Mastering Outcomes and Complications in Femoral Neck Fracture Fixation
Key Takeaway
Internal fixation of femoral neck fractures is fraught with potential complications, including fixation failure, nonunion, osteonecrosis, and infection. Successful management requires a deep understanding of hip biomechanics, precise implant selection, and meticulous surgical technique. This guide details the pathophysiology, prevention, and salvage strategies for these complex scenarios, ranging from valgus-producing osteotomies in young adults to arthroplasty in the geriatric population.
Comprehensive Introduction and Patho-Epidemiology
Femoral neck fractures remain one of the most intellectually and technically demanding injuries in orthopedic traumatology, historically and accurately dubbed the "unsolved fracture." Despite decades of iterative advancements in implant metallurgy, intraoperative fluoroscopic imaging, and a deeper understanding of fracture biology, internal fixation of the femoral neck continues to be associated with a uniquely high and frustrating complication profile. The precarious retrograde blood supply to the femoral head, combined with the immense, multidirectional shear forces acting across the fracture site, creates an inherently hostile biomechanical and biological environment for osteogenesis. As the global population ages, the burden of these fractures is increasing exponentially, demanding that orthopedic surgeons master both the index fixation techniques and the complex salvage pathways required when initial interventions fail.
The epidemiology of femoral neck fractures classically follows a bimodal distribution, reflecting two distinct pathophysiological mechanisms. In the younger demographic, typically defined as patients under the age of 60, these injuries are the result of high-energy trauma, such as motor vehicle collisions or falls from significant heights. These high-energy mechanisms impart massive kinetic energy to the proximal femur, resulting in vertically oriented, highly unstable fracture patterns with significant comminution and profound disruption of the delicate retinacular blood supply. Conversely, in the geriatric population, femoral neck fractures are predominantly low-energy fragility fractures. These occur secondary to age-related deterioration of trabecular architecture, cortical thinning, and diminished bone mineral density (osteoporosis), often precipitated by a simple fall from a standing height.
Understanding the patho-epidemiology extends beyond the mere mechanism of injury; it encompasses the systemic physiological status of the patient. In the elderly, a femoral neck fracture is rarely an isolated orthopedic event; it is frequently a sentinel event signaling a broader systemic decline. The one-year mortality rate following a hip fracture in the geriatric population remains staggeringly high, ranging from 20% to 30%, driven by cardiopulmonary complications, thromboembolic events, and the physiological stress of prolonged immobility. Therefore, the overarching goal of intervention in this demographic is not merely fracture union, but the rapid restoration of mobility and the minimization of perioperative morbidity.
For the consultant orthopedic surgeon, anticipating, recognizing, and managing the myriad complications associated with femoral neck fracture fixation is paramount. The primary adverse outcomes following internal fixation include catastrophic failure of fixation, clinically significant femoral neck shortening, nonunion, osteonecrosis (avascular necrosis), and deep postoperative infection. Determining the exact etiology of a complication—whether it stems from a biological failure, a biomechanical failure, or a combination of both—is the critical first step in formulating a successful, definitive revision strategy. Mastery of this domain requires an exhaustive understanding of surgical anatomy, meticulous preoperative planning, and flawless execution of osteosynthesis principles.
Detailed Surgical Anatomy and Biomechanics
A profound comprehension of the vascular anatomy of the proximal femur is the bedrock upon which successful femoral neck fracture management is built. The femoral head receives its blood supply from three primary sources: the extracapsular arterial ring, the ascending cervical branches (retinacular vessels), and the artery of the ligamentum teres. The extracapsular ring is formed by the anastamosis of the medial circumflex femoral artery (MCFA) posteriorly and the lateral circumflex femoral artery (LCFA) anteriorly. The most critical of these is the MCFA, which gives rise to the lateral epiphyseal artery system. These terminal vessels penetrate the joint capsule distally and course proximally along the posterosuperior aspect of the femoral neck within the retinacular folds to perfuse the majority of the femoral head.
The intracapsular nature of the femoral neck fracture poses a unique biological challenge. Unlike the diaphysis of long bones, the femoral neck is devoid of a cambium layer within its periosteum. Consequently, fracture healing in this region relies almost entirely on endosteal callus formation and primary cortical remodeling, rather than robust periosteal callus generation. Furthermore, the synovial fluid within the hip capsule contains fibrinolysins that actively inhibit the formation of a stable initial fracture hematoma, further retarding the early stages of the biological healing cascade. Any disruption of the retinacular vessels, whether from the initial traumatic displacement or iatrogenic injury during surgical exposure and reduction, dramatically increases the risk of osteonecrosis.
