Mastering Open Reduction & Internal Fixation of Sacroiliac Joint & Sacrum
Key Takeaway
This masterclass guides orthopaedic fellows through open reduction and internal fixation of sacroiliac joint dislocations and sacral fractures. We cover essential surgical anatomy, meticulous preoperative planning, and granular, real-time intraoperative execution. Learn precise dissection, reduction maneuvers, and hardware placement, emphasizing fluoroscopic guidance and neurovascular protection. We also delve into critical pearls, pitfalls, and comprehensive postoperative management to optimize patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Posterior pelvic ring injuries represent some of the most formidable challenges encountered by the orthopedic trauma surgeon. These are not isolated, simple fractures; rather, they are the culmination of high-energy traumatic forces—such as motor vehicle collisions, motorcycle crashes, and falls from significant heights—that disrupt the foundational core of the human skeleton. The posterior pelvic ring, comprising the sacrum, sacroiliac (SI) joints, and the posterior ilium, serves as the critical keystone articulation linking the axial skeleton to the lower appendicular skeleton. Disruption of this complex not only compromises immediate mechanical stability but also carries a profound risk of long-term functional impairment, chronic pain, and severe disability if not meticulously managed.
The epidemiological profile of these injuries underscores their severity, with mortality rates historically ranging from 10% to a staggering 50% in cases of severe open pelvic fractures or those accompanied by massive hemodynamic instability. The immediate threat to life is typically hemorrhagic shock, driven by the rich, highly vascular presacral and paravesical venous plexuses, as well as potential arterial lacerations involving branches of the internal iliac system. Consequently, the initial management of these patients is strictly governed by Advanced Trauma Life Support (ATLS) protocols, emphasizing rapid hemodynamic resuscitation, pelvic volume reduction via mechanical binders, and, when necessary, pre-peritoneal packing or angioembolization before definitive orthopedic reconstruction can even be considered.
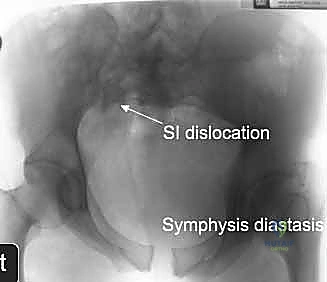
Once the patient is physiologically optimized, the focus shifts to the structural integrity of the pelvis. We broadly categorize pelvic ring injuries based on the vector of the deforming force and the resulting instability pattern, utilizing the Young-Burgess and Tile classification systems. Anterior injuries, such as symphyseal diastasis or pubic rami fractures, often serve as the "herald" lesions, pointing to a more sinister, hidden disruption posteriorly. The posterior lesions—iliac wing fractures, SI joint dislocations, crescent fractures, and sacral fractures—dictate the overall stability of the pelvic ring. A completely unstable hemipelvis, often seen in vertical shear (Tile C) injuries, exhibits both rotational and translational instability, demanding robust, multi-planar surgical fixation.
The evolution of pelvic trauma surgery has moved decisively away from prolonged recumbency and conservative management, which were historically plagued by catastrophic complications including deep vein thrombosis, pulmonary embolism, decubitus ulcers, and devastating malunions. Today, the standard of care for displaced, unstable posterior pelvic ring injuries is anatomic reduction and rigid internal fixation. Our focus in this definitive chapter is to dissect the nuances of operative intervention for displaced sacral fractures and highly unstable SI joint disruptions, providing the orthopedic surgeon with the advanced anatomical knowledge, preoperative planning strategies, and technical mastery required to execute these complex procedures safely and effectively.
Detailed Surgical Anatomy and Biomechanics
Osteology and the Articular Keystone
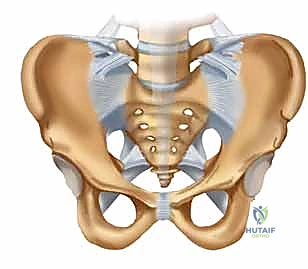
To master the surgical management of the posterior pelvis, one must possess an intimate, three-dimensional understanding of its osteology. The pelvic ring is a true biomechanical circle, formed by the paired innominate bones anteriorly and laterally, and the sacrum posteriorly. Each innominate bone is an embryological fusion of three distinct ossification centers: the ilium, the ischium, and the pubis, which converge at the triradiate cartilage within the acetabulum.
