Hemiresection Interposition Arthroplasty: Bowers Technique
Key Takeaway
The Bowers hemiresection interposition arthroplasty is a joint-sparing procedure designed to address distal radioulnar joint (DRUJ) pathology while preserving the triangular fibrocartilage complex (TFCC). By resecting the articular surface of the ulnar head and interposing soft tissue, surgeons can relieve pain and restore rotation. This technique is highly effective for rheumatoid arthritis, posttraumatic osteoarthritis, and unreconstructable ulnar head fractures, provided the TFCC remains competent.
Introduction to Distal Radioulnar Joint Arthroplasty
The distal radioulnar joint (DRUJ) is a highly complex diarthrodial articulation that, in conjunction with the proximal radioulnar joint, facilitates pronation and supination of the forearm. Pathologies affecting the DRUJ—ranging from rheumatoid arthritis to posttraumatic osteoarthritis—can severely debilitate hand and wrist function. Historically, complete excision of the distal ulna (the Darrach procedure) was the gold standard for DRUJ arthritis. However, complete resection often leads to radioulnar convergence, ulnar carpal translation, and profound weakness.
To mitigate the biomechanical consequences of complete ulnar head resection, William H. Bowers developed the Limited Ulnar Head Excision: Hemiresection Interposition Arthroplasty. This elegant, joint-sparing technique involves the partial resection of the ulnar head while meticulously preserving the ulnar styloid and the triangular fibrocartilage complex (TFCC). By maintaining the ligamentous tether between the radius, ulna, and carpus, the Bowers procedure preserves the functional kinematics of the wrist while eliminating the painful bone-on-bone articulation of an arthritic DRUJ.
Biomechanics and the Role of the TFCC
A profound understanding of DRUJ biomechanics is mandatory for any reconstructive wrist surgeon. The TFCC is the primary stabilizer of the DRUJ and the ulnocarpal articulation. It is a complex structure composed of the articular disc, the dorsal and volar radioulnar ligaments, the meniscus homologue, the ulnocarpal ligaments, and the extensor carpi ulnaris (ECU) tendon sheath.
The TFCC provides five critical biomechanical functions:
1. Radioulnar Stability: It provides a stable, dynamic radioulnar connection, preventing dorsal or volar subluxation of the distal ulna during forearm rotation.
2. Ulnocarpal Stability: It establishes a stable ulnocarpal connection, preventing ulnar translation of the carpus.
3. Load Transmission: It acts as a primary mechanism for transmitting axial forces from the hand to the forearm. In a neutral variance wrist, approximately 20% of the axial load is transmitted through the ulnocarpal joint via the TFCC, while 80% passes through the radiocarpal joint.
4. Suspensory Function: It functions as a suspensory ligament for the ulnar side of the carpus, tethering it to the distal radius.
5. Articular Extension: It provides an extended, smooth dividing surface for the proximal carpal row to articulate across the distal end of the forearm bones.
Clinical Pearl: The fundamental philosophy of the Bowers hemiresection interposition arthroplasty is that the TFCC must be preserved or reconstructable. If the TFCC is irreparably damaged or absent, the hemiresection technique offers no significant biomechanical advantage over standard ulnar shortening or complete resection techniques.
Indications and Contraindications
Patient selection is the most critical determinant of success in DRUJ arthroplasty. The Bowers procedure is highly specific in its applications.
Indications
The hemiresection interposition technique is indicated for the following conditions, provided the TFCC is intact or reconstructable:
* Unreconstructable Fractures of the Ulnar Head: Comminuted intra-articular fractures where open reduction and internal fixation (ORIF) is impossible.
* Ulnocarpal Impingement Syndrome: Specifically when associated with incongruity, chondromalacia, or arthritis of the DRUJ.
* Rheumatoid Arthritis: Involving the DRUJ, particularly in the early stages before complete destruction of the TFCC and carpal supination (caput ulnae syndrome) occurs.