Biomechanically, the proximal femur is a complex structure engineered to withstand massive physiological loads. During normal ambulation, the joint reaction forces across the hip can exceed three to five times the patient's total body weight. These forces are transmitted through the trabecular systems of the proximal femur, primarily the principal compressive trabeculae (medial) and the principal tensile trabeculae (lateral). The area of relative trabecular sparsity between these systems, known as Ward's triangle, is highly susceptible to osteoporotic structural failure. When a fracture occurs, the orientation of the fracture line relative to the horizontal axis—classically described by the Pauwels classification—dictates the biomechanical environment.
Pauwels Type I fractures (less than 30 degrees) experience primarily compressive forces, which are conducive to primary bone healing. However, Pauwels Type III fractures (greater than 50 degrees) are subjected to massive, deleterious shear forces. These shear forces promote fracture displacement, varus collapse, and hardware failure if not adequately neutralized by the chosen fixation construct. The surgeon must recognize that the mechanical axis of the lower extremity and the offset of the femoral neck create a lever arm that continuously attempts to drive the femoral head into varus and retroversion. Successful fixation demands an anatomical reduction that restores the native cortical buttress, particularly at the calcar femorale, to convert these destructive shear forces into therapeutic compressive forces.
Exhaustive Indications and Contraindications
The decision-making matrix for treating femoral neck fractures is complex, requiring the surgeon to synthesize the patient's physiological age, baseline functional status, bone quality, fracture morphology, and the presence of preexisting hip pathology. The fundamental dichotomy in treatment lies between joint-preserving internal fixation (osteosynthesis) and joint-replacing arthroplasty. Internal fixation is unequivocally the treatment of choice for all physiologically young and active patients, regardless of fracture displacement, as the preservation of the native femoral head is paramount for long-term functional survival. In this cohort, every surgical effort must be expended to achieve an anatomical reduction and rigid, length-stable fixation.
In the geriatric population, the indications for internal fixation are more narrowly defined. Nondisplaced or valgus-impacted fractures (Garden I and II) in the elderly are generally well-served by in situ internal fixation, typically utilizing multiple cannulated screws or a fixed-angle device. The biological envelope is minimally disrupted, and the inherent stability of the impacted fracture pattern yields high union rates with low surgical morbidity. However, for displaced femoral neck fractures (Garden III and IV) in patients over the age of 65, the literature overwhelmingly supports primary arthroplasty (total hip arthroplasty or hemiarthroplasty). Internal fixation in this specific demographic carries an unacceptably high reoperation rate (often exceeding 30-40%) due to fixation failure, nonunion, and osteonecrosis.
Contraindications to internal fixation must be rigorously respected to avoid predictable, catastrophic failures. Absolute contraindications include established, severe osteoarthritis or inflammatory arthropathy of the ipsilateral hip joint, as preserving a painful, degenerative joint offers no functional benefit to the patient. Additionally, pathological fractures secondary to metastatic disease or severe metabolic bone disease with inadequate bone stock for screw purchase are absolute contraindications for osteosynthesis; these scenarios mandate endoprosthetic reconstruction to provide immediate, durable stability.
Relative contraindications revolve around patient-specific factors that compromise the likelihood of successful biological healing or mechanical stability. Patients with severe, uncorrectable coagulopathies, active systemic infections, or those who are non-ambulatory at baseline (bedbound) may be better served by non-operative management or palliative arthroplasty depending on their overall prognosis. Furthermore, a delayed presentation of a displaced fracture in a young patient (greater than 2-3 weeks) represents a relative contraindication to standard in situ fixation, often necessitating a more complex reconstructive approach, such as a primary valgus intertrochanteric osteotomy, to address the highly probable nonunion.
