Mastering Femoral Head Fracture Repair at the Base of the Femoral

Key Takeaway
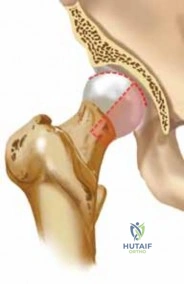
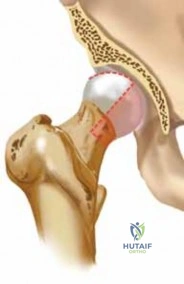
For anyone wondering about Mastering Femoral Head Fracture Repair at the Base of the Femoral, Femoral head fractures are rare, high-energy injuries associated with hip dislocations (5-15% of cases), often resulting in shearing damage to articular cartilage. Blood supply to the superior dome of the femoral head, originating from the base of the femoral, primarily involves the medial femoral circumflex artery traveling around the proximal femur and penetrating the joint capsule.
Introduction and Epidemiology
Fractures of the femoral head are rare but severe injuries that occur almost exclusively in the setting of high-energy trauma, most notably associated with hip fracture-dislocations. Epidemiological data indicate that femoral head fractures are present in approximately 5% to 15% of all posterior hip dislocations. Because of the extreme force required to induce a fracture-dislocation of the native hip joint, these injuries are frequently seen in motor vehicle collisions, specifically in "dashboard injuries" where an axial load is applied to a flexed knee, transmitting force directly along the femoral shaft to the hip joint.

The pathogenesis of these shearing injuries is heavily dictated by the position of the lower extremity at the exact moment of impact, combined with the patient’s intrinsic hip morphology. Posterior dislocations, which represent the vast majority of these injuries, occur when the hip is subjected to an axial load while in a flexed, adducted, and internally rotated position. Decreased femoral anteversion further diminishes the anterior coverage of the femoral head by the acetabulum, thereby increasing the susceptibility to posterior dislocation and subsequent shearing against the posterior acetabular wall.

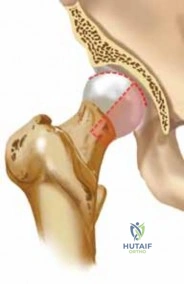
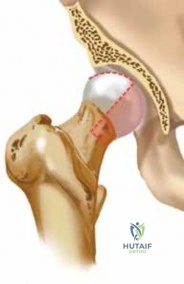
The Pipkin classification remains the standard for categorizing femoral head fractures and guiding surgical decision-making. Type I involves a fracture below the fovea capitis (the non-weight-bearing portion). Type II involves a fracture extending above the fovea capitis (the primary weight-bearing dome). Type III is any femoral head fracture associated with a femoral neck fracture, carrying an exceptionally high risk of avascular necrosis. Type IV is a femoral head fracture associated with an acetabular fracture, usually involving the posterior wall.
Surgical Anatomy and Biomechanics
A profound understanding of the proximal femoral vascular anatomy is paramount when managing femoral head fractures, as iatrogenic disruption of the residual blood supply can precipitate avascular necrosis (AVN) of the femoral head. The spherical femoral head is almost completely covered by articular hyaline cartilage, which is frequently contused, scored, or sheared during the dislocation event.

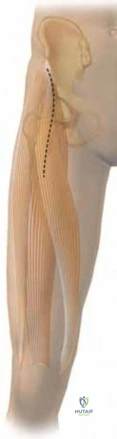
The primary vascular supply to the superior dome and the majority of the femoral head is derived from the medial femoral circumflex artery (MFCA). The deep branch of the MFCA travels posterior to the proximal femur, passing deep to the quadratus femoris muscle. It then courses superiorly and anteriorly to penetrate the posterior joint capsule just inferior to the piriformis tendon, giving rise to the superior retinacular vessels.
Additional, albeit minor, vascular contributions arise from the lateral femoral circumflex artery (supplying the anterior-inferior neck) and the foveal artery (a branch of the obturator artery traveling within the ligamentum teres). The foveal artery's contribution is variable and generally insufficient to maintain femoral head viability if the retinacular vessels are compromised.

