Comprehensive Introduction and Patho-Epidemiology
The Achilles tendon, representing the confluent aponeurotic extension of the gastrocnemius and soleus muscles, stands as the largest, thickest, and most biomechanically robust tendinous structure in the human body. Despite its formidable macroscopic architecture, which is engineered to withstand tensile loads exceeding ten times the body weight during explosive athletic maneuvers, it remains paradoxically highly susceptible to acute rupture. The incidence of acute Achilles tendon ruptures has seen a dramatic epidemiological surge over the past three decades, currently estimated at 18 to 32 per 100,000 person-years in Western populations. This rising prevalence is multifactorial, driven largely by an aging demographic that remains highly active in recreational sports—the classic "weekend warrior" phenomenon—as well as the increasing systemic use of fluoroquinolone antibiotics and corticosteroid injections, which induce rapid tenocyte apoptosis and collagen degradation.
The pathophysiology of an Achilles tendon rupture is rarely an event of pure acute mechanical overload in a perfectly healthy tendon; rather, it is the catastrophic endpoint of a chronic, often asymptomatic, degenerative continuum. Histopathological analyses of ruptured Achilles tendons invariably demonstrate pre-existing tendinosis, characterized by mucoid degeneration, hypoxic tenocyte necrosis, neovascularization, and a disorganized extracellular matrix with a pathological shift from Type I to Type III collagen. This degenerative cascade is most pronounced in the critical "watershed" zone, a region of relative hypovascularity located precisely 2 to 6 centimeters proximal to the calcaneal insertion. When a sudden eccentric load is applied to the dorsiflexed ankle—such as during the push-off phase of a sprint or a sudden change in direction—the diminished tensile capacity of this degenerative zone is exceeded, resulting in structural failure.
The management paradigm for acute Achilles tendon ruptures has been the subject of intense, decades-long debate within the orthopedic community, oscillating between operative and non-operative strategies. Historically, conservative management was plagued by unacceptably high rerupture rates (often exceeding 10-12%) and profound deficits in plantarflexion power, leading to a strong predilection for surgical intervention. However, the advent of dynamic functional rehabilitation protocols has significantly improved non-operative outcomes, narrowing the gap in rerupture rates between the two modalities. Nevertheless, open surgical repair remains the definitive gold standard for specific patient cohorts. It provides unparalleled biomechanical construct stiffness, allows for precise anatomical restoration of the musculotendinous resting length (crucial for optimizing the length-tension relationship of the triceps surae), and facilitates aggressive early rehabilitation. Open repair is particularly indicated for young, high-demand athletes, patients presenting with delayed or chronic ruptures, and cases involving large gap defects where biological bridging without surgical approximation is impossible.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the posterior ankle anatomy and the intricate biomechanical properties of the Achilles tendon is absolutely paramount for the operating surgeon. The tendon is formed by the coalescence of the gastrocnemius aponeurosis, which contributes the superficial and lateral fibers, and the soleus aponeurosis, which contributes the deep and medial fibers. As these fibers descend toward their insertion on the middle third of the posterior calcaneal tuberosity, they undergo a complex 90-degree internal rotation. This spiral configuration is not merely an anatomical curiosity; it is a critical biomechanical adaptation that allows the tendon to store and release elastic strain energy efficiently while accommodating the multi-planar forces generated during the gait cycle. The medial fibers of the proximal tendon become the posterior fibers distally, a structural nuance that the surgeon must respect when re-approximating frayed tendon ends to avoid rotational malalignment.