Indications and Contraindications Matrix
| Parameter | Indications for Internal Fixation | Contraindications for Internal Fixation |
|---|---|---|
| Patient Age / Demand | Physiologically young, high-demand patients (Absolute indication). | Low-demand, geriatric patients with displaced fractures (Relative to Arthroplasty). |
| Fracture Pattern | Nondisplaced or valgus-impacted fractures (Garden I/II) in all age groups. | Highly comminuted, osteoporotic fractures lacking medial calcar support. |
| Joint Status | Healthy, native articular cartilage with no preexisting symptomatic pathology. | Preexisting severe osteoarthritis, rheumatoid arthritis, or established AVN. |
| Bone Quality | Normal bone density capable of providing excellent hardware purchase. | Severe osteoporosis or pathological fractures (e.g., metastatic lesions). |
| Timing of Surgery | Acute presentation (ideally < 24-48 hours from injury). | Late presentation (> 3 weeks) with established nonunion/resorption. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the invisible foundation upon which surgical success is built. The evaluation begins with high-quality, orthogonally oriented radiographs, specifically an anteroposterior (AP) view of the pelvis and a cross-table lateral view of the affected hip. The AP pelvis allows for the assessment of the contralateral, uninjured proximal femur, providing a template for native neck-shaft angle, femoral offset, and leg length. Traction-internal rotation views are often invaluable; by temporarily neutralizing the deforming forces of the iliopsoas and short external rotators, these views unmask the true fracture morphology, the degree of comminution, and the feasibility of achieving a closed anatomical reduction.
In the modern era, advanced imaging is increasingly utilized. A preoperative computed tomography (CT) scan with 3D reconstructions is highly recommended for all young patients with high-energy fractures. CT imaging delineates occult comminution, defines the exact spatial orientation of the fracture plane (true Pauwels angle), and identifies basicervical extensions or associated femoral head fractures that would fundamentally alter the implant selection and surgical approach. Digital templating software must be employed to calculate the anticipated length of the lag screws, the appropriate angle of a sliding hip screw (typically 130 to 145 degrees), and the optimal entry point on the lateral cortex to ensure central placement within the femoral head.
Patient positioning is a critical decision that dictates the flow of the entire operation. The surgeon must choose between a specialized orthopedic fracture table and a standard radiolucent flat table. The fracture table allows for sustained, controlled skeletal traction and facilitates unimpeded fluoroscopic access for AP and lateral imaging. It is particularly advantageous for closed reduction and percutaneous fixation techniques. The affected limb is placed in a traction boot, and the reduction is achieved through longitudinal traction, slight abduction, and internal rotation to correct the typical external rotation deformity.
Conversely, positioning the patient supine on a flat radiolucent table is mandatory if an open reduction via an anterior (Smith-Petersen) or anterolateral (Watson-Jones) approach is anticipated. The flat table allows for dynamic manipulation of the limb during the procedure, which is essential for mobilizing the fracture fragments and achieving a direct, visually confirmed anatomical reduction. A bump is placed under the ipsilateral hemipelvis to elevate the hip, and the limb is draped free to allow for full range of motion. Regardless of the table chosen, the C-arm fluoroscopy unit must be positioned and tested prior to sterile draping to ensure that perfect, unobstructed AP and true lateral images of the femoral neck and head can be obtained seamlessly throughout the case.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution begins with the reduction of the fracture. A non-anatomical reduction, particularly one leaving the fracture in varus or retroversion, is the single greatest predictor of early fixation failure. Accept nothing less than an anatomical or slightly valgus reduction. If a closed reduction (e.g., the Leadbetter maneuver) fails to achieve perfect cortical alignment, the surgeon must immediately transition to an open reduction. An anterior Smith-Petersen approach is preferred for open reduction as it provides direct access to the intracapsular fracture hematoma, allows for a thorough capsulotomy, and facilitates direct manipulation of the proximal fragment without violating the precarious posterior retinacular blood supply.
Once anatomical reduction is achieved and provisionally held with smooth Kirschner wires, implant selection dictates the fixation sequence. For stable, purely transcervical fractures, multiple cannulated cancellous screws (typically 6.5mm or 7.0mm) placed in an inverted triangle configuration provide excellent torsional stability. The inferior screw must rest directly on the dense bone of the calcar femorale to resist varus bending moments. The posterior and anterior screws are placed superiorly, hugging the respective cortices. All screws must terminate in the dense subchondral bone of the femoral head, optimizing the tip-apex distance (TAD) to prevent hardware cutout.
For vertically oriented, highly unstable fracture patterns (Pauwels Type III) or basicervical variants, multiple parallel screws are biomechanically insufficient to resist the massive shear forces. In these scenarios, a fixed-angle construct, such as a Sliding Hip Screw (SHS) or a Femoral Neck System (FNS), is mandatory. The SHS provides a robust lateral cortical buttress and allows for controlled, dynamic compression along the axis of the femoral neck.

Figure 55-16A: Preoperative radiograph at the time of injury demonstrating a displaced femoral neck fracture with significant biomechanical instability.

