Hemiarthroplasty for Displaced Femoral Neck Fractures: An Intraoperative Masterclass

Key Takeaway
This masterclass provides a comprehensive, real-time guide to hemiarthroplasty for displaced femoral neck fractures. We delve into intricate surgical anatomy, meticulous preoperative planning, and granular intraoperative execution from the surgeon's perspective. Fellows will learn critical pearls, how to avoid pitfalls, and essential postoperative management strategies, ensuring a thorough understanding of this vital orthopaedic procedure.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and surgeons-in-training, to this definitive masterclass on the operative management of displaced femoral neck fractures. The geriatric hip fracture represents one of the most ubiquitous and consequential challenges encountered in modern orthopedic traumatology. As the global population ages, the incidence of these fragility fractures continues to rise exponentially, creating a "silver tsunami" that demands profound surgical expertise and optimized perioperative pathways. Our primary objective in performing a hemiarthroplasty is not merely the mechanical replacement of fractured bone, but the immediate restoration of patient mobility to mitigate the devastating systemic complications associated with prolonged recumbency.
The pathogenesis of femoral neck fractures in the elderly is inextricably linked to the deterioration of bone microarchitecture, predominantly driven by osteoporosis. A typical presentation involves a low-energy mechanism, such as a fall from standing height, where a direct impact on the greater trochanter transmits unyielding shear and compressive forces across the weakened cervical region of the proximal femur. In younger cohorts, these fractures are invariably the result of high-energy trauma—such as motor vehicle collisions or falls from significant heights—necessitating a completely different algorithmic approach focused on joint preservation rather than arthroplasty.
Understanding the profound epidemiological impact of this injury is paramount for any practicing orthopedic surgeon. The one-year mortality rate following a displaced femoral neck fracture in the geriatric population remains stubbornly high, historically cited between twenty and thirty percent, despite advancements in surgical technique and anesthetic care. This mortality is rarely a direct consequence of the fracture itself, but rather stems from the cascade of cardiopulmonary, thromboembolic, and infectious complications triggered by the injury and subsequent immobility. Therefore, hemiarthroplasty serves as a critical resuscitative procedure, designed to provide immediate, robust stability that permits full weight-bearing on post-operative day zero.
Mastering this procedure requires a synthesis of anatomical knowledge, biomechanical principles, and meticulous surgical execution. The transition from a competent surgeon to a master arthroplasty surgeon lies in the ability to anticipate intraoperative pitfalls, respect the delicate soft-tissue envelope, and flawlessly restore the patient's native hip biomechanics. Through this comprehensive text, we will dissect every phase of the hemiarthroplasty procedure, from nuanced preoperative templating to the final layered closure, equipping you with the requisite knowledge to execute this operation with unyielding precision and confidence.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional comprehension of proximal femoral anatomy is the absolute foundation of successful arthroplasty. The femoral neck acts as a dynamic structural strut, projecting superomedially and anteriorly from the femoral shaft to support the femoral head. In the average adult, the neck-shaft angle (angle of inclination) measures approximately 130 ± 7 degrees, while the native femoral anteversion averages between 10 and 15 degrees, though substantial ethnic and individual variations exist. The cross-sectional morphology of the femoral neck is not perfectly cylindrical but rather cam-shaped, featuring a shorter anteroposterior diameter compared to its mediolateral dimension, a critical detail when considering the trajectory of internal fixation or the geometry of a definitive neck osteotomy.


