Kyphectomy: Addressing Critical Skin Issues at the Apex of the Kyphosis

Key Takeaway
Looking for accurate information on Kyphectomy: Addressing Critical Skin Issues at the Apex of the Kyphosis? Kyphosis in spina bifida is a spinal deformity, typically occurring at the thoracolumbar, midlumbar, or lumbosacral junctions due to incomplete embryonic closure. This condition can lead to severe complications such as skin breakdown over the apex of the kyphosis, risking deep wound and central nervous system infections. It also causes gastrointestinal, genitourinary compromise, and thoracic insufficiency syndrome.
Introduction and Epidemiology
Kyphosis in the patient with myelomeningocele represents one of the most challenging deformities encountered in pediatric orthopedic surgery. The deformity typically manifests at the thoracolumbar junction, the midlumbar spine, or the lumbosacral junction. While the specific anatomic level of the kyphosis dictates the precise surgical vectors and fixation strategies required for repair, the underlying etiology—whether congenital, developmental, or paralytic—inevitably leads to devastating physiological consequences for the growing child.

The natural history of uncorrected severe kyphosis in spina bifida is characterized by relentless progression. The most immediate and life-threatening complication is the mechanical compromise of the soft tissue envelope. Skin breakdown over the prominent apex of the kyphosis is ubiquitous in neglected cases. This chronic ulceration serves as a nidus for deep wound infections, osteomyelitis of the apical vertebrae, and direct tracking of pathogens into the central nervous system, resulting in recurrent meningitis or ventriculitis.

Beyond the local tissue destruction, the profound sagittal imbalance induces secondary cascades across multiple organ systems. The severe forward flexion of the torso drastically reduces abdominal height, leading to mechanical compression of the viscera. This abdominal crowding compromises the gastrointestinal system, frequently resulting in diminished enteral absorption, chronic severe constipation, and feeding intolerance. Concurrently, the genitourinary system suffers from altered anatomical relationships, contributing to poor urinary drainage, vesicoureteral reflux, and the subsequent development of renal calculi. In extreme cases, the loss of abdominal height can cause disastrous kinking of the great vessels.
The secondary effects on pulmonary capacity are equally profound, producing a variant of thoracic insufficiency syndrome. Because the abdominal contents are forcefully pushed superiorly into the thoracic cage, diaphragmatic excursion is severely limited. This is often compounded by a compensatory secondary thoracic lordosis cephalad to the primary kyphosis, which further reduces intrathoracic volume.
Clinically, the C7 lateral plumb line demonstrates the upper torso falling drastically anterior to the pelvis. To maintain an upright sitting posture and interact with their environment, these children are forced to utilize their upper extremities as structural props. By pivoting on extended arms, the child attempts to unweight the diaphragm and recruit accessory muscles of respiration—a compensatory mechanism classically termed the "marionette maneuver." This obligate use of the upper limbs for truncal support and respiration effectively renders the child a "functional quadriplegic," severely limiting their ability to perform activities of daily living, transfer independently, or engage in normal developmental play. Bracing in this population is generally futile; it exacerbates skin pressure over the apex and ultimately fails to halt the progression of the deformity.
Surgical Anatomy and Biomechanics
A thorough understanding of the distorted embryology and resultant pathoanatomy is critical for safe surgical intervention. Embryologically, the notochord is normally covered dorsally by the progressive cephalic-to-caudal closure of the ectoderm. In myelomeningocele, this closure is incomplete, most frequently at the caudal end. This lack of posterior migration of the ectoderm surrounding the notochord leaves the neural placode exposed and vulnerable at birth.

This embryologic failure profoundly alters the development of the paraspinal musculature. Because the posterior elements (laminae and spinous processes) fail to form and close in the midline, the paraspinal muscles cannot migrate to their normal posterior position. Instead, they remain partially innervated and are trapped in a lateral and anterior position relative to the bony ridges of the dysplastic vertebrae. Biomechanically, this anterior displacement shifts the muscle action line anterior to the instantaneous axis of rotation of the spine. Consequently, muscles that normally function as spinal extensors act as powerful spinal flexors. With further growth and the assumption of an upright sitting posture, this anomalous musculature actively pulls the upper torso into a progressive kyphosis, a process further accelerated by gravity.

The osseous anatomy presents significant challenges for achieving a stable arthrodesis. The bony ridges located laterally in the area of the pedicle diastasis provide minimal bone stock for a posterior fusion mass. The midline defect from the original myelomeningocele repair is characteristically covered by a fragile, scarred dura that is separated from the overlying skin by only a tenuous, thin layer of subcutaneous tissue. This poor soft tissue envelope is frequently exacerbated by the patient's compromised nutritional status.
One of the few reliably formed vertebral structures in this patient population is the sacral ala. The preservation of sacral alar bone stock is therefore paramount, as it serves as the primary foundation for distal pelvic fixation during reconstructive procedures.