Figure 55-16B: Postoperative anteroposterior radiograph after operative reduction and fixation utilizing a fixed-angle sliding hip screw construct to provide controlled collapse while resisting excessive varus deformity.

Figure 55-16C: Postoperative lateral radiograph confirming central placement of the lag screw within the femoral head, optimizing the tip-apex distance (TAD).
When utilizing an SHS for a femoral neck fracture, a supplementary derotation screw is critical. The reaming process for the large lag screw imparts significant torsional torque, which can inadvertently spin the femoral head and destroy the reduction. A fully threaded positioning screw is placed superior and anterior to the planned lag screw trajectory prior to reaming. Once the lag screw is deployed and the side plate is secured to the femoral shaft, the traction is released, and the fracture is allowed to compress dynamically. Meticulous attention to the TAD, aiming for a combined AP and lateral distance of less than 25mm, is the most critical intraoperative metric to prevent subsequent mechanical failure.
Complications, Incidence Rates, and Salvage Management
Despite flawless surgical technique, the complication profile for femoral neck fracture fixation remains formidable. Internal fixation may fail due to a confluence of mechanical and biological factors. The most common culprits include inadequate anatomical reduction, poor implant selection, suboptimal implant positioning, unrecognized nonunion, osteonecrosis, and occult infection. Failure typically manifests as varus collapse, retroversion of the femoral head, or hardware cutout. The femoral neck is subjected to massive compressive and shear forces during physiological loading. If a fracture is left in varus or retroversion during the index procedure, the resultant joint reaction forces will drive the hardware through the cancellous bone of the femoral head, leading to catastrophic cutout.
Historically, the paradigm for treating femoral neck fractures involved using partially threaded cannulated screws to allow for dynamic compression across the fracture site. While compression promotes primary bone healing, excessive sliding leads to significant femoral neck shortening. Significant shortening alters the biomechanics of the hip joint by decreasing femoral offset. This reduces the lever arm of the hip abductors (gluteus medius and minimus), resulting in profound abductor weakness, a persistent Trendelenburg gait, increased energy expenditure, and diminished patient-reported outcome measures (PROMs).
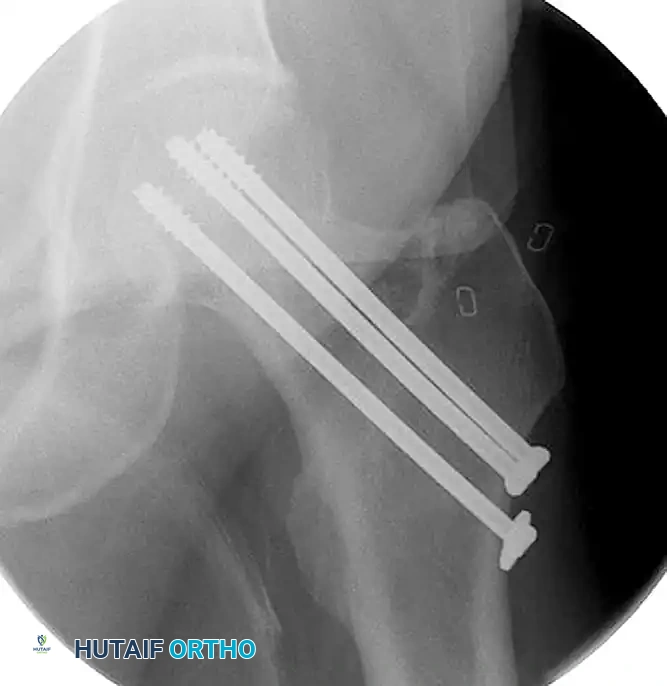
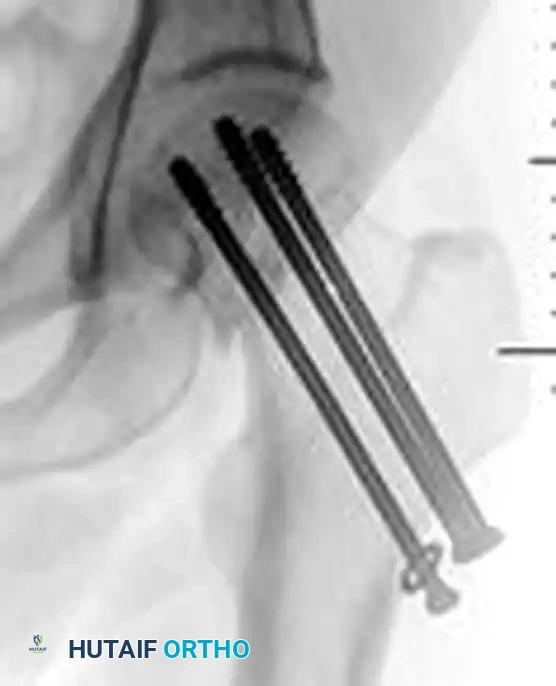
Figure 55-15A: Intraoperative fluoroscopic anteroposterior view demonstrating the initial fixation of a minimally displaced femoral neck fracture utilizing three partially threaded cannulated screws.
