both the surgical approach and the acquisition of unhindered fluoroscopic images. The use of radiolucent tables is standard for most extremity trauma. For fractures of the proximal femur or femoral shaft, a fracture table may be utilized to apply controlled traction and assist with indirect reduction.

The positioning of the C-arm should be planned in advance to ensure that orthogonal views can be obtained without compromising the sterile field or requiring awkward maneuvering of the limb. Proper padding of all bony prominences is critical to prevent perioperative neuropathies, particularly when traction is applied for extended periods.
Detailed Surgical Approach and Technique
The execution of a perfect reduction relies on a deep understanding of surgical approaches, the judicious use of internervous planes, and the mastery of both direct and indirect reduction techniques.
Principles of Internervous Planes
Surgical approaches should exploit internervous and intermuscular planes to minimize denervation and devascularization of the surrounding musculature. For example, the volar Henry approach to the radius utilizes the interval between the flexor carpi radialis and the brachioradialis proximally, and the flexor pollicis longus and the brachioradialis distally. Respecting these anatomical boundaries ensures that the biological envelope surrounding the fracture is preserved, which is a critical factor in subsequent fracture healing.

Direct Reduction Techniques
Direct reduction involves the visualization and physical manipulation of the fracture fragments. This is primarily indicated for articular fractures and simple diaphyseal fractures where absolute stability is required.

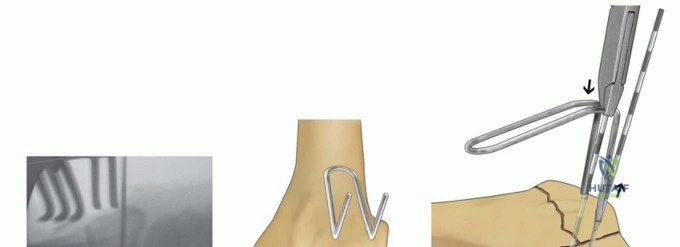
Pointed reduction forceps, often referred to as Weber clamps, are invaluable for applying compression across a fracture plane. When applying these clamps, the tines must be positioned perpendicular to the fracture line to prevent sheer forces that can cause displacement during compression.

In cases of dense cortical bone, small drill holes can be created to provide purchase points for the clamp tines, a technique particularly useful in the reduction of oblique tibial or femoral fractures. Schanz pins can be inserted into fracture fragments and used as "joysticks" to manipulate the bone in multiple planes, providing a powerful lever arm for correcting rotational and angular deformities.
Indirect Reduction Techniques
Indirect reduction prioritizes the preservation of the soft tissue envelope by manipulating the fracture fragments without direct exposure of the fracture site. This is the preferred method for comminuted diaphyseal and metaphyseal fractures.

Traction is the most fundamental indirect reduction technique. Longitudinal traction restores length and utilizes the principle of ligamentotaxis to align the intermediate fragments. A femoral distractor or an external fixator can be applied to maintain this traction, freeing the surgeon's hands to fine-tune the alignment and apply fixation.

The use of a plate as a reduction tool is another powerful indirect technique. By securing a contoured plate to one main fragment, the plate can be used as a template to draw the remaining fragment into alignment using cortical screws or specialized reduction devices such as the articulated tension device.

Intramedullary nailing inherently relies on indirect reduction techniques. The passage of the guide wire and the subsequent reaming process act to align the medullary canal. Poller screws (blocking screws) can be strategically placed adjacent to the medullary canal to narrow the path of the nail, forcing it into a trajectory that corrects angular deformities in metaphyseal fractures.

Fixation Strategies
Once reduction is achieved, it must be provisionally stabilized with Kirschner wires or reduction forceps before definitive fixation is applied. The choice of definitive fixation—whether lag screws, neutralization plates, bridge plates, or intramedullary nails—depends on the mechanical requirements of the fracture and the biological environment.

When utilizing lag screw techniques for absolute stability, the glide hole must be drilled in the near cortex and the thread hole in the far cortex to ensure interfragmentary compression. Neutralization plates are then applied to protect the lag screw from torsional and bending forces. In comminuted fractures managed with relative stability, bridge plating techniques are employed, utilizing long plates with a low screw density to provide a flexible construct that stimulates secondary bone healing.

Complications and Management
Despite meticulous planning and execution, complications in fracture reduction and fixation can occur. Recognizing these complications early and understanding the salvage pathways is critical for the orthopedic surgeon.