Vascular anatomy at the apex of the kyphosis requires meticulous attention. The great vessels (the descending aorta and the inferior vena cava) generally do not follow the acute contours of the kyphotic spine. Instead, they "bowstring" across the concavity of the kyphotic apex. This places the great vessels in perilous proximity to the anterior longitudinal ligament and the anterior vertebral bodies at the apex, significantly increasing the risk of catastrophic vascular injury during anterior subperiosteal dissection or apical vertebrectomy.
Indications and Contraindications
The decision to proceed with a kyphectomy is based on a combination of clinical deterioration, radiographic progression, and the failure of conservative measures. The primary goal of surgery is to re-establish sagittal balance, clear the abdomen for diaphragmatic excursion, and provide a stable spine that allows the soft tissue envelope to heal.

Progressive deformity that interferes with seating and positioning is a primary driver for surgical intervention. When the kyphosis exceeds 80 to 90 degrees, the biomechanical forces acting on the apex make skin breakdown inevitable.

Operative vs Non Operative Management
| Clinical Scenario | Management Strategy | Rationale |
|---|---|---|
| Recurrent Apical Skin Breakdown | Operative (Kyphectomy) | Chronic ulceration leads to osteomyelitis and CNS infection. Resection of the bony prominence is mandatory for soft tissue healing. |
| Loss of Sitting Balance / Functional Quadriplegia | Operative (Kyphectomy) | Correction of sagittal balance eliminates the need for the marionette maneuver, freeing the upper extremities for functional use. |
| Thoracic Insufficiency Syndrome | Operative (Kyphectomy) | Restoring abdominal height allows the viscera to descend, improving diaphragmatic excursion and pulmonary mechanics. |
| Mild Deformity (<50 degrees) with Intact Skin | Non-Operative (Observation/Seating Modifications) | Bracing is poorly tolerated, but custom wheelchair seating can distribute pressure and delay surgical intervention in mild cases. |
| Active Untreated CNS Infection | Contraindication (Delay Surgery) | Hardware placement in the setting of active meningitis or ventriculitis carries an unacceptably high risk of intractable deep surgical site infection. |
| Profound Medical Instability | Contraindication (Palliative Care) | Severe uncorrectable cardiopulmonary compromise may preclude the patient from surviving a massive reconstructive procedure. |
Pre Operative Planning and Patient Positioning
Comprehensive preoperative planning requires a multidisciplinary approach involving Orthopedic Surgery, Neurosurgery, Plastic Surgery, Urology, and Pulmonology. Nutritional optimization is critical; preoperative albumin and prealbumin levels must be evaluated and optimized, often requiring temporary enteral feeding supplementation, to mitigate the high risk of postoperative wound dehiscence.

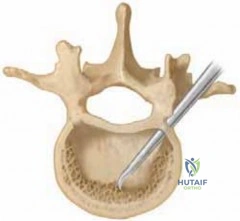
Advanced imaging is mandatory. High-resolution Computed Tomography (CT) with 3D reconstructions is utilized to map the dysplastic bony architecture, assess pedicle morphology for screw trajectory, and evaluate the integrity of the sacral ala and ilium for pelvic fixation.

Magnetic Resonance Imaging (MRI) of the entire neuraxis is required to evaluate the neural elements. The surgeon must identify the level of the functional spinal cord, rule out ascending syringomyelia, evaluate for a tethered cord, and assess the status of any Chiari malformation. The level of planned dural ligation must be carefully correlated with the patient's distal motor and sensory function to avoid iatrogenic neurologic deficit.

Patient positioning is a critical phase of the operation. The patient is typically positioned prone on a Jackson spinal table or custom-tailored bolsters. Extreme care must be taken to pad all bony prominences. The prominent apex of the kyphosis must be protected from any direct pressure during the initial stages of the procedure to prevent ischemic necrosis of the already compromised skin flaps. The abdomen must hang free to minimize intra-abdominal pressure, thereby reducing epidural venous engorgement and intraoperative blood loss.
Detailed Surgical Approach and Technique
The surgical execution of a kyphectomy is a massive undertaking that involves spinal exposure, neurosurgical dural ligation, apical vertebrectomy, deformity reduction, and complex pelvic fixation.
Incision and Exposure
The incision is tailored to the condition of the apical skin. Often, an elliptical incision is utilized to widely excise the ulcerated, adherent, or atrophic skin overlying the apex. The dissection proceeds through the subcutaneous tissues, which are often heavily scarred from previous closure attempts.