Unlike flexor tendons of the hand or the posterior tibial tendon, the Achilles tendon lacks a true synovial sheath. Instead, it is enveloped by the paratenon, a highly specialized, richly vascularized, multi-layered fascial sleeve consisting of a superficial epitenon and a deeper peritenon. The paratenon functions as both a biological gliding mechanism, reducing friction against surrounding tissues, and the primary source of extrinsic vascularity to the tendon mid-substance. The intrinsic blood supply, derived from the musculotendinous junction proximally and the osseous insertion distally, is notoriously tenuous. The mid-substance relies heavily on transverse segmental vessels arising from the posterior tibial and peroneal arteries, which traverse the anterior mesotenon to penetrate the tendon. Surgical dissection must meticulously preserve this paratenon-mesotenon complex. Stripping the paratenon or aggressively dissecting anterior to the tendon devascularizes the tissue, precipitating delayed healing, massive necrosis, and catastrophic repair failure.
The neural anatomy of the posterior leg demands equal vigilance, specifically concerning the sural nerve. Formed by the confluence of the medial sural cutaneous nerve (a branch of the tibial nerve) and the sural communicating branch (from the common peroneal nerve), the sural nerve courses distally along the posterolateral aspect of the calf, accompanied by the lesser saphenous vein. Critically for the orthopedic surgeon, the nerve crosses the lateral border of the Achilles tendon at a highly variable distance, averaging 9.8 cm (range, 7 to 13 cm) proximal to the calcaneal insertion. From this crossing point, it runs intimately close to the lateral margin of the tendon before passing posterior to the lateral malleolus. Consequently, surgical incisions and percutaneous suture passes are universally biased toward the posteromedial aspect of the tendon to mitigate the risk of iatrogenic sural nerve entrapment, transection, or neuroma formation, which can result in debilitating chronic pain and lateral foot numbness.
Exhaustive Indications and Contraindications
The decision algorithm for operative versus non-operative management of an Achilles tendon rupture requires a highly individualized approach, synthesizing the patient's physiological age, functional demands, medical comorbidities, and the morphological characteristics of the tear. Open surgical repair is definitively indicated in high-level athletes and active individuals who demand maximal restoration of plantarflexion peak torque and endurance. Furthermore, operative intervention is mandatory for delayed presentations (typically defined as >2-3 weeks post-injury) where proximal muscle retraction and gap formation preclude apposition through conservative equinus casting. Patients who have failed initial conservative management or present with a rerupture are also absolute candidates for open surgical exploration and augmentation.
Conversely, the surgeon must exercise extreme caution in patient populations where the biological envelope is compromised. The posterior ankle is characterized by thin, poorly vascularized fasciocutaneous tissue that is exquisitely sensitive to ischemia. Patients with severe peripheral vascular disease, poorly controlled diabetes mellitus with microvascular complications, or a history of significant tobacco use are at an exponentially higher risk for devastating postoperative complications, including wound dehiscence, deep soft tissue infection, and ultimate loss of the limb. In these cohorts, the risks of surgical intervention often far outweigh the biomechanical benefits, and non-operative management with a functional orthosis is strongly recommended.
Additionally, local skin conditions, such as active cellulitis, severe stasis dermatitis, or massive fracture blisters overlying the surgical site, represent absolute contraindications to immediate open repair. In such scenarios, surgery must be delayed until the soft tissue envelope has completely normalized, or alternative minimally invasive/percutaneous techniques should be considered if the timeline permits. The table below delineates the specific indications and contraindications to guide clinical decision-making.