* Posttraumatic Arthritis and Primary Osteoarthritis: Degenerative changes isolated to the DRUJ with a preserved ulnocarpal articulation.
* Chronic Painful TFCC Tears: Specifically, central perforations associated with DRUJ arthrosis where the peripheral stabilizing attachments remain competent.
Contraindications
- Incompetent or Absent TFCC: This is an absolute contraindication. Without a reconstructable TFCC, the remaining ulnar shaft will impinge on the radius (radioulnar convergence). In such cases, a Sauvé-Kapandji procedure or a Darrach resection is more appropriate.
- Severe Ulnar Positive Variance: Excessive ulnar length may require a formal ulnar shortening osteotomy rather than a simple hemiresection.
- Active Infection: Any active local or systemic infection precludes elective arthroplasty.
Preoperative Planning
Thorough clinical and radiographic evaluation is essential.
* Clinical Examination: Assess forearm rotation, grip strength, and DRUJ stability. The "piano key" sign (ballottement of the distal ulna) indicates DRUJ instability.
* Imaging: Standard posteroanterior (PA) and lateral radiographs of the wrist in neutral rotation are mandatory to assess ulnar variance and DRUJ congruity. Contralateral views are helpful for comparison.
* Advanced Imaging: A high-resolution MRI or CT arthrogram is highly recommended to definitively evaluate the integrity of the TFCC and the extent of chondral damage in the sigmoid notch.
Surgical Technique: Bowers Hemiresection Interposition Arthroplasty
The following step-by-step technique details the classic Bowers approach, incorporating meticulous soft tissue handling and dynamic stabilization of the ECU.
1. Patient Positioning and Approach
- Place the patient supine with the operative arm extended on a radiolucent hand table.
- Apply a well-padded proximal pneumatic tourniquet.
- Administer regional anesthesia (brachial plexus block) or general anesthesia based on patient and surgeon preference.
- Incision: Begin the longitudinal incision 5 to 7 cm proximal to the ulnocarpal joint, centered over the dorsal aspect of the distal ulna. Extend the incision distally, and at the level of the ulnocarpal joint, curve or angle the incision palmarward for 1 to 2 cm.
Surgical Warning: Meticulous dissection is required in the subcutaneous tissues to identify and protect the dorsal sensory branches of the ulnar nerve (DSBUN). Injury to these nerves can result in debilitating postoperative neuromas.
2. Retinacular Flap Elevation
- Expose the extensor retinaculum and the distal ulnocarpal area down to the deep fascia.
- Elevate the retinacular flaps to expose the underlying compartments. Raise a proximal flap based laterally (radially) and a distal flap based medially (ulnarward).
- These flaps are critical. They must be carefully developed as they will be used later for exposure, stabilization of the extensor carpi ulnaris (ECU), or augmentation of the TFCC. If they are not needed for stabilization, they can be reattached, used for coverage of the arthroplasty, or excised.
3. Management of the Extensor Carpi Ulnaris (ECU)
The ECU is a vital dynamic stabilizer of the ulnar aspect of the wrist. Its management depends on its intraoperative stability.
* If the ECU is stable: Reflect it laterally (radially) using subperiosteal dissection to expose the distal ulna.
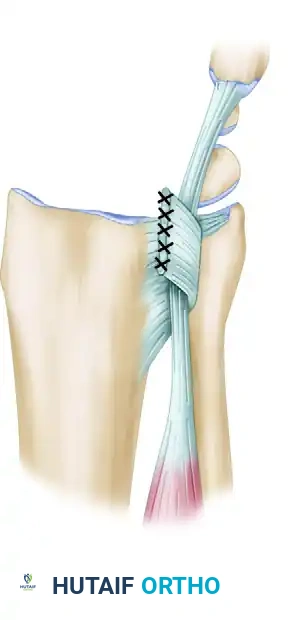
* If the ECU is unstable (subluxating): Mobilize the tendon distally to its insertion on the base of the fifth metacarpal. Utilize the previously raised proximal retinacular flap to fashion a stabilizing sling. Pass this fascial sling around the ECU tendon and suture it securely to the fibrous wall of the fourth extensor compartment.