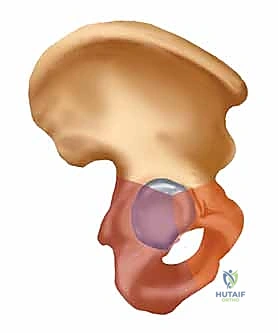
The sacrum functions as the terminal structural segment of the spinal column and the central keystone of the pelvic arch. It is typically composed of five fused sacral vertebrae, possessing a kyphotic curve that is highly variable among individuals. The lateral masses of the sacrum, or alae, articulate with the medial articular surfaces of the ilia to form the sacroiliac joints. The SI joint itself is a unique, diarthrodial joint with a complex topography; the sacral side is covered by thick hyaline cartilage, while the iliac side is lined with thinner fibrocartilage. The articular surfaces are not smooth but feature interlocking ridges and depressions that contribute to inherent bony stability, a concept known as form closure.

Biomechanically, when axial loads are transmitted from the spine through the sacrum to the lower extremities, the natural tendency is for the sacrum to flex (nutate) and displace inferiorly, while the hemipelves tend to externally rotate and translate cephalad. Because there are no dynamic muscular stabilizers that cross the SI joint to prevent this displacement, the pelvis relies entirely on its interlocking bony architecture and a massive, intricate network of static ligamentous restraints. Understanding this transmission of forces is paramount when selecting implants, as the fixation construct must neutralize these specific deforming vectors until bony union or ligamentous healing occurs.
The Ligamentous Complex: Primary Static Stabilizers
The ligamentous anatomy of the posterior pelvic ring is arguably the most robust in the human body, specifically evolved to withstand massive physiological loads. The sacroiliac ligaments are divided into anterior, interosseous, and posterior components. The anterior SI ligaments are relatively thin, flat bands that resist external rotation and anterior diastasis of the hemipelvis; they are often the first to tear in anteroposterior compression (APC) injuries. However, it is the posterior and interosseous ligamentous complexes that are the true workhorses of pelvic stability.
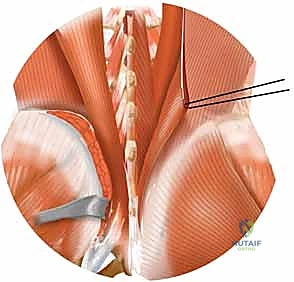
The interosseous sacroiliac ligaments are massive, short, and dense fibers connecting the sacral and iliac tuberosities deep within the joint space. They are the primary barrier against cephalad and posterior translation of the ilium relative to the sacrum. Superficial to these lie the posterior sacroiliac ligaments, which blend with the origins of the multifidus and erector spinae musculature. These ligaments are taut in sacral nutation and provide critical resistance against vertical shear forces.
Further reinforcing the pelvic floor and resisting rotational instability are the sacrotuberous and sacrospinous ligaments. The sacrotuberous ligament courses from the posterior iliac spines and lateral sacrum down to the ischial tuberosity, resisting sacral flexion. The sacrospinous ligament, lying deep to the sacrotuberous, connects the lateral margin of the sacrum and coccyx to the ischial spine. Together, these ligaments form a powerful tension band that prevents the hemipelvis from rotating outward and migrating proximally. In severe pelvic ring disruptions, surgical reduction must overcome the contracted remnants of these ligaments or, conversely, restore their anatomical tension to achieve a stable construct.
Neurovascular Danger Zones
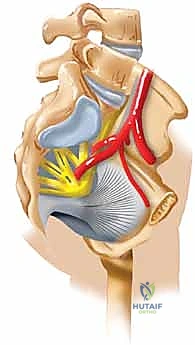
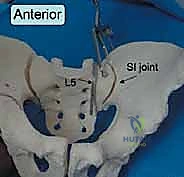
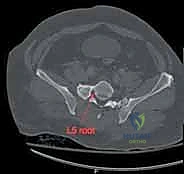
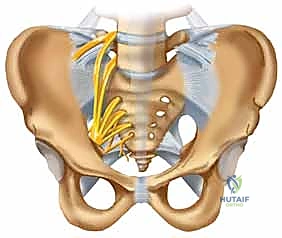
Surgical intervention in the posterior pelvic ring is fraught with hazard due to the intimate proximity of critical neurovascular structures. Meticulous dissection and precise implant placement are non-negotiable. The L5 nerve root is perhaps the most vulnerable structure during posterior pelvic fixation. It courses anteriorly and inferiorly over the superior aspect of the sacral ala, lying directly in the path of an errantly placed extra-osseous iliosacral screw.

