Open Reduction and Internal Fixation of Femoral Neck Fractures: A Master Surgical Guide

Key Takeaway
Open reduction and internal fixation (ORIF) of femoral neck fractures is indicated when closed reduction fails or in young patients requiring anatomic restoration. Utilizing a modified Smith-Petersen approach allows direct visualization of the fracture. Fixation constructs, including cannulated screws, compression hip screws, or proximal femoral locking plates, are selected based on fracture geometry and comminution. Achieving anatomic reduction and length-stable fixation is paramount to minimizing complications such as osteonecrosis and nonunion.
Comprehensive Introduction and Patho-Epidemiology
The management of displaced intracapsular femoral neck fractures, particularly in the young, physiologically active patient, remains one of the most formidable and unforgiving challenges in the realm of orthopedic trauma. Unlike intertrochanteric fractures, which occur in highly vascularized extracapsular cancellous bone with a robust healing envelope, femoral neck fractures occur within the synovial fluid-filled joint capsule and jeopardize the tenuous retrograde blood supply to the femoral head. This anatomical reality creates a uniquely hostile environment for fracture healing, predisposing the patient to catastrophic complications such as osteonecrosis (avascular necrosis, AVN) and nonunion. The bimodal epidemiological distribution of these injuries dictates two entirely distinct treatment paradigms. In the elderly, low-demand population, these fractures typically result from low-energy ground-level falls through osteoporotic bone, and the gold standard of treatment is prosthetic replacement (hemiarthroplasty or total hip arthroplasty) to allow immediate weight-bearing and minimize perioperative morbidity.
Conversely, in the young adult population (typically defined as physiologically less than 60 to 65 years of age), femoral neck fractures are predominantly the result of high-energy trauma, such as motor vehicle collisions, falls from significant heights, or high-velocity athletic injuries. In this demographic, joint preservation through meticulous Open Reduction and Internal Fixation (ORIF) is the absolute gold standard. The native hip joint is biomechanically superior to any arthroplasty construct, and preserving the patient's own femoral head is paramount for ensuring long-term functional survivorship and allowing a return to high-impact activities. However, the margin for error in young femoral neck ORIF is virtually nonexistent. The tolerance for malreduction in these fractures is zero.
Failure to achieve a perfect, anatomic reduction significantly increases the risk of mechanical failure, nonunion, and osteonecrosis. Historically, there was a reliance on closed reduction and percutaneous pinning; however, modern orthopedic traumatology recognizes that an inadequate closed reduction must never be accepted. If an anatomic closed reduction cannot be achieved and confirmed on multiple fluoroscopic views, the surgeon must immediately transition to an open approach. The imperative is to restore the precise spatial orientation of the femoral head relative to the neck, re-establish the cortical buttress, and apply a biomechanically optimized, length-stable fixation construct.
Furthermore, the timing of surgical intervention in young femoral neck fractures remains a critical topic of debate and investigation. While historic dogma mandated emergent surgical decompression and fixation within six hours to mitigate the "tamponade effect" of the intracapsular hematoma, contemporary evidence suggests that while early surgery (within 12 to 24 hours) is optimal for general physiologic recovery and pain control, the quality of the anatomic reduction and the stability of the fixation construct are the most profound independent predictors of successful union and femoral head survival. Therefore, surgery should be performed as urgently as possible, but only when the appropriate surgical team, equipment, and optimal operating room conditions are available to guarantee a flawless execution of the procedure.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the vascular anatomy of the proximal femur is the foundational prerequisite for performing joint-preserving surgery of the hip. The arterial supply to the femoral head is derived primarily from the medial circumflex femoral artery (MCFA) and, to a lesser extent, the lateral circumflex femoral artery (LCFA). The MCFA gives rise to the critical retinacular vessels, which ascend along the posterior and superior aspects of the femoral neck within the synovial reflection. These vessels penetrate the femoral head just distal to the articular cartilage. Because this blood supply is entirely retrograde, any displaced fracture of the femoral neck physically shears these ascending vessels, rendering the femoral head acutely ischemic. The ligamentum teres provides a negligible blood supply to the adult femoral head via the foveal artery, which is insufficient to maintain viability in the event of MCFA disruption. Therefore, the surgical approach and capsulotomy must be meticulously designed to avoid further iatrogenic injury to the posterior-superior retinacular vessels.