Figure 1: Stabilization of the extensor carpi ulnaris with a retinacular sling. The flap is based on the fibrous wall between compartments four and five, preventing volar subluxation of the tendon during forearm rotation.
4. Joint Exposure and Hemiresection
- With the retinacular flaps elevated and the ECU managed, proceed to detach the radioulnar joint capsule.
- Release the capsule distally, laterally (radially), and proximally. Reflect the capsular tissue medially (ulnarward) to fully expose the articular surface of the ulnar head and the sigmoid notch of the radius.
- Using sharp osteotomes and rongeurs, meticulously remove the synovium, the ulnar head articular cartilage, and the underlying subchondral bone.
- The Resection: Remove all osteophytes around the sigmoid notch. Resect the subchondral bone of the ulnar head, but strictly preserve the ulnar styloid axis and its ligamentous attachments. The remaining ulnar shaft should resemble a smooth, tapering, 1-cm dowel.
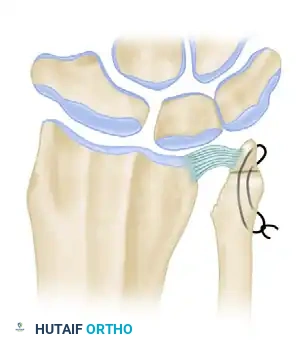
Figure 2: The ulnar head is resected to resemble a tapering dowel, meticulously preserving the ulnar styloid and the critical attachments of the TFCC.
5. TFCC Inspection and Impingement Assessment
- Inspect the triangular fibrocartilage carefully. Note that central perforations are common in degenerative conditions and do not require repair, provided the peripheral radioulnar ligaments remain intact.
- Dynamic Assessment: Place the wrist in ulnar deviation. Compress the radiocarpal joint and actively rotate the radial and ulnar shafts through full pronation and supination.
- Observe closely for any ulnocarpal abutment or radioulnar impingement. The resected ulnar shaft must not impinge on the radius or the carpus during dynamic loading.
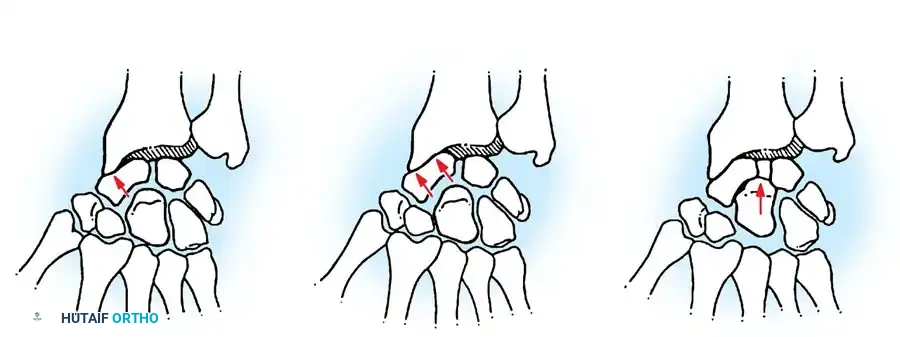
6. Addressing Impingement: Interposition vs. Shortening
If ulnocarpal abutment or radioulnar impingement is detected during the dynamic assessment, it must be addressed immediately to prevent postoperative pain and failure of the arthroplasty.

Figure 3 (Bowers A): Demonstration of impingement. Because the ulna is too long relative to the resection, the remaining ulnar shaft impinges on the stylocarpal ligament and the radius during rotation and ulnar deviation.
To correct this impingement, the surgeon has two primary options: Soft Tissue Interposition or Ulnar Shortening.
Option A: Soft Tissue Interposition (The "Anchovy" Technique)
If the impingement is mild to moderate, or if it cannot be definitively determined preoperatively, soft tissue interposition is the preferred method.