Crucial to the structural integrity of the proximal femur is the calcar femorale. This dense, vertically oriented condensation of cancellous bone originates superiorly near the greater trochanter and fuses with the posterior cortex of the femoral neck, projecting distally into the lesser trochanteric region. The calcar acts as the primary load-bearing conduit, transmitting compressive forces from the femoral head down into the medial femoral diaphysis. When performing a hemiarthroplasty, seating the collar of a prosthesis or ensuring appropriate cement mantle pressurization against the calcar is vital for preventing early subsidence and ensuring long-term axial stability of the construct.
The biomechanical symphony of the native hip joint relies heavily on the concepts of offset and leg length. Femoral offset is defined as the perpendicular distance from the center of rotation of the femoral head to the anatomical axis of the femoral shaft. Restoring this offset during hemiarthroplasty is non-negotiable; inadequate offset shortens the abductor lever arm, leading to a profound Trendelenburg gait, increased joint reactive forces, and debilitating postoperative limp. Conversely, excessive offset can lead to trochanteric bursitis and excessive tension on the soft tissues, potentially limiting range of motion and increasing wear on the native acetabular cartilage.
Vascular Anatomy and Osteonecrosis Pathophysiology
The vascular supply to the femoral head is a precarious network, rendering it highly susceptible to ischemic insult following a cervical fracture. The predominant arterial inflow is derived from the medial femoral circumflex artery (MFCA), specifically its lateral epiphyseal branch. The MFCA courses posteriorly around the base of the femoral neck, penetrating the joint capsule to give rise to ascending retinacular vessels that travel along the femoral neck to perfuse the head. This posterior and superior vascular dominance dictates that any significant displacement of a femoral neck fracture will inevitably shear or kink these vital conduits.
Secondary contributions to the femoral head's vascularity include the inferior metaphyseal artery, a branch of the lateral femoral circumflex artery, and the artery of the ligamentum teres, derived from the obturator artery. While the artery of the ligamentum teres is crucial during pediatric development, its contribution in the adult population is highly variable and often negligible, providing insufficient collateral circulation in the event of retinacular vessel disruption. Consequently, when a displaced intracapsular fracture occurs, the primary lifeblood of the femoral head is severed, precipitating the cascade toward avascular necrosis (AVN).
The incidence of AVN and subsequent nonunion in displaced femoral neck fractures managed with internal fixation in the elderly is unacceptably high, often exceeding thirty percent in historical cohorts. This high failure rate forms the primary biological rationale for abandoning joint-preserving operations in favor of arthroplasty for displaced fractures in the geriatric demographic. By excising the devascularized femoral head and replacing it with a prosthetic construct, the surgeon definitively eliminates the risks of nonunion and osteonecrosis, guaranteeing a stable, weight-bearing joint regardless of the compromised local vascularity.
Fracture Classification Frameworks
The Garden classification system remains the most universally utilized framework for categorizing femoral neck fractures, based primarily on the degree of displacement observed on the anteroposterior radiograph. Grade I represents an incomplete, valgus-impacted fracture; Grade II is a complete but nondisplaced fracture; Grade III denotes a completely fractured neck with partial displacement and varus malalignment; and Grade IV signifies complete displacement with no engagement of the primary fracture fragments. While academically detailed, for practical surgical decision-making, this system is frequently dichotomized into "nondisplaced" (Garden I and II) and "displaced" (Garden III and IV) categories.