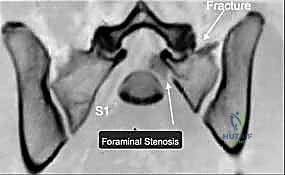
Any hardware placed too superiorly or anteriorly into the S1 body risks compressing or lacerating this nerve root, leading to devastating motor deficits, particularly a foot drop due to tibialis anterior weakness, and sensory loss over the dorsum of the foot. Furthermore, the sacral plexus, formed by the lumbosacral trunk (L4, L5) and the ventral rami of S1-S4, lies immediately anterior to the sacral body. Over-penetration of the anterior sacral cortex during drilling or screw insertion can cause catastrophic damage to these nerves, resulting in permanent bowel, bladder, and sexual dysfunction.
Vascularly, the superior gluteal artery and nerve represent a significant danger zone during posterior approaches. These structures exit the pelvis through the greater sciatic foramen, passing superior to the piriformis muscle, immediately lateral and inferior to the SI joint.
During extensive posterior soft tissue stripping, or when applying reduction clamps (such as a Jungbluth clamp) to the posterior ilium, the superior gluteal neurovascular bundle is at high risk of iatrogenic injury. Laceration of the superior gluteal artery can result in massive, difficult-to-control hemorrhage, as the proximal stump often retracts deep into the pelvis. Surgeons must maintain a healthy respect for the sciatic notch and avoid blind clamp placement or excessive inferior dissection along the posterior iliac border.
Osteology and Segmentation Anomalies
A critical, yet historically underappreciated, aspect of pelvic trauma surgery is the prevalence of sacral dysmorphism and segmentation anomalies. Up to 30-40% of the normal population exhibits some degree of upper sacral dysmorphism, which drastically alters the safe osseous corridors available for internal fixation. Most commonly, this presents as a transitional lumbosacral vertebra—either a sacralized L5 or a lumbarized S1.
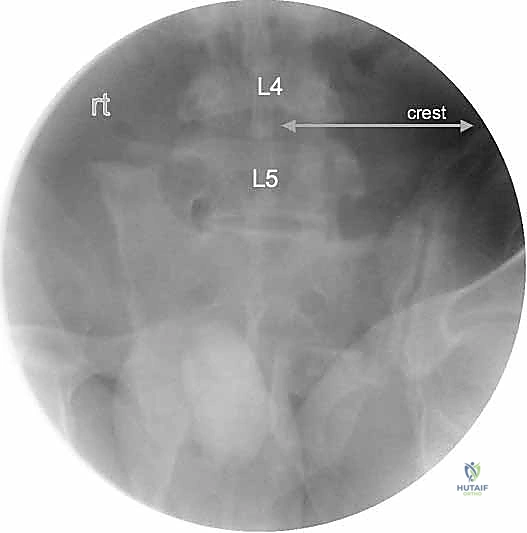
In a dysmorphic sacrum, the upper sacral segment (often referred to as the "transitional" segment) is not recessed within the pelvis but sits relatively high, often colinear with the iliac crests. The alar slope is acutely angled anteriorly and inferiorly, and the safe osseous corridor for an S1 iliosacral screw is significantly constricted in both the axial and coronal planes. Furthermore, the neural foramina are often distorted, and residual disc spaces may exist between the upper sacral segments.
Failure to recognize a dysmorphic pelvis on preoperative imaging is a primary cause of iatrogenic nerve injury and hardware misplacement. Standard orthogonal fluoroscopy is often misleading in these patients. Surgeons must rely heavily on preoperative CT templating to identify these anomalies. In cases of severe S1 dysmorphism, the S1 corridor may be entirely unsafe for screw placement, mandating the use of the S2 corridor, which, while smaller, is typically more consistently shaped and orthogonal to the ilium, or alternative fixation methods such as lumbopelvic spinal constructs.
Exhaustive Indications and Contraindications
The decision to proceed with operative fixation of the posterior pelvic ring requires a nuanced synthesis of the patient's physiological status, the biomechanical instability of the fracture pattern, and the local soft tissue envelope. Not all pelvic fractures require surgery; stable, minimally displaced injuries (e.g., Tile Type A, isolated pubic rami fractures, or non-displaced lateral compression injuries) are often managed successfully with protected weight-bearing and aggressive physical therapy. However, when the structural integrity of the pelvic ring is compromised, operative intervention becomes mandatory to restore anatomy and permit early mobilization.