* Harvest a dispensable tendon (commonly the palmaris longus, a strip of the ECU, or the flexor carpi ulnaris).
* Roll the tendon into a "ball" or "anchovy."
* Pack this tendon ball tightly into the empty radioulnar space created by the hemiresection.
* Stabilize the interpositional graft by suturing it securely to the dorsal and volar radioulnar capsules. This biological spacer prevents bony contact and minimizes radioulnar convergence.
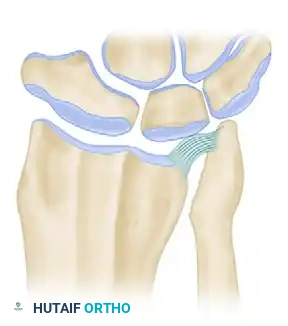
Figure 4 (Bowers B): Correction of impingement via soft tissue interposition. A tendon ball is sutured into the radioulnar defect, acting as a biological buffer.
Option B: Ulnar Shortening Osteotomy
If there is severe ulnar positive variance causing profound stylocarpal or ulnocarpal abutment that cannot be managed by interposition alone, a formal ulnar shortening procedure is required.
* Perform a transverse or oblique osteotomy of the ulnar shaft proximal to the hemiresection site.
* Shorten the ulna by the required amount (typically 2-4 mm) to achieve neutral or slightly negative variance.
* Fix the osteotomy rigidly with a dynamic compression plate.
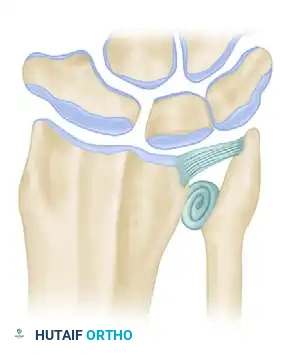
Figure 5 (Bowers C): Correction of impingement via ulnar shortening. The ulnar shaft is shortened proximally, decompressing the ulnocarpal space while maintaining the integrity of the TFCC and the hemiresection arthroplasty.
7. Closure
- Once impingement is resolved and the ECU is stabilized, thoroughly irrigate the surgical site.
- Repair the dorsal radioulnar capsule over the interpositional graft if possible.
- Close the extensor retinaculum, ensuring the ECU remains in its stabilized dorsal position.
- Deflate the tourniquet, achieve meticulous hemostasis, and close the subcutaneous tissues and skin in a standard fashion.
- Apply a bulky, sterile compressive dressing and a long-arm sugar-tong splint with the forearm in neutral rotation.
Alternative Ulnar Shortening Procedures
While the Bowers hemiresection is highly effective for DRUJ arthritis with a competent TFCC, surgeons must be familiar with alternative procedures for varying pathologies. Numerous ulnar shortening and resection procedures have been described in the literature:
- Darrach Resection: Complete excision of the distal ulna. Reserved for low-demand, elderly patients, or severe rheumatoid arthritis where the TFCC is completely destroyed. It carries a high risk of postoperative instability.
- Matched Resection (Watson et al.): A contoured resection of the distal ulna designed to match the curve of the radius, attempting to minimize convergence.
- Wafer Resection (Feldon et al.): Excision of the distal 2-4 mm of the ulnar articular cartilage and subchondral bone, leaving the styloid and DRUJ ligaments intact. Indicated for mild ulnocarpal abutment without severe DRUJ arthritis.
- Sauvé-Kapandji Procedure (Baldwin/Lauenstein): A combined distal radioulnar arthrodesis (fusion of the DRUJ) with the creation of a proximal pseudarthrosis of the distal ulna. This is the procedure of choice for DRUJ arthritis in young, high-demand patients or when the TFCC is irreparably deficient.
Postoperative Protocol and Rehabilitation
Successful outcomes following a Bowers procedure rely heavily on a structured, phased rehabilitation program.