Figure 55-15B: Postoperative anteroposterior radiograph revealing significant femoral neck shortening. The dynamic compression allowed by the partially threaded screws has resulted in a loss of femoral offset and abductor lever arm.
Nonunion of the femoral neck occurs in up to 15-30% of displaced fractures treated with internal fixation. It is defined as a lack of radiographic progression of healing at 6 months post-injury, accompanied by persistent groin or thigh pain. In young, active patients with a viable femoral head, a valgus intertrochanteric osteotomy is the procedure of choice for nonunion. By resecting a laterally based wedge of bone from the intertrochanteric region, the femoral neck is placed into valgus. This converts the deleterious shear forces (Pauwels III) at the nonunion site into favorable compressive forces (Pauwels I), stimulating osteogenesis.
Osteonecrosis (AVN) is a devastating complication resulting from the disruption of the delicate blood supply to the femoral head. While initial trauma tears retinacular vessels, secondary ischemia can occur due to an intracapsular hematoma. The hip capsule is a robust, unyielding structure. Bleeding from the fracture site accumulates within the joint, exponentially raising intracapsular pressure. If this pressure exceeds the capillary perfusion pressure, a tamponade effect occurs. Decompression via capsulotomy is highly recommended in young patients to mitigate this risk. Deep infection following fixation is catastrophic, characterized by biofilm formation on avascular bone and metallic implants. Acute infections with stable hardware require aggressive débridement and hardware retention until union, whereas chronic infections demand complete hardware removal, resection of necrotic bone, and staged arthroplasty.
Complications and Salvage Strategies
| Complication | Estimated Incidence | Primary Etiology | Definitive Salvage Strategy |
|---|---|---|---|
| Fixation Failure (Cutout) | 5% - 15% | Malreduction (varus/retroversion), high TAD, poor bone quality. | Young: Revision ORIF or Valgus Osteotomy. Elderly: Conversion to THA/Hemi. |
| Femoral Neck Shortening | 25% - 60% | Uncontrolled dynamic compression, highly comminuted fractures. | Conservative (shoe lift, PT). Severe: Trochanteric advancement or THA. |
| Nonunion | 10% - 30% | Inadequate stability, shear forces (Pauwels III), biological failure. | Young: Valgus Intertrochanteric Osteotomy. Elderly: Conversion to THA. |
| Osteonecrosis (AVN) | 10% - 30% | Disruption of MCFA retinacular vessels, intracapsular tamponade. | Pre-collapse: Core decompression/osteotomy. Post-collapse: Total Hip Arthroplasty. |
| Deep Surgical Infection | 1% - 5% | Bacterial seeding, hematoma, prolonged surgical time, poor host biology. | Acute: I&D, retain hardware. Chronic: Hardware removal, resection arthroplasty, staged THA. |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of femoral neck fracture fixation relies as heavily on strict adherence to postoperative rehabilitation protocols as it does on intraoperative biomechanical execution. Rehabilitation must be carefully phased to balance the mechanical limitations of the fixation construct with the physiological necessity of early mobilization. The immediate postoperative phase (Days 0-14) is focused on medical optimization, pain control, and the prevention of catastrophic systemic complications. Chemical thromboembolic prophylaxis (e.g., Low Molecular Weight Heparin or Direct Oral Anticoagulants) combined with mechanical prophylaxis is mandatory for a minimum of 28 to 35 days postoperatively, as pelvic and hip trauma carries a profound risk for deep vein thrombosis (DVT) and pulmonary embolism (PE).