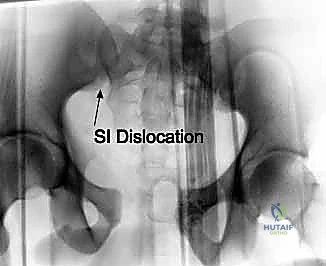
The primary indication for open reduction and internal fixation (ORIF) or percutaneous fixation is mechanical instability. This is clinically and radiographically evident in injuries with significant displacement (typically defined as >1 cm of posterior translation or cephalad migration), complete disruption of the posterior ligamentous complex (Tile Type C / vertical shear injuries), or highly unstable open-book (APC-III) injuries. Furthermore, any progressive deformity noted on serial radiographs during a trial of non-operative management warrants immediate surgical stabilization.
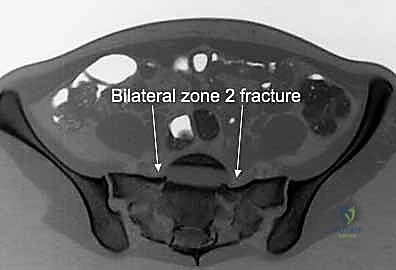
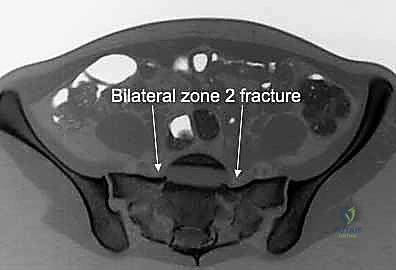
Neurologic compromise secondary to sacral fractures or SI joint fracture-dislocations is a compelling, often urgent, indication for surgery. Entrapment of the sacral nerve roots within a displaced sacral foraminal fracture (Denis Zone II) or compression of the lumbosacral trunk by a displaced sacral ala can lead to profound deficits. In these scenarios, surgical intervention is not merely for mechanical stability, but to perform a meticulous neural decompression, remove impinging bone fragments, and stabilize the fracture to prevent ongoing dynamic nerve injury. Open pelvic fractures, though rare, represent absolute surgical emergencies requiring immediate aggressive debridement, copious irrigation, and temporary or definitive stabilization to mitigate the exceptionally high risk of sepsis.
Contraindications to definitive pelvic reconstruction are primarily physiological. Hemodynamically unstable patients in extremis are not candidates for lengthy, complex pelvic reconstructions. These patients require "damage control" orthopedics—application of external fixators, pelvic binders, and pre-peritoneal packing to arrest hemorrhage and stabilize the bony volume until physiological reserve is restored. Additionally, a severely compromised posterior soft tissue envelope, such as a massive Morel-Lavallée lesion (a closed degloving injury) over the lumbosacral region, is a strong relative contraindication to open posterior approaches due to the exorbitant risk of deep surgical site infection and wound necrosis. In such cases, percutaneous techniques or delayed open surgery after soft tissue resolution must be employed.
| Parameter | Indications for Operative Fixation | Contraindications (Absolute & Relative) |
|---|---|---|
| Mechanical | Posterior displacement > 1cm; Vertical shear (Tile C); Unstable APC III; Progressive deformity. | Stable, non-displaced fractures (Tile A); Impacted LC-I injuries with intact posterior hinge. |
| Neurological | Sacral nerve root entrapment; Progressive neurologic deficit; Lumbosacral trunk compression. | Pre-existing, non-traumatic profound paralysis (relative, depending on goals of care). |
| Physiological | Hemodynamically stable patient; Optimized polytrauma patient. | Hemodynamic instability (Damage Control only); Severe coagulopathy; Refractory shock. |
| Soft Tissue | Intact, healthy overlying skin; Open fractures requiring debridement. | Massive Morel-Lavallée lesion (relative for open approaches); Active local infection. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Diagnostic Studies
Meticulous preoperative planning is the absolute cornerstone of successful posterior pelvic ring surgery. The margin for error is measured in millimeters, and navigating the complex, three-dimensional anatomy requires a comprehensive imaging strategy. The standard plain radiographic trauma series remains the initial step. An anteroposterior (AP) pelvis view provides a global overview, allowing for side-to-side comparison of the iliac crests, sacral foramina, and pubic symphysis.