Phase I: Immobilization (Weeks 0-3)
* The patient remains in a long-arm sugar-tong splint or a Muenster cast with the forearm in neutral rotation.
* Strict elevation and digital range of motion (ROM) exercises are encouraged immediately to prevent stiffness and reduce edema.
* Shoulder and elbow ROM exercises are mandatory.
Phase II: Early Mobilization (Weeks 3-6)
* The long-arm splint is transitioned to a short-arm removable wrist splint.
* Begin active and active-assisted forearm rotation (pronation/supination) and wrist flexion/extension under the guidance of a certified hand therapist.
* Avoid forceful gripping or heavy lifting, as the capsular tissues and interpositional graft are still healing.
Phase III: Strengthening (Weeks 6-12)
* Discontinue the splint for daily activities.
* Initiate progressive resistance exercises, focusing on ECU strengthening and dynamic DRUJ stabilization.
* Gradual return to normal activities and light labor.
Phase IV: Return to Full Activity (Months 3-6)
* Patients can typically return to heavy manual labor or sports by 4 to 6 months postoperatively, provided they have achieved pain-free, full range of motion and symmetric grip strength.
Complications and Pitfalls
While the hemiresection interposition arthroplasty is highly successful when indicated, complications can occur:
- Radioulnar Convergence: If the TFCC is incompetent or fails postoperatively, the remaining ulnar shaft will converge and impinge on the radius, causing severe pain and limited rotation. This is the most common cause of failure and usually requires revision to a Sauvé-Kapandji procedure.
- ECU Tendinitis or Subluxation: Failure to adequately stabilize the ECU during the initial exposure can lead to painful snapping of the tendon over the distal ulna. The retinacular sling technique described above is critical to preventing this.
- Stylocarpal Impingement: If the ulnar styloid is left too long, or if the patient has significant ulnar positive variance that was not addressed with shortening, the styloid may abut the triquetrum.
- Neuroma Formation: Injury to the dorsal sensory branch of the ulnar nerve during the surgical approach can result in a painful neuroma, which is often more debilitating than the original DRUJ arthritis.
Conclusion
The Bowers Limited Ulnar Head Excision with Hemiresection Interposition Arthroplasty remains a cornerstone technique in the armamentarium of the reconstructive wrist surgeon. By respecting the intricate biomechanics of the DRUJ and meticulously preserving the TFCC, surgeons can reliably relieve arthritic pain while maintaining the critical stability and load-bearing capacity of the ulnar wrist. Strict adherence to indications, precise surgical execution—particularly regarding ECU stabilization and impingement management—and structured postoperative rehabilitation are paramount to achieving excellent, long-lasting clinical outcomes.
📚 Medical References
- hemiresection interposition arthroplasty of the distal radioulnar joint, J Hand Surg 20A:944, 1995.
- DiBenedetto MR, Lubbers LM, Coleman CR: Long-term results of the minimal resection Darrach procedure, J Hand Surg 16A:445, 1991.
- Nanchahal J, Sykes PJ, Williams RL: Excision of the distal ulna in rheumatoid arthritis: is the price too high? J Hand Surg 21B:189, 1996.
- Newman RJ: Excision of the distal ulna in patients with rheumatoid arthritis, J Bone Joint Surg 69B:203, 1987.
- O’Donovan TM, Ruby LK: The distal radioulnar joint in rheumatoid arthritis, Hand Clin 5:249, 1989.
- Posner MA, Ambrose L: Excision of the distal ulna in rheumatoid arthritis, Hand Clin 7:383, 1991.
- Sanders RA, Frederick HA, Hontas RB: The Sauv-Kapandji procedure: a salvage operation for the distal radioulnar joint, J Hand Surg 16A:1125, 1991.
- Tulipan DJ, Eaton RG, Eberhart RE: The Darrach procedure defended: technique redefi ned and long-term follow-up, J Hand Surg 16A:438, 1991.
You Might Also Like