The biomechanical environment of the femoral neck is dictated by the orientation of the fracture line and the vector of forces acting across the hip joint during physiologic loading. The Pauwels classification, originally described in 1935, remains the most highly relevant biomechanical framework for preoperative planning and implant selection. Pauwels Type I fractures exhibit a fracture line of less than 30 degrees relative to the horizontal plane. In these patterns, compressive forces predominate across the fracture site, making them inherently more stable and often amenable to parallel cannulated screw fixation. Pauwels Type II fractures (30 to 50 degrees) experience a mixture of shear and compressive forces. Pauwels Type III fractures, characterized by a vertical fracture line exceeding 50 degrees, are highly unstable. In these vertical patterns, high shear forces predominate, attempting to drive the femoral head into varus collapse and retroversion. Biomechanical data unequivocally demonstrate that parallel cannulated screws are insufficient to neutralize the shear forces inherent in Pauwels III fractures, mandating the use of fixed-angle devices.
Beyond the coronal orientation of the fracture, the assessment of sagittal plane comminution is equally critical. High-energy trauma frequently results in significant posterior comminution of the femoral neck. The posterior cortex acts as the primary structural buttress against retroversion. When this buttress is compromised, the femoral head is highly susceptible to posterior tilt and shortening during the healing phase, even with seemingly robust internal fixation. Preoperative advanced imaging is highly recommended to assess the degree of this posterior comminution, as its presence dictates the necessity for length-stable fixation constructs that can act as internal fixators rather than relying on cortical apposition for stability.

Furthermore, the concept of femoral neck shortening has gained significant attention in recent biomechanical and clinical literature. Standard sliding hip screws and partially threaded cannulated screws rely on dynamic compression along the axis of the femoral neck to achieve secondary bone healing. However, in the setting of comminution or osteopenia, this uncontrolled sliding leads to profound shortening of the femoral neck. Shortening greater than 5 millimeters significantly alters the biomechanics of the hip joint, decreasing the abductor lever arm, reducing resting tension on the gluteus medius, and resulting in a chronic Trendelenburg gait, diminished functional outcome scores, and accelerated joint degeneration.
Exhaustive Indications and Contraindications
The decision-making matrix for the treatment of femoral neck fractures requires a synthesis of patient-specific physiologic factors, fracture morphology, and injury context. Open Reduction and Internal Fixation is not a universally applicable procedure; rather, it is a highly targeted intervention designed for specific clinical scenarios where the benefits of joint preservation outweigh the substantial risks of fixation failure.
The absolute primary indication for ORIF of a femoral neck fracture is a displaced intracapsular fracture in a physiologically young, active patient (generally under the age of 60-65). In this cohort, the native hip joint must be preserved to accommodate high-demand physical activities and to avoid the multiple revision arthroplasties that would inevitably be required over the patient's lifespan if a primary joint replacement were performed. Additionally, ORIF is strictly indicated in any patient, regardless of age, presenting with a nondisplaced or valgus-impacted femoral neck fracture, as these inherently stable patterns have a high rate of union and a low rate of AVN when protected with in-situ fixation. In the setting of polytrauma, where the patient may have an ipsilateral femoral shaft fracture or multiple systemic injuries, early definitive fixation of the femoral neck with ORIF is indicated to facilitate mobilization and minimize the systemic inflammatory response, provided the patient is hemodynamically stable enough for the procedure.
Contraindications to ORIF are primarily centered around the inability of the patient to biologically heal the fracture, or the presence of pre-existing joint pathology that would render a healed native hip non-functional. Elderly, low-demand patients with displaced fractures are best served with arthroplasty. Chronological age is less important than biological age; a frail 60-year-old with severe medical comorbidities and osteopenia is a poor candidate for ORIF, whereas a robust, athletic 70-year-old may be considered for joint preservation. Severe pre-existing osteoarthritis or inflammatory arthropathy of the hip is an absolute contraindication to ORIF, as the joint is already compromised, and arthroplasty will simultaneously address both the fracture and the arthritis. Delayed presentation (typically greater than 3 to 4 weeks) of a displaced fracture is a relative contraindication to primary ORIF, as the incidence of AVN and nonunion rises exponentially; these patients may require primary arthroplasty or complex reconstructive osteotomies.