Subperiosteal dissection is carried out laterally along the dysplastic bony ridges. The surgeon must stay strictly subperiosteal to minimize bleeding and avoid inadvertent entry into the spinal canal. The laterally displaced paraspinal muscles are elevated off the rudimentary transverse processes and pedicles.
Dural Ligation and Cord Transection

Once the bony anatomy is exposed, the neurosurgical phase commences. The dural sac and neural placode are identified. In patients with no distal neurologic function, the dural sac and the non-functional distal spinal cord are ligated and transected. This is typically performed cephalad to the planned vertebrectomy site but strictly distal to any functioning nerve roots. A meticulous, water-tight closure of the proximal dural stump is achieved using non-absorbable sutures, often reinforced with a transfixing ligature and tissue sealants, to prevent postoperative cerebrospinal fluid (CSF) leaks.
Apical Resection

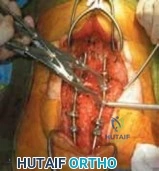
With the neural elements managed, the apical vertebrae are exposed. The dissection must proceed circumferentially around the vertebral bodies to be resected. A blunt, subperiosteal plane is meticulously developed along the anterior longitudinal ligament.

This is the most dangerous portion of the procedure, as the aorta and inferior vena cava bowstring directly across this space. Retractors are placed to protect the great vessels. An apical vertebrectomy (typically involving 1 to 3 vertebral bodies) and the adjacent intervertebral discs are resected using osteotomes, rongeurs, and a high-speed burr. The goal is to create a large closing-wedge osteotomy that will allow the spine to hinge posteriorly.
Reduction and Deformity Correction

Following the vertebrectomy, the deformity is reduced. This is achieved by extending the patient's torso and closing the anterior bony defect. This maneuver effectively shortens the spinal column, removing tension from the anterior soft tissues and vessels, while simultaneously correcting the severe sagittal kyphosis. The reduction must be controlled to prevent kinking of the proximal functional spinal cord.
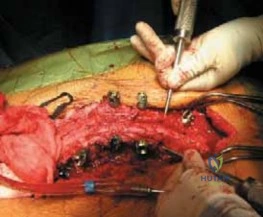
Instrumentation and Fixation

Rigid segmental fixation is paramount. Proximally, pedicle screws are placed into the thoracic and upper lumbar vertebrae. Distally, robust pelvic fixation is required due to the long lever arm of the construct and the poor bone quality. Techniques such as Sacral-Alar-Iliac (SAI) screws, traditional iliac screws, or the Luque-Galveston technique are employed. The rods are contoured to the corrected sagittal profile and secured. Compression is applied across the vertebrectomy site to enhance bony apposition and stability.
Bone Grafting and Closure

Extensive decortication of the remaining posterior elements and lateral gutters is performed. Copious amounts of structural allograft and local autograft (from the resected vertebrae) are packed into the fusion bed. Closure is frequently complex and may require the expertise of a plastic surgeon. If the primary skin cannot be closed without tension, local advancement flaps, rotational flaps, or regional muscle flaps (such as latissimus dorsi or gluteus maximus turnover flaps) are utilized to provide a robust soft tissue envelope over the hardware.
Complications and Management
The complication profile for kyphectomy in the myelomeningocele population is notoriously high, reflecting the severe systemic and local tissue compromises inherent to the disease process.

Wound breakdown and deep surgical site infections are the most common and devastating complications. The ischemic nature of the skin flaps, combined with poor nutritional status and proximity to the perianal region, creates a high-risk environment.

Hardware failure and pseudarthrosis are also frequent due to the massive biomechanical forces exerted on the construct and the inherently poor osteogenic potential of the dysplastic bone.
Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Prevention and Salvage Strategy |
|---|---|---|
| Wound Dehiscence / Necrosis | 15% - 30% | Prevention: Preop nutritional optimization, tension-free closure, flap coverage. Salvage: Serial debridement, negative pressure wound therapy (NPWT), delayed plastic surgery flap reconstruction. |
| Deep Surgical Site Infection | 10% - 20% | Prevention: Intrawound vancomycin powder, meticulous dead-space management. Salvage: Aggressive irrigation and debridement, retention of hardware (if stable) until fusion occurs, long-term suppressive IV antibiotics. |
| Pseudarthrosis / Hardware Failure | 10% - 25% | Prevention: Robust pelvic fixation (SAI screws), copious bone grafting, adequate anterior column support. Salvage: Revision instrumentation, extension of fusion, anterior column reconstruction if necessary. |
| Cerebrospinal Fluid (CSF) Leak | 5% - 15% | Prevention: Double-ligation of the thecal sac, use of dural sealants. Salvage: Over-sewing the leak, lumbar drain placement (if anatomically feasible), re-exploration and primary repair. |
| Massive Hemorrhage | Variable | Prevention: Careful subperiosteal dissection, protection of great vessels, use of antifibrinolytics (Tranexamic Acid). Salvage: Rapid blood product transfusion protocols, immediate packing, vascular surgery consultation for great vessel injury. |
Post Operative Rehabilitation Protocols
Postoperative care requires intensive monitoring, typically beginning
Clinical & Radiographic Imaging