Malreduction, particularly in intra-articular fractures, is a primary driver of poor outcomes. Articular step-offs alter joint contact pressures, leading to localized cartilage overload and rapid degeneration. In diaphyseal fractures, malrotation or significant angular deformity can alter the mechanical axis of the limb, predisposing adjacent joints to early osteoarthritis.

Nonunion and delayed union are often the result of either inadequate mechanical stability or a compromised biological environment. Hypertrophic nonunions, characterized by abundant callus formation that fails to bridge the fracture gap, indicate adequate biology but insufficient mechanical stability. The management typically involves increasing the stability of the construct, often through the application of compression plating or the exchange of an intramedullary nail to a larger diameter. Atrophic nonunions, conversely, lack callus formation and indicate a failure of biology. Management requires debridement of fibrous tissue, opening of the medullary canal, and the application of bone graft to stimulate osteogenesis, alongside rigid fixation.

| Complication | Incidence Rate | Etiology and Risk Factors | Salvage Strategy |
|---|---|---|---|
| Malreduction | Varies by fracture | Inadequate visualization or failure to recognize deforming forces | Early revision osteosynthesis or corrective osteotomy |
| Hypertrophic Nonunion | 2 to 5 percent | Inadequate mechanical stability with preserved biology | Improve construct stiffness and apply compression |
| Atrophic Nonunion | 1 to 3 percent | Excessive soft tissue stripping or poor host biology | Biological augmentation with autograft and rigid fixation |
| Deep Infection | 1 to 5 percent | Open fractures or prolonged operative duration | Radical debridement, hardware removal if loose, targeted antibiotics |
| Hardware Failure | 1 to 4 percent | Premature weight bearing or nonunion leading to fatigue failure | Revision fixation with correction of underlying mechanical or biological failure |
Post Operative Rehabilitation Protocols
The success of a perfect surgical reduction is ultimately realized through a structured, biologically appropriate postoperative rehabilitation protocol. The mechanobiology of the healing fracture dictates the progression of weight-bearing and mobilization.
Early Mobilization Strategies
Early range of motion of the adjacent joints is paramount to prevent capsular contracture, minimize tendon adhesions, and promote cartilage nutrition. For intra-articular fractures managed with absolute stability, early active and passive range of motion is typically initiated within the first few postoperative days. The rigid fixation construct protects the anatomical reduction while the movement stimulates synovial fluid circulation, which is essential for the metabolic maintenance of the articular chondrocytes.

Weight Bearing Progression
The progression of weight-bearing is directly tied to the type of fixation and the anticipated mode of bone healing. Constructs providing relative stability, such as intramedullary nails in diaphyseal fractures, often permit early progressive weight-bearing. The micromotion at the fracture site under physiological loading stimulates the formation of an endochondral callus.

Conversely, fractures managed with absolute stability via lag screws and neutralization plates rely on primary bone healing. These constructs are highly susceptible to fatigue failure if subjected to cyclical loading before the cutting cones have bridged the fracture site. Therefore, weight-bearing is typically restricted until radiographic evidence of primary healing is observed, which may take several weeks to months depending on the anatomical location and patient biology.
Summary of Key Literature and Guidelines
The evolution of fracture management is deeply rooted in the foundational work of the AO Foundation (Arbeitsgemeinschaft für Osteosynthesefragen). The original tenets of anatomical reduction, stable internal fixation, preservation of blood supply, and early active pain-free mobilization remain the bedrock of modern orthopedic trauma surgery.

Landmark biomechanical studies by Stephan Perren defined the relationship between interfragmentary strain and the mode of bone healing, shifting the paradigm from a strict demand for absolute stability in all fractures to the acceptance of relative stability and biological osteosynthesis for diaphyseal and comminuted metaphyseal injuries. Clinical outcome studies, such as the seminal work by Joel Matta on acetabular fractures, unequivocally demonstrated that the quality of the articular reduction is the single most important predictor of long-term joint survivorship. Similarly, studies by Jesse Jupiter on distal radius fractures highlighted the necessity of restoring volar tilt, radial inclination, and ulnar variance to optimize functional outcomes. These academic pillars continue to guide the tactical decision-making process, ensuring that the pursuit of perfect reduction is balanced with the biological imperatives of fracture healing.