Crucially, the anterior half of the femoral neck is largely devoid of critical vascular structures. This anatomic reality dictates that anterior surgical approaches to the hip joint (such as the Smith-Petersen or Hueter approaches) do not compromise the primary vascular supply of the femoral head, making them advantageous for isolated anterior femoral head fracture fixation. The acetabular labrum, which deepens the socket and provides a fluid seal, is frequently avulsed or torn during the dislocation and must be assessed during surgical intervention.
Indications and Contraindications
The primary goal of treatment is to achieve a concentric, stable reduction of the hip joint while restoring the articular congruency of the femoral head. Emergent closed reduction of the dislocated hip is the universal first step. Once the hip is reduced, the decision to proceed with operative versus non-operative management depends on the fracture pattern, fragment size, degree of displacement, and the presence of intra-articular incarcerated fragments.
| Parameter | Operative Indications | Non-Operative Indications |
|---|---|---|
| Pipkin Type I | Displaced >1-2 mm, or presence of intra-articular loose bodies preventing concentric reduction. | Non-displaced or minimally displaced (<1 mm step-off) with a perfectly congruent joint post-reduction. |
| Pipkin Type II | Nearly all cases require Open Reduction and Internal Fixation (ORIF) due to involvement of the weight-bearing dome. | Extremely rare; only considered in strictly non-displaced fractures in non-ambulatory patients. |
| Pipkin Type III | Absolute indication for surgery. Often requires Arthroplasty in older patients or precise ORIF in young patients. | None. High risk of nonunion and avascular necrosis. |
| Pipkin Type IV | Absolute indication for surgery to address both the femoral head and acetabular wall fractures. | None. |
| Joint Congruency | Incongruent joint space on post-reduction CT scan; retained osteochondral fragments. | Concentric reduction confirmed on fine-cut CT scan with no interposed tissue or bone. |
| Patient Status | Medically optimized for major orthopedic trauma surgery. | Medically unstable patients; polytrauma patients in extremis (damage control orthopedics applies). |
Contraindications to immediate open reduction and internal fixation include severe hemodynamic instability, active systemic infection, or severe pre-existing osteoarthritis of the affected hip, in which case a primary total hip arthroplasty (THA) may be more appropriate than osteosynthesis, particularly in the geriatric population.

Pre Operative Planning and Patient Positioning
Because of the high energy required to induce a fracture-dislocation of the hip, all patients must undergo a rigorous Advanced Trauma Life Support (ATLS) evaluation. Airway, cardiovascular, thoracic, and visceral injuries take precedence and must be stabilized emergently.

The initial orthopedic evaluation begins with a trauma anteroposterior (AP) pelvis radiograph. The immediate goal is the emergent closed reduction of the hip joint in the emergency department, ideally within 6 hours of injury, to minimize the risk of avascular necrosis. Following a successful closed reduction, a dedicated fine-cut computed tomography (CT) scan of the pelvis and bilateral hips is mandatory.
The CT scan provides critical information regarding the size and location of the femoral head fragment, the presence of marginal impaction or posterior wall acetabular fractures (Pipkin IV), and the identification of small, incarcerated intra-articular osteochondral fragments that may block concentric reduction.
Careful physical examination must document the preoperative neurological status. Because sciatic nerve injuries (particularly the peroneal division) are common with posterior dislocations, motor and sensory examination of the affected extremity is critical. Strength grades (1–5) for ankle dorsiflexion, plantar flexion, and extensor hallucis longus function must be recorded.

Patient positioning is dictated by the chosen surgical approach.
* For an Anterior (Smith-Petersen) Approach, the patient is positioned supine on a radiolucent flat Jackson table or a standard operating table. A bump may be placed under the ipsilateral hemipelvis.
* For a Posterior (Kocher-Langenbeck) Approach or a Surgical Dislocation (Ganz) Approach, the patient is placed in the lateral decubitus position using a peg board or bean bag. The operative leg must be draped free to allow for full manipulation, dislocation, and reduction during the procedure.
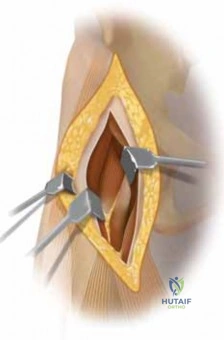
Detailed Surgical Approach and Technique
The choice of surgical approach is one of the most debated topics in orthopedic traumatology regarding femoral head fractures. The decision hinges on the location of the fracture fragment (anterior vs. posterior), the presence of associated acetabular fractures, and the surgeon's familiarity with complex hip exposures.
Anterior Approach via Smith Petersen
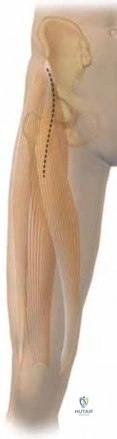
The anterior approach utilizes the internervous plane between the femoral nerve (sartorius, rectus femoris) and the superior gluteal nerve (tensor fasciae latae, gluteus medius). This approach is highly favored for isolated femoral head fractures (Pipkin I and II) because the anterior hip capsule is incised, avoiding the delicate posterior retinacular blood supply provided by the MFCA.