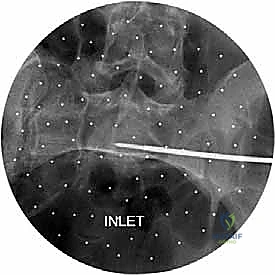
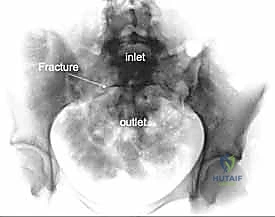
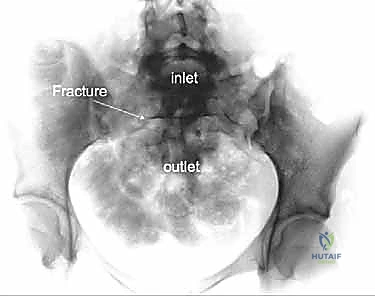
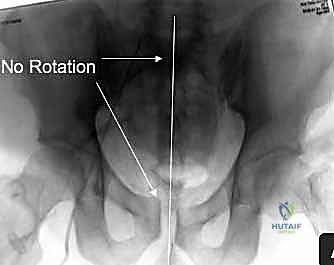
However, the AP view alone is vastly insufficient for assessing posterior displacement. The Inlet view, obtained by directing the X-ray beam 45 degrees caudally, is essential for evaluating anterior-posterior translation, internal/external rotational deformity of the hemipelvis, and the presence of sacral impaction fractures.
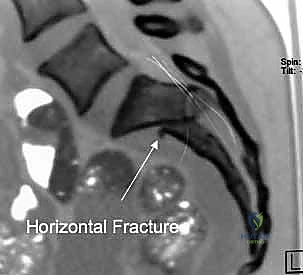
The Outlet view, directed 45 degrees cephalad, provides an en face projection of the sacrum. This view is critical for diagnosing cephalad (vertical) migration of the hemipelvis, assessing flexion/extension deformities of the sacrum, and visualizing the sacral neural foramina to identify transforaminal fracture lines.
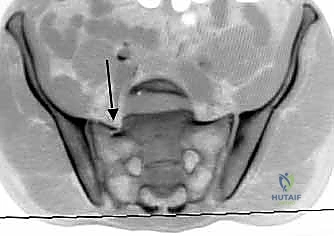
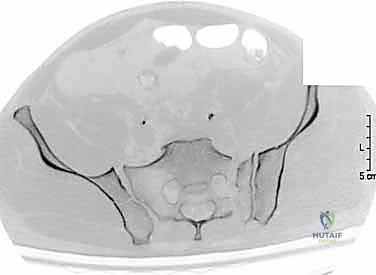
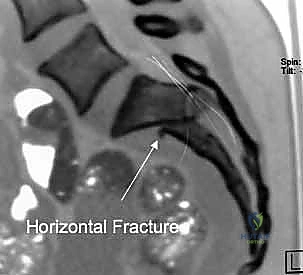
While plain films are fundamental, high-resolution Computed Tomography (CT) is the gold standard and an absolute prerequisite for operative planning. Fine-cut (1-2mm) axial, coronal, and sagittal reconstructions are mandatory. The CT scan allows the surgeon to precisely delineate the fracture geometry, assess the size and comminution of sacral fragments, and identify intra-articular debris within the SI joint. Furthermore, 3D reconstructions provide an unparalleled spatial understanding of the injury pattern, aiding in the conceptualization of reduction vectors.
Templating and Safe Zone Identification
Once the imaging is acquired, the surgeon must engage in rigorous preoperative templating. This involves identifying the "safe zones" for hardware placement, primarily for iliosacral or transsacral screws. Using the axial and coronal CT cuts, the surgeon measures the dimensions of the S1 and S2 osseous corridors. The safe zone is defined anteriorly by the sacral promontory and anterior cortex, posteriorly by the sacral spinal canal, superiorly by the L5/S1 disc space (or the L5 nerve root), and inferiorly by the S1 neural foramen.