| Clinical Scenario | Indication Status for ORIF | Rationale and Biomechanical Considerations |
|---|---|---|
| Young Patient (<60 yrs), Displaced Fracture | Absolute Indication | Joint preservation is paramount. Native hip biomechanics are superior to arthroplasty for high-demand activities. |
| Nondisplaced / Valgus Impacted (Any Age) | Absolute Indication | High probability of union with in-situ fixation. Minimal risk of AVN due to intact retinacular vessels. |
| Ipsilateral Femoral Shaft Fracture | Absolute Indication | Requires fixed-angle construct (e.g., cephalomedullary nail or separate CHS + retrograde nail) to stabilize both injuries. |
| Elderly, Low-Demand, Displaced Fracture | Absolute Contraindication | High risk of nonunion/AVN. Arthroplasty allows immediate weight-bearing and definitive treatment. |
| Pre-existing Severe Hip Osteoarthritis | Absolute Contraindication | Preserving a painful, arthritic joint is illogical. Total Hip Arthroplasty addresses both pathologies simultaneously. |
| Delayed Presentation (> 3-4 Weeks) | Relative Contraindication | Extremely high risk of AVN/nonunion. Consider primary THA or valgus-producing proximal femoral osteotomy. |
| Pathologic Fracture (Malignancy) | Relative Contraindication | Poor healing potential. Arthroplasty with tumor prosthesis or cemented fixation is often required for immediate stability. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful femoral neck ORIF. The surgeon must not rely solely on standard anteroposterior (AP) and lateral radiographs. While these provide the initial diagnosis and Pauwels classification, a fine-cut computed tomography (CT) scan of the pelvis and proximal femur with 3D reconstructions is highly recommended, particularly in high-energy trauma. The CT scan allows for precise quantification of posterior neck comminution, identification of subtle basicervical extension, and assessment of the exact spatial displacement of the femoral head. This three-dimensional understanding dictates the reduction maneuvers required intraoperatively.
Preoperative templating must be performed to select the appropriate implant and determine its optimal trajectory. Using digital templating software on the uninjured contralateral hip, the surgeon should measure the native neck-shaft angle and femoral offset. When planning for a Compression Hip Screw (CHS), the angle of the side plate (typically 130, 135, or 140 degrees) must be chosen to match the native anatomy and allow the lag screw to sit perfectly centered within the femoral head in both the AP and lateral planes. The trajectory of the lag screw must be planned to achieve a tip-apex distance (TAD) of less than 25 millimeters, a recognized biomechanical threshold that significantly reduces the risk of implant cut-out. If a Proximal Femoral Locking Plate (PFLP) is planned, the surgeon must template the length of the plate to ensure adequate diaphyseal fixation distal to the fracture.
Patient positioning is a critical decision that influences both the ease of surgical access and the quality of intraoperative fluoroscopy. Two primary options exist: the dedicated fracture table and the flat radiolucent (Jackson or operating) table. The fracture table allows for precise application of skeletal traction and internal rotation, which can facilitate closed reduction or assist in maintaining an open reduction. It also provides unimpeded access for the C-arm to obtain true AP and cross-table lateral views without moving the patient's leg. However, the fracture table rigidly locks the patient's limb, severely limiting the surgeon's ability to dynamically manipulate the leg during a demanding open reduction.
Conversely, positioning the patient supine on a flat radiolucent table with a radiolucent bump under the ipsilateral sacrum allows the entire hemipelvis and lower extremity to be prepped and draped free. This "sloppy lateral" or fully free-draped supine position provides the surgeon with complete freedom to flex, extend, abduct, and rotate the hip to facilitate direct reduction through the anterior approach. The trade-off is that obtaining high-quality lateral fluoroscopic images requires the C-arm to be rolled in obliquely and the uninjured leg to be elevated or dropped out of the way, which can be cumbersome. Regardless of the table chosen, the C-arm must be positioned and tested prior to prepping and draping to guarantee that perfectly orthogonal AP and lateral views of the femoral head and neck can be obtained flawlessly.
Step-by-Step Surgical Approach and Fixation Technique
While a Watson-Jones (anterolateral) approach can be utilized, subcapital and transcervical femoral neck fractures are best visualized and most easily reduced through a Modified Smith-Petersen (Anterior) Approach. This approach exploits the true internervous plane between the femoral nerve territory (sartorius and rectus femoris) and the superior gluteal nerve territory (tensor fasciae latae). It provides unparalleled, direct en face visualization of the anterior femoral neck, which is critical for assessing the accuracy of the cortical reduction.