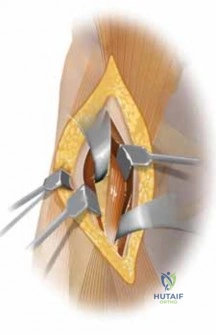
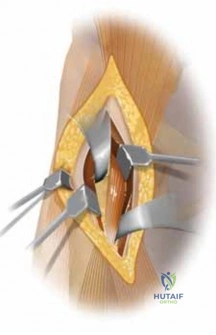
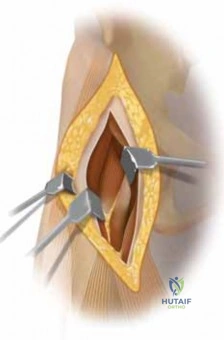
An incision is made starting at the anterior superior iliac spine (ASIS) and extending distally toward the lateral patella. The superficial dissection separates the sartorius and TFL. The deep dissection separates the rectus femoris and the gluteus medius. The ascending branch of the lateral femoral circumflex artery is identified and ligated. The reflected head of the rectus femoris may be detached from the anterior joint capsule. A T-shaped or I-shaped capsulotomy is performed, exposing the anterior femoral head and neck. This provides excellent visualization of the fracture site for direct reduction and fixation.
Surgical Dislocation of the Hip
The Ganz surgical dislocation approach is an elegant and highly effective technique that provides 360-degree visualization of the femoral head and acetabulum while meticulously preserving the MFCA blood supply. It is increasingly becoming the gold standard for complex Pipkin fractures.
The patient is in the lateral decubitus position. A straight lateral incision is made over the greater trochanter. The fascia lata is split, and a trochanteric flip osteotomy is performed. A stepped osteotomy of the greater trochanter (leaving the gluteus medius and minimus attached to the mobile fragment, and the vastus lateralis attached distally) is executed. The trochanteric fragment is flipped anteriorly.

The capsule is approached via the interval between the piriformis and gluteus minimus. A Z-shaped capsulotomy is performed. The hip is then surgically dislocated anteriorly by externally rotating and flexing the leg. This maneuver safely protects the posterior retinacular vessels, which remain relaxed and intact. The entire femoral head can be inspected, and precise articular reduction can be achieved.

Posterior Approach via Kocher Langenbeck
The posterior approach is primarily indicated when a femoral head fracture is associated with a posterior wall acetabular fracture (Pipkin IV). It does not provide adequate visualization of anteriorly displaced femoral head fragments without performing an iatrogenic surgical dislocation, which, if done through a posterior approach, carries a significant risk of stretching and tearing the remaining intact MFCA branches.
The patient is positioned prone or lateral. The incision is centered over the greater trochanter, curving posteriorly toward the posterior superior iliac spine (PSIS). The gluteus maximus is split in line with its fibers. The short external rotators (piriformis, obturator internus, superior/inferior gemelli) are identified, tagged, and released near their femoral insertions, protecting the sciatic nerve medially. The posterior capsule is incised to expose the posterior wall and the joint space.

Fracture Reduction and Fixation Techniques
Once the fracture is exposed, the joint is thoroughly irrigated to remove hematoma and small cartilaginous debris. Small, non-articular fragments or highly comminuted fragments that do not contribute to joint stability are excised.

For fixable fragments, anatomic reduction is achieved using pointed reduction forceps or dental picks. Provisional fixation is obtained with smooth Kirschner wires. Definitive fixation is typically achieved using multiple 2.0 mm, 2.4 mm, or 3.0 mm headless compression screws. It is absolutely critical that the screw heads are countersunk at least 1 to 2 millimeters beneath the articular cartilage surface to prevent devastating iatrogenic scoring of the acetabular cartilage during hip range of motion.
Alternatively, bioabsorbable pins (e.g., poly-L-lactic acid or polyglycolic acid) can be utilized, particularly for smaller fragments. These obviate the need for future hardware removal but may be associated with sterile sinus tract formation or osteolysis in some patients. After fixation, the hip is taken through a full range of motion under direct visualization to ensure stability, absence of impingement, and confirmation that hardware is not prominent.
Complications and Management
The management of femoral head fractures is fraught with high complication rates, largely due to the initial high-energy trauma and the precarious vascular supply of the proximal femur.