Anatomical location also plays a critical role in classification and subsequent management. Subcapital fractures occur immediately distal to the articular cartilage of the femoral head, while transcervical fractures traverse the mid-portion of the femoral neck. Both are intracapsular and carry a high risk of vascular compromise. In contrast, basicervical fractures occur at the base of the neck, near the intertrochanteric line. These fractures are extracapsular, behave biomechanically more like intertrochanteric fractures, and are frequently amenable to robust internal fixation constructs, such as a dynamic hip screw or a cephalomedullary nail, rather than arthroplasty.
Understanding these classifications is not merely an academic exercise; it directly dictates the surgical algorithm. A Garden I or II fracture in an elderly patient is typically managed with percutaneous in situ pinning to prevent secondary displacement. However, the moment a fracture is deemed Garden III or IV in a patient with a physiologic age over 65 to 70 years, the treatment pendulum swings decisively towards hemiarthroplasty or total hip arthroplasty, prioritizing immediate stability over the precarious attempt at biological preservation.
Exhaustive Indications and Contraindications
The decision to proceed with a hemiarthroplasty is predicated on a meticulous evaluation of the patient's physiologic age, baseline functional demands, bone quality, and the specific morphological characteristics of the fracture. The quintessential indication for a hemiarthroplasty is a displaced, intracapsular femoral neck fracture (Garden III or IV) in an elderly, low-demand ambulator. In this specific cohort, the primary goal is rapid mobilization to prevent the cascade of immobility-related complications. Hemiarthroplasty provides immediate structural stability, allowing for full, unrestricted weight-bearing immediately post-operation, a feat rarely achievable or reliable with internal fixation in osteoporotic bone.
Beyond the standard geriatric trauma presentation, hemiarthroplasty is heavily indicated in patients with profoundly compromised bone stock. Individuals exhibiting a Dorr Type C proximal femur—characterized by a wide, "stovepipe" medullary canal and paper-thin cortices—are exceptionally poor candidates for internal fixation due to the exorbitant risk of hardware cut-out and catastrophic failure. Similarly, patients presenting with pathologic fractures secondary to metastatic disease, or those with severe neurological comorbidities such as Parkinson's disease or dense hemiplegia, require the predictable, robust stability that only an arthroplasty construct can provide, minimizing the risk of postoperative dislocation or construct failure.
Conversely, absolute and relative contraindications must be rigorously respected to prevent catastrophic postoperative failures. The most critical contraindication to a hemiarthroplasty is preexisting symptomatic acetabular disease, such as advanced osteoarthritis or inflammatory arthropathy. Placing a hard metallic prosthetic head against a compromised, eburnated acetabulum will inevitably lead to rapid, agonizing cartilage wear, groin pain, and the need for early, complex revision to a total hip arthroplasty. Furthermore, young physiologic age is a strong relative contraindication; in patients under 60 years old, every heroic effort should be made to achieve an anatomical reduction and stable internal fixation to preserve the native joint and avoid the long-term complications of arthroplasty.
| Parameter | Indications for Hemiarthroplasty | Contraindications for Hemiarthroplasty |
|---|---|---|
| Patient Age / Demand | Physiologic age > 70 years, low functional demand, household ambulator. | Physiologic age < 60 years, high functional demand, active lifestyle. |
| Fracture Pattern | Displaced intracapsular (Garden III/IV), inadequate closed reduction. | Nondisplaced (Garden I/II), basicervical, or intertrochanteric fractures. |
| Bone Quality | Severe osteoporosis (Dorr Type C), pathologic lesions, renal osteodystrophy. | Excellent bone stock amenable to rigid screw fixation. |
| Joint Status | Pristine native acetabular cartilage, no prior hip pain. | Preexisting acetabular osteoarthritis, rheumatoid arthritis, inflammatory arthropathy. |
| Systemic Factors | Neuromuscular disorders (Parkinson's), limited life expectancy. | Active systemic sepsis, localized active joint infection. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a hemiarthroplasty is largely determined before the scalpel ever touches the skin. Meticulous preoperative planning begins with a comprehensive clinical assessment. The classic presentation of a shortened, externally rotated limb is pathognomonic for a displaced proximal femur fracture. However, the surgeon must maintain a high index of suspicion for occult fractures, where the limb may appear normally aligned. The logroll test—gently rolling the limb internally and externally—is the most sensitive clinical maneuver; excruciating groin pain during this test strongly suggests a femoral neck fracture, even in the absence of gross radiographic displacement.
Radiographic evaluation must be exhaustive. A standard anteroposterior (AP) view of the pelvis and a cross-table lateral view of the affected hip are mandatory. The AP pelvis allows for comparison with the contralateral, uninjured hip, which is vital for assessing native offset and leg length. The cross-table lateral is indispensable for quantifying the degree of posterior comminution and true anteroposterior displacement. In cases of high-energy trauma or suspected occult fractures, advanced imaging modalities such as Magnetic Resonance Imaging (MRI) or thin-slice Computed Tomography (CT) become invaluable, with MRI being the gold standard for detecting radiographically silent trabecular microfractures.