| Category | Specific Criteria / Condition | Rationale / Clinical Context |
|---|---|---|
| Absolute Indications | High-demand athletes / Young active patients | Maximizes construct stiffness; restores precise musculotendinous length for peak push-off power. |
| Absolute Indications | Delayed presentation (>3 weeks) with gap | Retraction of the gastrocnemius-soleus complex prevents conservative apposition; requires open mobilization/augmentation. |
| Absolute Indications | Open Achilles tendon lacerations | Requires formal irrigation, debridement, and primary repair to prevent deep infection and restore continuity. |
| Relative Indications | Palpable gap >3 cm in resting equinus | High risk of elongation and weakness if treated non-operatively; surgery ensures gap closure. |
| Relative Contraindications | Chronic tobacco use | Nicotine-induced microvascular vasoconstriction significantly increases the risk of wound dehiscence and flap necrosis. |
| Relative Contraindications | Advanced age / Sedentary lifestyle | The functional benefits of surgery do not outweigh the perioperative risks; conservative management yields acceptable ADL function. |
| Absolute Contraindications | Severe Peripheral Arterial Disease (PAD) | Inadequate vascularity to heal the posteromedial surgical incision; high risk of amputation. |
| Absolute Contraindications | Active local infection / Poor skin envelope | Incising through compromised skin guarantees deep space infection and hardware/suture contamination. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative clinical evaluation and meticulous surgical planning are the cornerstones of a successful Achilles tendon repair. The diagnosis is primarily clinical, anchored by a comprehensive physical examination. The pathognomonic Thompson test (calf squeeze test) must be performed; an absence of passive ankle plantarflexion upon squeezing the gastrocnemius muscle belly indicates a complete disruption of the musculotendinous unit. Additionally, the Matles test—observing the resting posture of the ankle with the patient prone and knees flexed to 90 degrees—is critical. A ruptured Achilles will demonstrate increased resting dorsiflexion compared to the contralateral intact limb. While clinical examination is usually sufficient, advanced imaging is utilized in equivocal cases or delayed presentations. Ultrasound is an excellent, cost-effective dynamic modality that can assess the gap size in real-time, though it is highly operator-dependent. Magnetic Resonance Imaging (MRI), specifically T2-weighted fat-suppressed sagittal and axial sequences, is the gold standard for defining the exact location of the tear, the degree of tendinosis, the extent of proximal retraction, and the presence of interposed degenerative tissue, which dictates the need for potential augmentation (e.g., V-Y advancement or turndown flaps).
Optimization of the patient in the holding area involves careful selection of anesthesia. While general anesthesia is frequently employed, regional anesthesia—specifically a spinal or epidural block—combined with a continuous popliteal sciatic nerve block provides profound intraoperative muscle relaxation and exceptional postoperative analgesia. This regional approach minimizes the systemic stress response and reduces the need for postoperative opioids, facilitating an accelerated discharge. Prior to positioning, a well-padded pneumatic tourniquet is applied to the proximal thigh of the operative leg. Exsanguination is achieved via gravity elevation or an Esmarch bandage, and the tourniquet is inflated to 250–300 mm Hg to ensure a bloodless surgical field, which is vital for identifying the delicate paratenon and sural nerve branches.
Patient positioning is a critical step that requires the coordinated effort of the surgical team. The patient is carefully log-rolled into the prone position onto a radiolucent operating table. Chest rolls (longitudinal bolsters from the clavicle to the iliac crest) are essential to allow free abdominal excursion, thereby preventing increased intra-abdominal pressure, which can impede venous return via the inferior vena cava and lead to increased epidural venous bleeding. The knees are typically padded, and the feet are allowed to hang freely over the edge of the bed, or the bed is flexed to allow 90 degrees of knee flexion. Prepping and draping must include the entire lower extremity from the toes to the mid-thigh. Crucially, the contralateral uninjured lower extremity must be prepped into the field or left accessible through a clear drape. This allows the surgeon to perform an intraoperative Matles test, directly comparing the resting equinus tension of the repaired tendon to the native contralateral side, ensuring precise restoration of the musculotendinous length.
Step-by-Step Surgical Approach and Fixation Technique
The open repair of the Achilles tendon is a meticulous procedure that demands strict adherence to tissue-handling principles. The primary goal is a biomechanically rigid repair that resists elongation, enveloped in a biologically viable soft tissue bed.
Incision and Deep Dissection
With the patient prone and the tourniquet inflated, the palpable defect in the tendon is identified. A longitudinal posteromedial incision, approximately 8 to 10 cm in length, is utilized. The incision is placed exactly 1 to 1.5 cm medial to the palpable medial border of the Achilles tendon. This medial bias is non-negotiable; it protects the laterally coursing sural nerve and prevents the surgical scar from lying directly over the posterior prominence of the tendon, thereby avoiding painful shoe-wear irritation postoperatively. The distal extent of the incision must terminate proximal to the shoe counter line.