In a normal pelvis, the S1 corridor is typically large enough to accommodate one or two 7.0mm or 7.3mm cannulated screws. However, in the presence of sacral dysmorphism, as previously discussed, this corridor may be critically narrowed or entirely absent. The surgeon must measure the exact angle of the safe trajectory relative to the true horizontal and coronal planes of the pelvis. This templated angle will guide the intraoperative fluoroscopic views and the trajectory of the guide wire. If the S1 corridor is deemed unsafe, the templating process is repeated for the S2 body, which, while smaller in cross-sectional area, is often more predictable in dysmorphic patients.
Patient Positioning and Fluoroscopic Setup
The choice of patient positioning—supine versus prone—is dictated by the specific injury pattern, the planned surgical approach, and the necessity for concurrent anterior ring fixation. The supine position is frequently utilized for percutaneous iliosacral screw fixation, particularly when combined with anterior symphyseal plating or retrograde pubic rami screws. It allows for excellent airway access and simultaneous management of intra-abdominal or thoracic injuries. A radiolucent flat Jackson table is highly recommended to facilitate unobstructed fluoroscopic imaging.
Conversely, the prone position is preferred when direct open reduction of the posterior ring is required, such as in highly comminuted sacral fractures requiring decompression, complex SI joint fracture-dislocations needing direct visualization, or when utilizing lumbopelvic spinal fixation techniques. Prone positioning allows gravity to assist in reducing cephalad displacement and provides direct access to the posterior ilium for the application of reduction clamps.

Regardless of the position, the fluoroscopic setup is critical. Before prepping and draping, the surgeon must ensure that perfect Inlet, Outlet, and true lateral views of the sacrum can be obtained without obstruction from the table or the patient's contralateral anatomy. The C-arm must be highly mobile, and the technician must be briefed on the specific angles required, which were determined during the preoperative templating phase. The inability to obtain crisp, orthogonal fluoroscopic images is an absolute contraindication to percutaneous posterior pelvic fixation.
Step-by-Step Surgical Approach and Fixation Technique
Surgical Approaches to the Posterior Ring
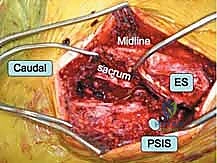
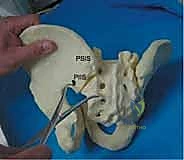
When closed or percutaneous reduction maneuvers fail, or when direct neural decompression is mandated, an open approach to the posterior pelvic ring is required. The most common approaches are the posterior midline approach and the paramedian (lateral to the posterior superior iliac spine - PSIS) approach. The midline approach provides excellent bilateral access to the sacrum for lumbopelvic fixation or transsacral plating. However, it requires significant subcutaneous dissection to reach the SI joints, increasing the risk of dead space formation and postoperative wound complications.
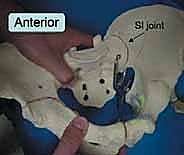
The paramedian approach, typically an incision made approximately 2-3 cm lateral to the PSIS and curving distally, offers direct, targeted access to the SI joint and the posterior ilium. The gluteus maximus is split in line with its fibers or elevated off the posterior ilium. This approach is ideal for applying pelvic reduction clamps, visualizing the posterior aspect of the SI joint to clear interposed tissue, and placing posterior tension band plates. Extreme care must be taken during the inferior dissection to avoid the superior gluteal neurovascular bundle exiting the sciatic notch.
For injuries involving the anterior aspect of the SI joint or the sacral ala (e.g., crescent fractures), a lateral window of the ilioinguinal approach or an anterior intrapelvic (modified Stoppa) approach may be utilized. These anterior approaches allow for direct visualization of the anterior SI joint and the application of anterior plates, avoiding the high wound complication rates associated with posterior incisions, though they carry their own risks regarding the external iliac vessels and the lumbosacral trunk.
Reduction Maneuvers: Restoring the Keystone
Anatomic reduction of the posterior ring is the most challenging and critical step of the procedure. Malreduction, particularly residual vertical displacement or internal rotation, leads to altered gait biomechanics, chronic pain, and a high risk of hardware failure. Reduction is achieved through a combination of skeletal traction, manual manipulation, and the strategic use of specialized pelvic reduction instruments.

Schanz pins (5.0mm or 6.0mm) placed percutaneously into the dense bone of the posterior iliac crests serve as excellent "joysticks." These allow the surgeon to manipulate the hemipelvis in multiple planes, correcting rotational and translational deformities. For vertical shear injuries, skeletal traction applied via a distal femoral pin can assist in pulling the hemipelvis distally. Once gross alignment is achieved, specialized clamps are utilized for fine-tuning and provisional stabilization.