Digital Templating and Component Selection
Digital templating is a non-negotiable phase of the preoperative workflow, transforming a generic procedure into a patient-specific reconstruction. Utilizing calibrated digital radiographs, the surgeon must first determine the center of rotation of the native, uninjured hip. By overlaying prosthetic templates on the contralateral normal femur, the surgeon can accurately predict the required stem size, the optimal level of the femoral neck osteotomy, and the specific head-neck offset required to restore native abductor tension. Failure to template frequently results in leg length discrepancies, instability, or the selection of an inappropriately sized implant that risks intraoperative periprosthetic fracture.
The choice of implant fixation—cemented versus cementless—is a critical decision made during the templating phase. Cemented stems are the gold standard for elderly patients with osteoporotic, Dorr Type B or C bone, providing immediate, uniform stress transfer and a significantly lower risk of intraoperative fracture. However, the use of bone cement carries the risk of Bone Cement Implantation Syndrome (BCIS), necessitating meticulous canal preparation and communication with anesthesia. Cementless, press-fit stems are reserved for younger patients or those with robust, Dorr Type A bone, relying on diaphyseal or metaphyseal engagement for initial stability and subsequent osteointegration.
Sizing the prosthetic femoral head is equally critical. The extracted native head will be measured intraoperatively using a specialized caliper, but preoperative estimation is helpful. The goal is to select a unipolar or bipolar head that perfectly matches the native acetabular diameter. An oversized head will cause equatorial binding, leading to restricted range of motion, severe groin pain, and rapid destruction of the acetabular rim. Conversely, an undersized head will result in polar point-loading, accelerating superior dome wear, increasing contact stresses, and precipitating early central migration of the prosthesis.
Anesthesia, Positioning, and Theater Setup
The choice of anesthesia—neuraxial (spinal) versus general—is tailored to the patient's cardiopulmonary status in consultation with the anesthesia team. Spinal anesthesia is frequently preferred as it may reduce intraoperative blood loss, lower the risk of deep vein thrombosis, and minimize the pulmonary complications associated with intubation in frail, elderly patients. Regardless of the anesthetic modality, the administration of prophylactic intravenous antibiotics (typically a first-generation cephalosporin) within one hour prior to incision is an absolute, non-negotiable standard of care to prevent periprosthetic joint infection.


Patient positioning is paramount for achieving optimal surgical exposure and ensuring accurate intraoperative assessment of leg length and component version. For the standard posterolateral approach, the patient is placed in the true lateral decubitus position. The operating table must be perfectly parallel to the floor. Rigid pelvic fixation is achieved using a pegboard system, a vacuum beanbag, or padded lateral positioners applied to the anterior superior iliac spine (ASIS) and the sacrum. The sacral pad must be positioned carefully to avoid obstructing the posterior surgical trajectory.
An axillary roll is placed beneath the dependent thorax to protect the brachial plexus, and all bony prominences, particularly the common peroneal nerve at the fibular head of the down leg, are meticulously padded. The operative leg is draped free to allow for full, unrestricted manipulation during the procedure. The surgeon must verify that the pelvis is not tilted or rotated, as any malpositioning will severely distort the surgeon's perception of acetabular version and femoral anteversion, inevitably leading to prosthetic malposition and a high risk of postoperative dislocation.
Step-by-Step Surgical Approach and Fixation Technique
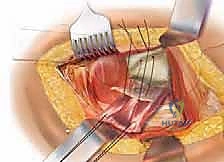
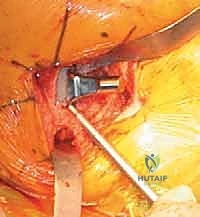
The posterolateral approach (frequently referred to as the Moore or Southern approach) remains the workhorse exposure for hemiarthroplasty due to its extensile nature, excellent visualization of the proximal femur, and relative ease of execution. The incision is centered over the posterior third of the greater trochanter, extending proximally towards the posterior superior iliac spine and distally along the axis of the femoral shaft. Following meticulous hemostasis of the subcutaneous tissues, the fascia lata is sharply incised in line with the skin incision, and the gluteus maximus fibers are bluntly split in line with their orientation, taking care to coagulate any traversing branches of the inferior gluteal artery.