Dissection proceeds sharply through the epidermis and dermis. The surgeon must absolutely avoid "skiving" or creating multiple subcutaneous planes. The subcutaneous fat must be taken down directly to the paratenon as a single, full-thickness fasciocutaneous flap. The vascular plexus supplying the skin resides within this delicate subcutaneous layer; undermining the skin edges will inevitably lead to ischemic necrosis and wound breakdown. Once the paratenon is identified, it is incised longitudinally in the midline. The paratenon is then carefully reflected medially and laterally, maintaining its continuity with the overlying subcutaneous tissues. The hematoma is evacuated, and the ruptured tendon ends are delivered into the wound. The ragged, "mop-end" fibrinous debris is sharply debrided back to healthy, parallel, glistening collagen fibers to optimize biological healing.
Primary Repair: The Krackow Locking Technique
The core principle of the primary repair is to establish a construct that can withstand early active range of motion. The Krackow locking stitch remains the biomechanical gold standard. Unlike simple grasping sutures that can pull through the longitudinally oriented collagen bundles under tension, the Krackow technique utilizes a series of locking loops that convert longitudinal pull into transverse compression, effectively "strangling" the tendon bundles and providing immense pull-out strength.
Using a heavy, ultra-high-molecular-weight polyethylene (UHMWPE) braided suture (e.g., #2 or #5 FiberWire, Orthocord, or HiFi), the surgeon places a running locking stitch along the medial and lateral borders of the proximal stump. Typically, 3 to 4 locking loops are placed on each side, progressing distally toward the rupture site. The process is then repeated on the distal stump, progressing proximally. Contemporary techniques often employ a 4-core or 6-core strand repair to maximize construct stiffness.
Once the core sutures are placed, the critical step of tensioning occurs. The knee is flexed to 90 degrees, and the ankle is placed in resting equinus (usually 15 to 25 degrees of plantarflexion) to match the contralateral limb. The sutures are tied securely with multiple square knots, ensuring the knots are buried within the rupture site to prevent subcutaneous irritation. A supplemental circumferential epitenon repair using a finer absorbable suture (e.g., 2-0 or 3-0 Vicryl) is performed using a running simple or cross-stitch technique. This "tidies" the repair site, minimizes bulk, and improves the gliding surface.
Gastrocnemius Flap Augmentation (Lindholm Technique)
In scenarios of delayed presentation, chronic ruptures with a substantial gap, or severe tendinosis where the primary repair is deemed biomechanically tenuous, augmentation is mandatory. The Lindholm technique utilizes vascularized turndown flaps from the proximal gastrocnemius aponeurosis. Through a proximal extension of the incision, the deep fascia is opened to expose the broad gastrocnemius aponeurosis.
Two parallel fascial flaps are fashioned from the aponeurosis, each approximately 1 to 1.5 cm wide and 7 to 8 cm long. The critical maneuver is to leave these flaps attached distally at a point exactly 3 cm proximal to the rupture site, preserving their distal vascular tether. Each flap is then twisted 180 degrees on its longitudinal axis. The biomechanical rationale for this twist is profound: it ensures that the smooth, external (anterior) surface of the aponeurosis faces outward toward the subcutaneous tissue, while the rough, cut surface faces inward against the tendon. This drastically reduces postoperative adhesions. The flaps are turned distally, bridging the defect, and sutured securely to the distal tendon stump and to each other, creating a robust, biological reinforcement sleeve.