Weight-bearing status is the most critical variable in the rehabilitation protocol and must be individualized based on patient age, fracture pattern, and the rigidity of the chosen fixation. For young patients treated with multiple cannulated screws or an SHS for a displaced or vertically oriented fracture, weight-bearing is typically restricted to toe-touch weight-bearing (TTWB) or partial weight-bearing (PWB, roughly 20-30 lbs) for 6 to 8 weeks. This restriction is vital to prevent early varus collapse and catastrophic hardware cutout before early endosteal callus can form. Conversely, in elderly patients where internal fixation was chosen (typically for nondisplaced fractures), immediate weight-bearing as tolerated (WBAT) is often permitted. The risk of mechanical failure in the elderly is superseded by the life-threatening risks of prolonged recumbency, including atelectasis, pneumonia, and decubitus ulcers.
The intermediate rehabilitation phase (Weeks 6-12) marks the transition to active functional recovery. Radiographic surveillance is paramount during this period. Serial radiographs (AP and cross-table lateral) should be obtained at 2 weeks, 6 weeks, 3 months, 6 months, and 1 year. The surgeon must meticulously evaluate for signs of varus subsidence, screw back-out, loss of joint space, or subchondral sclerosis indicative of impending osteonecrosis. Once early radiographic union is confirmed—typically around the 6-to-8-week mark—patients are progressively advanced to full weight-bearing. Physical therapy intensifies, shifting focus from simple range of motion to aggressive strengthening of the hip abductor complex (gluteus medius and minimus) to counteract the biomechanical disadvantage caused by any minor femoral neck shortening.
The final phase of rehabilitation (Months 3-12) is dedicated to restoring pre-injury functional baseline and monitoring for late-onset complications. Patients are encouraged to resume low-impact cardiovascular activities and proprioceptive training. The surgeon must remain vigilant for the insidious onset of groin pain during this phase, which is often the earliest clinical harbinger of late nonunion or the collapse phase of osteonecrosis. Early detection of these clinical and radiographic signs allows for timely, joint-preserving interventions before catastrophic structural failure necessitates complex arthroplasty reconstruction.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management of femoral neck fractures is heavily guided by high-level, multicenter randomized controlled trials that have fundamentally shaped orthopedic trauma protocols. Among the most influential is the FAITH trial (Fixation using Alternative Implants for the Treatment of Hip fractures). This landmark international study compared the outcomes of sliding hip screws versus multiple cancellous screws in the treatment of femoral neck fractures. The FAITH trial demonstrated that while both constructs yielded similar overall rates of reoperation, the sliding hip screw provided a distinct biomechanical advantage in basicervical and vertically oriented fracture patterns, significantly reducing the risk of avascular necrosis and nonunion in these specific, highly unstable morphologies.
Equally critical to the understanding of geriatric hip fracture management is the HEALTH trial (Hip fracture Evaluation with Alternatives of Total Hip arthroplasty versus Hemiarthroplasty). While focused on arthroplasty, its findings heavily influence the indications for internal fixation. The HEALTH trial established that for displaced femoral neck fractures in the elderly, arthroplasty provides superior functional outcomes and lower reoperation rates compared to internal fixation. Furthermore, it delineated that total hip arthroplasty offers a modest functional advantage over hemiarthroplasty in highly active, independent older adults, thereby narrowing the indications for osteosynthesis in the geriatric population strictly to nondisplaced or valgus-impacted fracture patterns.
Clinical guidelines promulgated by major orthopedic societies, including the American Academy of Orthopaedic Surgeons (AAOS) and the Orthopaedic Trauma Association (OTA), emphasize the critical importance of surgical timing. Current evidence-based guidelines strongly recommend that surgical intervention for femoral neck fractures—whether fixation or arthroplasty—be performed within 24 to 48 hours of hospital admission. Delays beyond this window are unequivocally associated with exponential increases in 30-day mortality, major medical complications (delirium, pneumonia, thromboembolism), and prolonged hospital lengths of stay. In young patients, treating a displaced femoral neck fracture as a true physiological emergency, with intervention ideally occurring within 12 to 24 hours, is advocated to decompress the intracapsular hematoma and maximize the potential for femoral head survival.
The synthesis of this landmark literature dictates a highly algorithmic approach to femoral neck fractures. The surgeon must abandon dogmatic adherence to a single technique and instead apply a nuanced, evidence-based strategy. This requires the integration of patient-specific physiological parameters, advanced biomechanical principles, and an exhaustive understanding of the complication profile. Only through this rigorous, academically grounded approach can the orthopedic surgeon hope to master the outcomes and effectively manage the inevitable complications of the "unsolved fracture."
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).