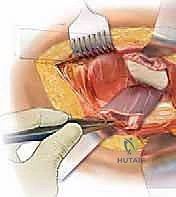
Deep retraction reveals the short external rotators (SERs) and the piriformis tendon. The sciatic nerve, located posteriorly, is identified but not routinely dissected unless its course is aberrant; it is protected throughout the case by gentle, broad retraction of the posterior soft tissues. The piriformis, superior gemellus, obturator internus, and inferior gemellus are tagged with heavy non-absorbable sutures and sharply detached from their insertion at the trochanteric fossa. This conjoined tendon flap is reflected posteriorly, serving as a protective soft-tissue buffer over the sciatic nerve.
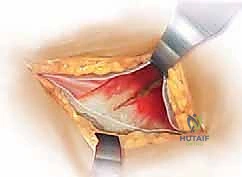
A robust, full-thickness capsulotomy is then performed. A T-shaped or H-shaped incision is made in the posterior capsule, and the capsular flaps are tagged for later robust repair. Upon entering the joint, a copious fracture hematoma is typically encountered and evacuated. The fractured femoral neck is visualized, and the femoral head is extracted using a heavy corkscrew device. Extraction can be challenging if a vacuum seal exists within the acetabulum; passing a curved elevator behind the head to break the suction seal is often necessary. Once retrieved, the native head is meticulously measured with calipers to dictate the definitive prosthetic head size.



Proximal Femoral Preparation and Osteotomy
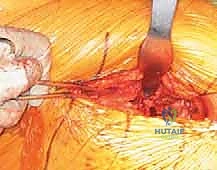
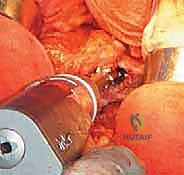
With the head removed, the limb is internally rotated, flexed, and adducted to deliver the proximal femur out of the wound. The definitive neck osteotomy is performed using an oscillating saw. The level and angle of this cut are dictated by the preoperative template, typically referencing a specific distance (often one fingerbreadth or approximately 1.5 cm) proximal to the lesser trochanter. The cut must be smooth and precise to provide a stable platform for the prosthetic collar, if a collared stem is utilized. A box osteotome is then used to open the femoral canal laterally, ensuring the trajectory is aligned with the anatomical axis of the diaphysis to prevent varus malpositioning.




Sequential broaching of the femoral canal is performed with escalating sizes. The surgeon must pay absolute attention to the version of the broach, aiming to reproduce the patient's native anteversion, typically between 10 and 15 degrees relative to the posterior condylar axis of the knee. Excessive retroversion will lead to posterior instability, while excessive anteversion risks anterior dislocation. Broaching continues until axial and rotational stability is achieved within the metaphyseal bone. If a cemented stem is planned, the canal is broached to a size larger than the chosen implant to allow for an adequate, uniform 2mm cement mantle.
For cemented fixation, meticulous canal preparation is paramount. The canal is aggressively brushed and irrigated with pulsatile lavage to remove all fat, marrow, and debris, minimizing the embolic load and ensuring interdigitation of the cement into the cancellous trabeculae. A distal cement restrictor is placed to allow for adequate pressurization. Third-generation cementing techniques are employed: the bone cement is vacuum-mixed to reduce porosity, injected retrogradely using a cement gun, and proximally pressurized. The definitive stem is then inserted in the correct version and held rigidly until complete polymerization occurs.



Trialing, Implantation, and Meticulous Closure
Prior to definitive implantation, a rigorous trialing phase is mandatory. The trial stem and head are inserted, and the hip is reduced. The surgeon assesses soft tissue tension, leg length equality (by palpating the relationship of the medial malleoli or comparing knee heights), and dynamic stability. The "shuck test" is performed: applying longitudinal traction to the femur to ensure no more than 2-3 millimeters of distraction occurs, indicating appropriate myofascial tension. The hip is then taken through a full, extreme range of motion—particularly flexion, adduction, and internal rotation—to ensure there is no bony or hardware impingement that could lever the head out of the acetabulum.



Once the optimal parameters are confirmed, the trial components are removed. If a bipolar head is selected, it is assembled onto the definitive stem on the back table. The final components are implanted, and the hip is gently reduced. A final check of stability and range of motion is conducted. At this juncture, meticulous irrigation of the joint space is performed to remove any residual bone debris or cement particles, which act as potent third-body wear generators if left behind.



The closure is arguably as critical as the bony reconstruction, particularly when utilizing a posterolateral approach, to mitigate the risk of postoperative dislocation. A robust, transosseous repair of the posterior capsule and the short external rotators is mandatory. Heavy non-absorbable sutures are passed through drill holes in the greater trochanter and tied securely, re-establishing the posterior soft-tissue tension band. The fascia lata is closed tightly, followed by a layered closure of the subcutaneous tissues and skin.




Complications, Incidence Rates
Clinical & Radiographic Imaging Archive