The patient is positioned, and a longitudinal incision is made beginning at the anterior superior iliac spine (ASIS) and extending approximately 10 to 12 cm distally toward the lateral aspect of the patella. The superficial fascia is incised, and the interval between the TFL laterally and the sartorius medially is developed. As the dissection deepens, the surgeon will encounter the ascending branches of the lateral femoral circumflex artery (LFCA) crossing the surgical field transversely within the fat pad overlying the rectus femoris. These vessels must be meticulously isolated, clamped, and cauterized or ligated to prevent massive postoperative hematoma. The direct head of the rectus femoris is identified, tagged, and released from its origin on the anterior inferior iliac spine (AIIS). The indirect head and the iliocapsularis muscle are reflected off the anterior hip capsule, and the iliopsoas tendon is retracted medially with a blunt Hohmann retractor.
A formal capsulotomy is then performed to expose the fracture and evacuate the fracture hematoma, which often sits under significant tension. A T-shaped capsulotomy is most frequently utilized, with the longitudinal limb running parallel to the axis of the femoral neck and the transverse limb parallel to the intertrochanteric line. Crucially, the surgeon must strictly avoid posterior extension of the capsulotomy at the base of the femoral neck to prevent iatrogenic transection of the vital retinacular vessels.
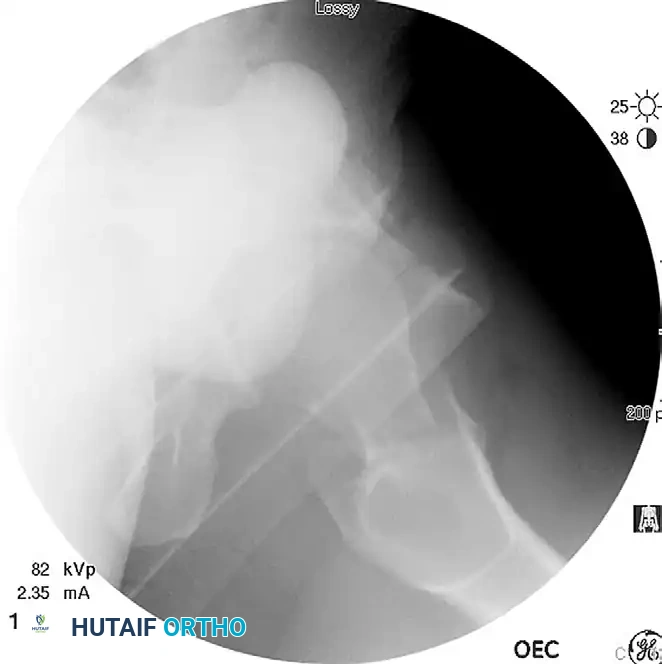
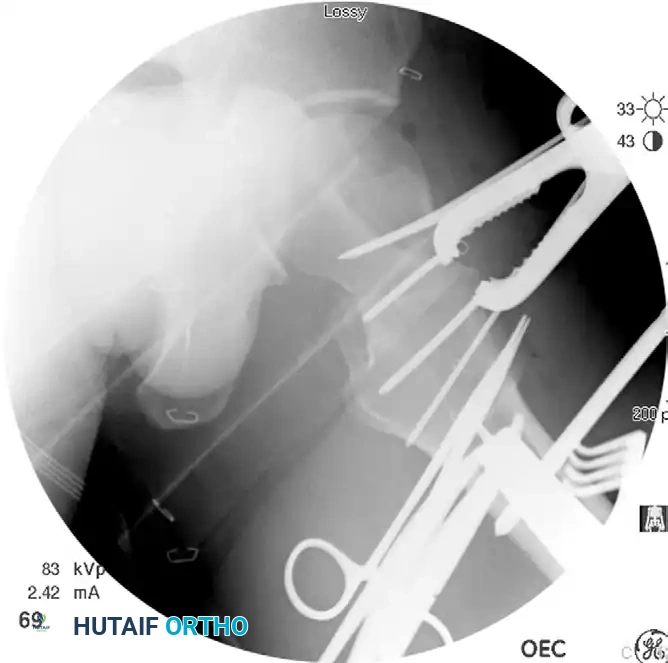
Once the fracture is exposed, the reduction sequence commences. Direct visualization allows for precise manipulation. Distal control is achieved by placing a 5.0-mm Schanz pin into the proximal femoral diaphysis through a separate lateral stab incision, attaching a T-handle to provide a powerful lever for controlling rotation and translation of the shaft. Proximal control is obtained by inserting two 2.0-mm threaded Kirschner wires (joysticks) into the anterior aspect of the femoral head. Using Cobb elevators and ball-spike pushers, the surgeon anatomically aligns the anterior cortical edges. Once perfect alignment is achieved visually and fluoroscopically, a Farabeuf or Jungbluth reduction clamp is applied across the fracture to compress the fragments and rigidly hold the reduction while definitive hardware is placed.