| Complication | Estimated Incidence | Etiology and Pathogenesis | Management and Salvage Strategies |
|---|---|---|---|
| Avascular Necrosis (AVN) | 10% - 30% | Disruption of the medial femoral circumflex artery during the initial trauma or iatrogenically during surgical exposure. | Early stages: Core decompression, bisphosphonates. Late stages (collapse): Total Hip Arthroplasty (THA). |
| Post-Traumatic Osteoarthritis | 20% - 50% | Initial chondral shear injury at the time of dislocation; incongruent joint reduction; prominent hardware. | Non-operative: NSAIDs, activity modification, intra-articular injections. Operative: THA or hip arthrodesis in very young laborers. |
| Heterotopic Ossification (HO) | 20% - 40% | Soft tissue trauma, muscle stripping (especially in the anterior or extensile approaches). | Prophylaxis is key (Indomethacin for 3-6 weeks or single-dose localized radiation). Excision indicated only if mature and mechanically blocking motion. |
| Sciatic Nerve Palsy | 10% - 20% | Traction or direct contusion during posterior dislocation; iatrogenic retraction injury during the posterior approach. | Most are neuropraxias that resolve spontaneously over 3-12 months. Ankle-foot orthosis (AFO) for foot drop. Surgical exploration rarely indicated unless known transection. |
| Nonunion / Hardware Failure | < 5% | Inadequate fixation, premature weight-bearing, severe comminution. | Revision ORIF with bone grafting if viable head; THA if associated with AVN or severe arthritis. |

Avascular necrosis remains the most dreaded complication. The risk increases significantly if the hip remains dislocated for more than 6 hours. Serial radiographs are required postoperatively to monitor for sclerosis, subchondral lucency (crescent sign), and eventual collapse of the femoral head. If symptomatic collapse occurs in an older patient, conversion to a total hip arthroplasty is the definitive salvage procedure. In younger patients, joint-preserving procedures such as core decompression or vascularized fibular grafting may be attempted prior to collapse, though results in the post-traumatic setting are less predictable than in idiopathic AVN.

Post Operative Rehabilitation Protocols
Postoperative rehabilitation must balance the need to protect the delicate articular fixation with the necessity of early mobilization to prevent stiffness and thromboembolic events.

Immediately postoperatively, the patient is placed on strict deep vein thrombosis (DVT) prophylaxis, utilizing low molecular weight heparin (LMWH) or direct oral anticoagulants (DOACs), barring any contraindications from concomitant visceral or intracranial trauma. Heterotopic ossification prophylaxis should be initiated within 24 hours of surgery, typically consisting of Indomethacin 75 mg sustained-release daily for 3 to 6 weeks, or a single fraction of 700 cGy localized radiation therapy to the hip.
Weight-bearing is strictly limited. Patients are typically restricted to toe-touch weight-bearing (TTWB) or flat-foot weight-bearing (to eliminate the gastrocnemius-soleus pump force across the hip joint) for a minimum of 6 to 8 weeks. Early passive and active-assisted range of motion is encouraged to nourish the articular cartilage and prevent capsular contracture. Flexion is generally limited to 90 degrees, and extreme internal or external rotation is avoided to protect the capsulotomy repair and the posterior soft tissues.
Progression to partial and then full weight-bearing is permitted only after radiographic evidence of fracture consolidation is observed, usually around the 8 to 12-week mark. Full return to heavy labor or high-impact sports may take 6 to 12 months and is contingent upon the absence of AVN or progressive arthritic changes.
Summary of Key Literature and Guidelines
The management of femoral head fractures has evolved significantly over the past few decades, heavily influenced by seminal anatomical and clinical studies.

The foundational work by Pipkin in 1957 established the classification system that remains universally utilized today. His correlation between the fracture location relative to the fovea capitis and the ultimate functional outcome set the stage for modern surgical indications. Epstein's subsequent large-scale reviews of posterior fracture-dislocations reinforced the critical nature of emergent reduction, demonstrating an exponential increase in avascular necrosis rates when reductions were delayed beyond 6 hours.

More recently, the anatomical studies by Gautier and Ganz detailing the precise extraosseous and intraosseous course of the medial femoral circumflex artery revolutionized the surgical approach to the hip. Their development of the surgical dislocation via a trochanteric flip osteotomy provided a safe, extensile method to address complex Pipkin fractures without compromising the residual vascularity. Current literature strongly supports the anterior Smith-Petersen approach for isolated, anteriorly displaced Pipkin I and II fractures, while the Ganz surgical dislocation is increasingly preferred for complex, comminuted, or posteriorly oriented fractures, offering superior visualization and lower rates of iatrogenic AVN compared to traditional posterior approaches.
Clinical & Radiographic Imaging