Plantaris Tendon Augmentation (Lynn Technique)
An alternative and highly elegant augmentation strategy is the Lynn technique, which utilizes the autologous plantaris tendon. The plantaris is a vestigial structure present in approximately 90% of patients, located deep to the medial head of the gastrocnemius and running along the medial border of the Achilles tendon. Following the primary Krackow repair, the plantaris tendon is identified and harvested by dividing it distally near its calcaneal insertion, maximizing its length.
Using smooth forceps and a scalpel, the tubular plantaris tendon is meticulously teased apart and fanned out to form a broad, flat, biological membrane.
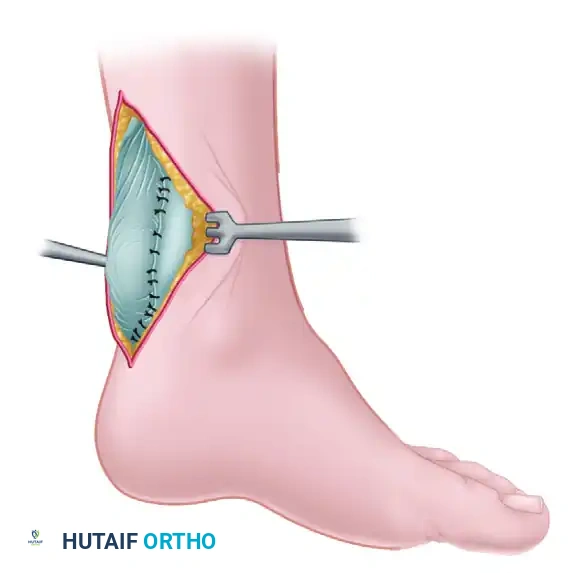
Figure 48-17A: Lynn technique for repairing a fresh rupture of the Achilles tendon. The ruptured Achilles tendon has been primarily sutured. The plantaris tendon has been divided distally and is being meticulously fanned out to form a broad autologous membrane.
This fanned-out autograft is then draped directly over the primary Achilles tendon repair site. It is sutured circumferentially to the epitenon using fine absorbable sutures.
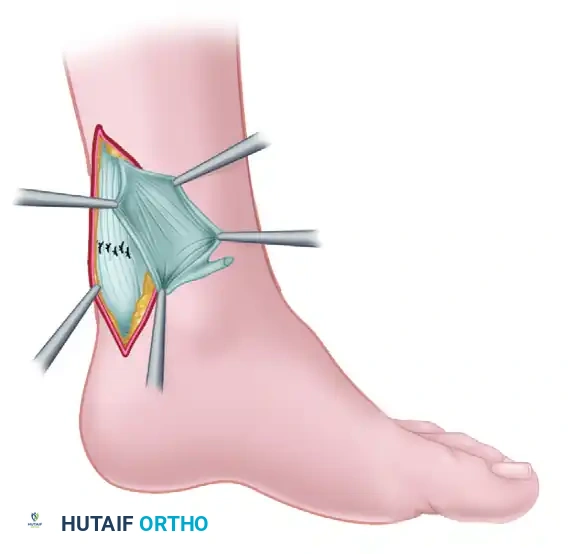
Figure 48-17B: The fanned-out plantaris tendon has been placed over the primary repair of the Achilles tendon and sutured securely in place, providing biological augmentation and a smooth gliding surface.
This plantaris membrane acts as a highly vascularized biological shield. It reinforces the mechanical strength of the repair, provides a rich scaffold for tenocyte migration and collagen cross-linking, and crucially, acts as an interpositional barrier preventing restrictive adhesions between the healing Achilles tendon and the overlying paratenon and skin. Following any repair or augmentation, the paratenon must be meticulously closed as a separate layer with 4-0 absorbable suture to restore the gliding envelope before standard skin closure.