The choice of internal fixation depends heavily on the Pauwels angle and the presence of comminution. For stable, low-shear fracture patterns (Pauwels I and II) without significant comminution, Cannulated Screw Fixation is appropriate. Through a separate lateral approach, three 6.5-mm or 7.3-mm partially threaded cannulated screws are inserted in an inverted triangle configuration. The inferior screw must rest directly on the calcar femorale, and the posterior screw must sit adjacent to the posterior cortex to maximize biomechanical stability. Washers must be used to prevent screw head punch-out through the lateral cortex.

For highly unstable, vertical shear patterns (Pauwels III) or basicervical fractures, a Compression Hip Screw (CHS) with a derotational screw is mandatory. A guide pin is placed centrally into the femoral head, and a superior partially threaded cannulated screw is inserted first to prevent rotation during CHS reaming. The CHS lag screw is then inserted, followed by the application of the side plate to the femoral shaft. This fixed-angle construct is vastly superior in resisting vertical shear forces compared to parallel screws.


In cases of severe femoral neck comminution where length-stable fixation is paramount to prevent shortening and abductor dysfunction, a Proximal Femoral Locking Plate (PFLP) may be utilized. The locking construct acts as an internal fixator, rigidly holding the anatomically reduced femoral neck and preventing collapse into varus and retroversion. The locking screws provide angular stability independent of bone quality, making this an excellent choice for complex, comminuted patterns in young patients.

Complications, Incidence Rates, and Salvage Management
Despite flawless surgical execution, intracapsular femoral neck fractures carry a notoriously high complication rate, frequently leading to revision surgery. The hostile biological environment and the immense mechanical forces crossing the hip joint conspire to make these injuries incredibly difficult to heal. The two most devastating complications are osteonecrosis (AVN) and nonunion.
Osteonecrosis occurs due to the disruption of the retrograde blood supply at the time of injury. In meta-analyses of young patients, the overall incidence of osteonecrosis is approximately 20% to 25%, rising significantly with the degree of initial displacement. The pathophysiology involves ischemia of the subchondral bone, leading to trabecular collapse and eventual secondary osteoarthritis. While some young patients with AVN may tolerate the condition if the collapse is minimal, the majority will eventually require conversion to a Total Hip Arthroplasty (THA). The role of routine capsulotomy in preventing AVN by relieving the tamponade effect remains controversial; however, most trauma surgeons advocate for it during an open approach, provided the retinacular vessels are meticulously protected.
Nonunion of the femoral neck is driven by mechanical instability, poor biology, or a synergistic combination of both. The nonunion rate ranges from 10% to 15%, with significantly higher rates observed in Pauwels Type III vertical shear fractures. Nonunion typically presents with persistent groin pain and progressive varus collapse visible on serial radiographs. The primary defense against nonunion is an absolute anatomic reduction and the selection of a length-stable, fixed-angle implant. If a nonunion occurs in a young patient with a viable (non-necrotic) femoral head, a salvage procedure such as a valgus-producing intertrochanteric osteotomy is indicated. This procedure reorients the fracture line to a more horizontal position, converting shear forces into compressive forces to stimulate healing.