The Jungbluth clamp, applied to screws placed in the posterior ilium and the sacrum, is incredibly powerful for reducing SI joint dislocations. Alternatively, a large Weber pointed reduction clamp can be placed across the SI joint, with one tine on the sacrum and the other on the ilium, to compress the joint. Throughout the reduction process, continuous fluoroscopic imaging in the Inlet and Outlet planes is mandatory to verify the correction of all deforming vectors. The reduction must be anatomically perfect before any definitive hardware is introduced.
Definitive Fixation: Iliosacral Screws and Beyond
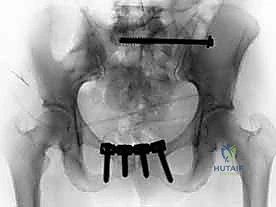
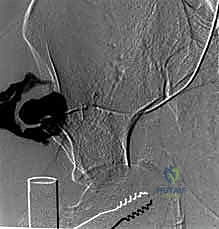
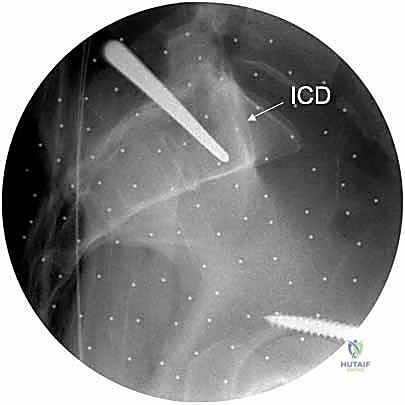
The workhorse of posterior pelvic ring fixation is the iliosacral screw. Once anatomic reduction is confirmed, a guide wire is advanced from the lateral aspect of the ilium, across the SI joint, and into the sacral body. The trajectory is meticulously guided by alternating Inlet and Outlet fluoroscopic views. The Inlet view ensures the wire remains within the anterior-posterior confines of the sacral body, avoiding the spinal canal and the anterior cortex.
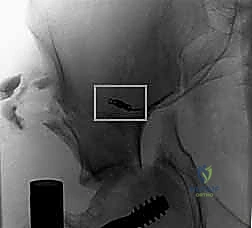
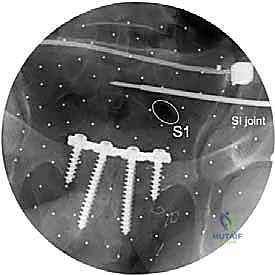
The Outlet view confirms the superior-inferior trajectory, ensuring the wire passes safely between the upper sacral endplate and the S1 neural foramen. A true lateral view of the sacrum is also highly recommended to verify the wire's position relative to the alar slope and the sacral promontory. Once the wire is perfectly positioned, a cannulated drill is used, and a large-fragment (typically 7.3mm) partially threaded screw is inserted to provide compression across the SI joint. For pure SI dislocations, two screws are often placed to prevent rotational toggling.
In cases of highly unstable vertical shear injuries, bilateral sacral fractures, or poor bone quality, transsacral-transiliac screws offer vastly superior biomechanical stability. These screws traverse the entire width of the pelvis, passing from one ilium, through the sacral body, and into the contralateral ilium. This construct acts as a robust internal tie-rod, neutralizing both vertical and rotational forces far more effectively than unilateral iliosacral screws.

When the sacrum is severely comminuted (e.g., U-type or H-type spinopelvic dissociations) or when the osseous corridors are too narrow for screw fixation, lumbopelvic fixation (triangular osteosynthesis) is the definitive salvage technique. This involves placing pedicle screws in the lower lumbar vertebrae (L4, L5) and long iliac screws traversing the posterior superior iliac spine down toward the supra-acetabular corridor. These are connected by rigid rods, effectively bypassing the shattered sacrum and transferring the axial load directly from the lumbar spine to the intact ilium.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique and advanced imaging, surgery of the posterior pelvic ring is associated with a formidable complication profile. The high-energy nature of the initial trauma, combined with the complex regional anatomy and the necessity for extensive surgical exposure, creates a perfect storm for potential adverse events. The orthopedic surgeon must be acutely aware of these risks, employ aggressive preventative strategies
Clinical & Radiographic Imaging Archive