Complications, Incidence Rates, and Salvage Management
The open repair of the Achilles tendon, while highly successful in restoring mechanical function, carries a distinct and unforgiving complication profile. The most dreaded and frequent complications are related to the tenuous soft tissue envelope of the posterior ankle. Superficial wound dehiscence and deep surgical site infections occur in approximately 2% to 5% of cases, but this rate climbs exponentially in patients with vasculopathy, diabetes, or those who smoke. The mechanism of failure is almost always ischemic necrosis of the skin edges due to aggressive subcutaneous undermining or excessive tension on the closure. When deep infection occurs, it threatens the entire repair construct and the viability of the limb.
Sural nerve injury is another significant complication, occurring in 1% to 3% of open repairs (and up to 10% in percutaneous repairs). This manifests as hyperesthesia, burning pain, or a frank neuroma along the lateral border of the foot. It is typically the result of straying laterally during the incision, blind clamping of bleeding veins in the posterolateral gutter, or incorporating the nerve into the locking suture loops. Intraoperative vigilance is the only reliable prevention.
Rerupture, while less common in open repairs compared to conservative management, still occurs in 2% to 4% of patients. It is almost universally tied to patient non-compliance during the early rehabilitation phase—specifically, premature weight-bearing without heel wedges, accidental slips resulting in sudden forced dorsiflexion, or returning to explosive sports before adequate biological remodeling has occurred (typically before 6 months). Finally, iatrogenic tendon elongation is a subtle but functionally devastating complication. If the surgeon fails to adequately tension the repair in resting equinus, the tendon heals in an elongated state. This alters the length-tension curve of the triceps surae, resulting in a permanent, unrecoverable loss of plantarflexion push-off power, leaving the patient with a persistent limp and inability to perform a single-leg heel raise.
| Complication | Estimated Incidence | Etiology / Mechanism | Salvage Management / Treatment Strategy |
|---|---|---|---|
| Superficial Wound Dehiscence | 3% - 5% | Ischemia of skin edges; excessive tension; early motion before skin healing. | Local wound care, strict immobilization, oral antibiotics if cellulitis is present. Usually heals by secondary intention. |
| Deep Space Infection / Necrosis | 1% - 2% | Contamination of hematoma; progression of superficial necrosis exposing the tendon. | Aggressive operative I&D, removal of non-absorbable sutures, IV antibiotics. May require Plastic Surgery for sural artery flap or free tissue transfer (ALT flap). |
| Sural Nerve Injury / Neuroma | 1% - 3% | Iatrogenic transection or entrapment in lateral suture passes. | Initial trial of gabapentinoids and desensitization. Refractory neuromas require surgical excision and burying the proximal nerve stump into the soleus muscle belly. |
| Tendon Rerupture | 2% - 4% | Sudden forced dorsiflexion event; premature removal of CAM boot wedges; biological failure. | Revision open surgery. Primary repair is rarely possible; requires V-Y advancement, turn-down flaps, or Flexor Hallucis Longus (FHL) tendon transfer. |
| Tendon Elongation / Weakness | 5% - 10% | Failure to tension the repair in adequate equinus; aggressive early passive stretching. | Extremely difficult to salvage. Custom AFO bracing. In severe cases, surgical shortening or FHL transfer to augment plantarflexion power. |
Phased Post-Operative Rehabilitation Protocols
The contemporary philosophy regarding Achilles tendon rehabilitation has undergone a paradigm shift. Historical protocols mandated 6 to 8 weeks of rigid cast immobilization, which inevitably led to profound calf atrophy, severe ankle stiffness, and disorganized collagen deposition. Modern evidence-based protocols emphasize early, controlled functional mobilization. The application of controlled mechanical stress stimulates tenocytes to align newly synthesized Type I collagen fibers along the axis of tension, significantly increasing the tensile strength and Young's modulus of the healing tendon.
Phase I: Maximum Protection and Biological Healing (Weeks 0–2)
Immediately postoperatively, the primary goal is wound healing and edema control. The patient is made strictly non-weight-bearing (NWB) with the assistance of crutches or a knee scooter. The operative limb is immobilized in a well-padded posterior splint or a short-leg cast. Crucially, the ankle is locked in 20 to 30 degrees of plantarflexion (gravity equinus) to eliminate any tension on the fresh surgical anastomosis. Strict elevation above the level of the heart is mandated to minimize venous congestion, which is a primary driver of wound dehiscence.