| Complication | Estimated Incidence | Primary Pathophysiology | Salvage Management Strategy |
|---|---|---|---|
| Osteonecrosis (AVN) | 20% - 25% (Displaced) | Disruption of MCFA retinacular vessels; ischemia and subchondral collapse. | Early: Core decompression (controversial). Late/Collapsed: Total Hip Arthroplasty (THA). |
| Nonunion | 10% - 15% | Mechanical instability (shear forces), inadequate reduction, poor biological envelope. | Viable Head: Valgus-producing proximal femoral osteotomy. Necrotic Head: THA. |
| Femoral Neck Shortening | 30% - 60% (>5mm) | Dynamic compression along the fracture axis, especially with comminution. | Symptomatic management, shoe lifts. Prevention via length-stable implants is key. |
| Implant Failure / Cut-out | 5% - 10% | Poor implant trajectory (TAD > 25mm), osteopenia, failure to achieve anatomic reduction. | Revision ORIF with bone grafting (if early), or conversion to Arthroplasty. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following femoral neck ORIF must be meticulously tailored to the patient's age, bone quality, fracture pattern, and the biomechanical robustness of the fixation construct. Unlike arthroplasty, where immediate full weight-bearing is the norm, joint preservation surgery requires a delicate balance between protecting the fixation to allow for biological healing and mobilizing the patient to prevent systemic complications.
Phase 1 (Weeks 0 to 6) focuses on immediate postoperative protection and complication prevention. In young patients with high-energy trauma, weight-bearing is strictly restricted to touch-down weight bearing (TDWB) or flat-foot weight bearing (allowing the weight of the leg only, approximately 20 pounds) using crutches or a walker. This restriction is crucial to prevent early mechanical failure of the implant or varus collapse of the femoral head. Deep vein thrombosis (DVT) prophylaxis is mandatory, typically utilizing low-molecular-weight heparin or direct oral anticoagulants for a minimum of 28 to 35 days. Active and passive range of motion (ROM) of the hip, knee, and ankle is initiated immediately to prevent capsular contracture, with specific avoidance of extreme internal rotation or forced flexion that might stress the anterior capsule repair.
Phase 2 (Weeks 6 to 12) marks the transition to progressive loading, contingent upon radiographic evidence of early callus formation or maintenance of fracture alignment without hardware complication. Weight-bearing is gradually advanced from TDWB to partial weight-bearing (PWB), and eventually to full weight-bearing as tolerated (WBAT) by the end of the 12th week. Physical therapy intensifies, focusing on isometric abductor strengthening, core stability, and gait normalization. Aquatic therapy can be highly beneficial during this phase to allow for buoyancy-assisted movement and strengthening.
Phase 3 (Months 3 to 6 and beyond) focuses on the return to high-level function. Once full, painless weight-bearing is achieved and radiographs confirm solid clinical union, patients begin advanced closed-kinetic-chain exercises, proprioceptive training, and sport-specific drills. Return to high-impact sports or heavy manual labor is generally delayed until at least 6 months postoperatively, and only after a thorough clinical and radiographic evaluation confirms complete consolidation of the fracture and restoration of symmetric abductor strength.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of femoral neck fractures is heavily guided by landmark clinical trials and extensive meta-analyses that have shaped modern orthopedic protocols. A thorough understanding of this literature is essential for evidence-based practice.
The FAITH trial (Fixation using Alternative Implants for the Treatment of Hip fractures) is a monumental multicenter randomized controlled trial that compared sliding hip screws (CHS) to cancellous screws in the treatment of femoral neck fractures. The study demonstrated that while there was no significant difference in the overall rate of reoperation between the two groups, the sliding hip screw provided a distinct advantage in patients with displaced fractures, basicervical fractures, and those who were active smokers, significantly reducing the risk of AVN and nonunion in these high-risk cohorts. This trial solidified the preference for fixed-angle devices in unstable fracture patterns.
The timing of surgery has been extensively evaluated by researchers such as Bhandari and the FIX-IT study group. Historically, emergent surgery within 6 hours was advocated to prevent AVN. However, modern systematic reviews have demonstrated that while surgical delay beyond 24 hours is associated with increased mortality and systemic complications, a delay of up to 12 to 24 hours to optimize the patient medically and ensure the availability of an experienced surgical team does not significantly increase the rate of AVN or nonunion. The consensus guideline now dictates that surgery should be performed on an urgent basis, ideally within 24 hours, but never at the expense of a suboptimal surgical environment or an inadequately prepared patient.
Finally, the work of Zlowodzki and colleagues has brought critical attention to the phenomenon of femoral neck shortening following ORIF. Their research demonstrated that clinically significant shortening (greater than 5 mm) occurs in up to 66% of healed fractures treated with standard sliding devices. They