Phase II: Early Mobilization and Controlled Loading (Weeks 2–6)
At the two-week mark, assuming the surgical incision has healed impeccably, the sutures are removed. The patient is transitioned from the rigid splint into a removable controlled ankle motion (CAM) boot. To maintain the protective equinus, 2 to 3 solid heel wedges (providing roughly 20-30 degrees of plantarflexion) are placed inside the boot. Weight-bearing is progressively advanced from partial to full, as tolerated, while locked in the wedged boot. The hallmark of this phase is the initiation of early active range of motion. Out of the boot, the patient performs active plantarflexion and active-assisted dorsiflexion to neutral (0 degrees). Passive dorsiflexion is strictly and unequivocally prohibited, as it can stretch the immature collagen matrix and lead to irreversible tendon elongation.
Phase III: Progressive Strengthening and Normalization (Weeks 6–12)
During this phase, the heel wedges are sequentially removed from the CAM boot, typically at a rate of one wedge every 1 to 2 weeks, slowly bringing the ankle down to a neutral plantigrade position. By week 8 to 10, the patient is usually transitioned out of the CAM boot and into regular supportive footwear equipped with a small (1 cm) silicone heel lift to prevent sudden stretching. Physical therapy intensifies, focusing heavily on eccentric loading of the gastrocnemius-soleus complex, which has been shown to be the most effective stimulus for tendon remodeling. Proprioceptive training, utilizing BAPS boards and single-leg stance exercises, is commenced to restore neuromuscular control.
Phase IV: Advanced Function and Return to Sport (Months 4–6+)
The final phase focuses on plyometrics, dynamic multidirectional stability, and sport-specific training. Progression to jogging, jumping, and cutting maneuvers is allowed only when the patient demonstrates sufficient baseline strength. Return to competitive, explosive sports is never dictated by a strict timeline alone; it is a criteria-based decision. The patient must achieve a Limb Symmetry Index (LSI) of greater than 90% on functional testing—specifically the single-leg heel raise endurance test and hop testing—compared to the uninjured limb. They must also demonstrate full, pain-free range of motion and a complete absence of apprehension during dynamic loading.
Summary of Landmark Literature and Clinical Guidelines
The evolution of Achilles tendon rupture management is deeply rooted in robust clinical literature and randomized controlled trials. A pivotal turning point in the operative versus non-operative debate was the landmark randomized controlled trial by Willits et al. (JBJS Am, 2010). This study demonstrated that when an aggressive, early functional rehabilitation protocol is employed, the rerupture rates between operatively and non-operatively treated patients are statistically indistinguishable. This study fundamentally shifted the global paradigm, proving that the high rerupture rates historically associated with conservative management were largely a consequence of prolonged rigid immobilization rather than the absence of surgical sutures.
However, subsequent meta-analyses, such as the comprehensive review by Soroceanu et al. (JBJS Am, 2012), provided crucial nuance. While confirming that functional rehab mitigates rerupture risks in conservative groups, the data clearly showed that operative repair still provides a statistically significant advantage in restoring peak plantarflexion strength and allows for an earlier return to work and high-impact sports. Furthermore, operative repair significantly reduces the incidence of tendon elongation, a subtle but functionally limiting outcome often seen in non-operative cohorts.
The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines synthesize this vast body of literature. The guidelines strongly recommend shared decision-making, emphasizing that while both pathways are viable, open surgical repair remains the preferred modality for young, active patients, high-level athletes, and those with delayed presentations. The guidelines also issue a strong recommendation for the implementation of early functional mobilization protocols regardless of the initial treatment choice, cementing the principle that controlled mechanical loading is the ultimate driver of biological tendon healing.
